

Abstract
Background:
Disease surveillance and notification (DSN) is part of the Health Management Information System (HMIS) which comprises databases, personnel, and materials that are organized to collect data which are utilized for informed decision making. The knowledge about DSN is very important for the reporting of notifiable diseases.
Objective:
The aim of this study is to examine the awareness and knowledge of health-care workers about DSN, and availability of facility records in Anambra State, Nigeria.
Materials and Methods:
The study was a descriptive cross-sectional one in which relevant data were collected from health-care workers selected by a multistage sampling technique. Qualitative information was also elicited by key informant interviews, whereas an observational checklist, preceded by a desk review was used to examine the availability of facility records.
Results:
Although 89.8% of the health-care workers were aware of the DSN system, only 33.3, 31.1, and 33.7% of them knew the specific uses of forms IDSR 001, IDSR 002, and IDSR 003 (IDSR: Integrated Diseases Surveillance and Response), respectively. Knowledge of use of the various forms at the facility and local government area (LGA) levels were generally low, although the observational checklist revealed that IDSR 001 and IDSR 002 forms were predominantly found in primary health-care facilities. HMIS forms were less likely to be available in secondary health-care facilities (χ2=7.67, P=0.005).
Conclusions:
Regular training and retraining of concerned health-care workers on DSN at the LGA level is recommended. This should run concurrently with adequate and regular provision of IDSR forms, copies of the standard case definitions, and other necessary logistics to the health-care facilities by the local and state governments.
Keywords: Awareness, disease surveillance and notification, facility records, knowledge
INTRODUCTION
Surveillance according to the World Health Organization (WHO) is to watch over with great attention, authority, and often with suspicion.1 Disease surveillance is defined as the ongoing systematic collection, collation, analysis, and interpretation of health-care data, essential to the planning, implementation, and evaluation of public health-care practice, closely integrated with the timely dissemination of these data to those who need to know, in order that action may be taken.2,3 Disease surveillance depends on definition of case and recognition of illness, compilation of individual data, analysis, and reporting.4
Disease notification is a process of reporting the occurrence of disease or other health-related conditions to appropriate and designated authorities.5 Disease surveillance and notification (DSN) is part of the Health Management Information System (HMIS) which comprises databases, personnel, and materials that are organized to collect data which are utilized for informed decision making.6
Notifiable diseases are diseases that, by statutory requirements, must be reported to the public health-care authority in the pertinent jurisdiction when the diagnosis is made.7 Such diseases are deemed to be of sufficient importance to public health care to require that their occurrence be reported to authorities.8 The epidemic-prone diseases are recorded weekly, in addition to the monthly report. They include: Cholera, measles, cerebrospinal meningitis, yellow fever, and so on. Also included are the diseases targeted for eradication and elimination such as poliomyelitis, dracunculiasis, neonatal tetanus, leprosy lymphatic filariasis, and other diseases of public health importance like pneumonia and diarrhoea in under-fives, bloody diarrhoea, HIV/AIDS, tuberculosis, onchocerciasis, malaria, pertussis, hepatitis B, plague, and sexually transmitted infections (STIs).8 With the epidemiological transition, noncommunicable diseases such as diabetes mellitus and hypertension, tropical diseases like noma and buruli ulcer, emerging infectious diseases such as human influenza of the H5N1 subtype and severe acute respiratory syndrome (SARS), and other diseases under the International Health Regulation (IHR).8
The health-care facility which could be public or private is the first level for the generation of health-care facility-based data, and it also receives records from community-based health-care workers serving within its catchment area. The health-care facility staff collects data at this level, fills, and sends the forms on a weekly or monthly basis or immediately depending on the condition of disease or health care. These results are sent to the Local Government Primary Health Care Department (Monitoring and Evaluation Unit), which collates data from various health-care facilities in the locality and sends these to the State Ministry of Health (Epidemiology Unit). These data are analysed before transmission to the Federal Ministry of Health (Epidemiology and Planning Research and Statistics Unit) for national collation, analysis, records, and action.
The knowledge about the notification of disease is very important for the reporting of notifiable diseases. However, the knowledge of reporting requirements and responsibilities among health-care personnel has not been examined adequately as a cause of under-reporting.9 In Nigeria, the collection, collation, analysis, and interpretation of data in health-care facilities are often unsatisfactory, partly due to insufficient awareness among health-care personnel on the importance of this process.10 Studies on DSN have been carried out in Benin, Yobe but none has been conducted in Anambra State.9,10 The study will also contribute to research in DSN in Nigeria and in the West African Subregion. It is therefore in the light of the above that a study on the DSN in Anambra State is necessary. This study will no doubt identify the militating factors, proffer solutions, and help in making informed suggestions toward the formulation of policies and improvement of the DSN system in the state. The objective of this study therefore is to determine awareness and knowledge of health-care workers about DSN on one hand, and availability of facility records in Anambra State, Nigeria.
MATERIALS AND METHODS
The study area is Anambra State, Nigeria and is located in the Southeast geopolitical zone of the country. It has a population of 4,182,032 with 2,174,641 males and 2,007,391 females, and a population density of 869/km2.11 There are 21 local government areas (LGAs) and 177 communities in the state. The major language is Igbo, whereas the literacy level ranges from 48.6% to 84.1%.12 Awka, the state capital is about a 30-minute drive from the commercial nerve center of the state, Onitsha and 40 minutes from Nnewi, another major commercial center of the state, aptly referred to as the ‘Japan of Africa’.12 Two tertiary health-care institutions, the Anambra State University Teaching Hospital Awka, still in its rudimentary stage and the Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi are located in the state. There are 32 state government-owned general hospitals, 14 mission hospitals, 189 maternity homes, and about 600 private hospitals and clinics. Each of the 21 LGAs has an equitable distribution of primary health-care centres (210) and 166 health-care posts. There are five schools of nursing and midwifery and a school of health-care technology.13
This study design was a descriptive cross-sectional one. Health-care workers involved in DSN in the state health-care facilities were enrolled in the study. These include the facility heads, medical record officers, the DSN focal person, and at least two other staff members in select health-care facilities in the selected LGAs, and the DSN officers (DSNOs) of the selected LGAs. Also included was the state epidemiologist in charge of Disease Surveillance and HMIS in Anambra State. The health-care facilities were also assessed for the availability of DSN records.
The sample size for this study was determined using the formula,14 n=z2 pq/d2 where n = calculated sample size, z=standard normal deviate at 95% confidence interval=1.96, P = proportion of respondents that ever reported occurrence of an epidemic, q = the proportion of respondents that never reported occurrence of an epidemic, and d = precision level 5%=0.05. In a study in Yobe State, Nigeria, 79% of the respondents were found to have reported occurrence of an epidemic.9 Therefore, P=0.79, while q=1 – 0.79=0.21
![]()
An adjustment of the estimate of the sample size to cover for non-response rate was made by dividing the sample size calculated with a factor f, that is, n/f, where f is the estimated response rate.15 Therefore, anticipating a response rate of 95%, the minimum sample size required for the study was 254 health-care workers, and the study sample size = 254/0.95=270.
A multistage sampling technique was used to select six LGAs from the state (three urban and three rural LGAs). Then, nine health-care facilities were selected from each of these six LGAs and five health-care providers were selected from each of them. Data collection was done using interviewer-administered semi-structured health-care provider questionnaires, key informant interviews (KIIs), and a desk review and health-care facility observational checklist to examine the availability of facility records.
Quantitative data were analysed with the aid of the Statistical Package for Social Sciences (SPSS) version 16. Tests of statistical significance were carried out using Chi-square tests for proportions. The results were presented in the form of tables for easy appreciation. Qualitative data obtained from the recordings of the KIIs were transcribed verbatim, translated and field notes made, and the findings of desk reviews were reported.
Ethical approval was obtained from the NAUTH Ethical Committee (NAUTHEC), whereas the permission to conduct the study was obtained from the State Ministry of Health, Ministry of Local Government Affairs, and the Local Government Primary Health Care Department. In addition, written informed consent was obtained from all the respondents.
The study was however limited to notifiable infectious diseases only, because data were not collected on maternal and child health care, family planning, and noncommunicable diseases.
RESULTS
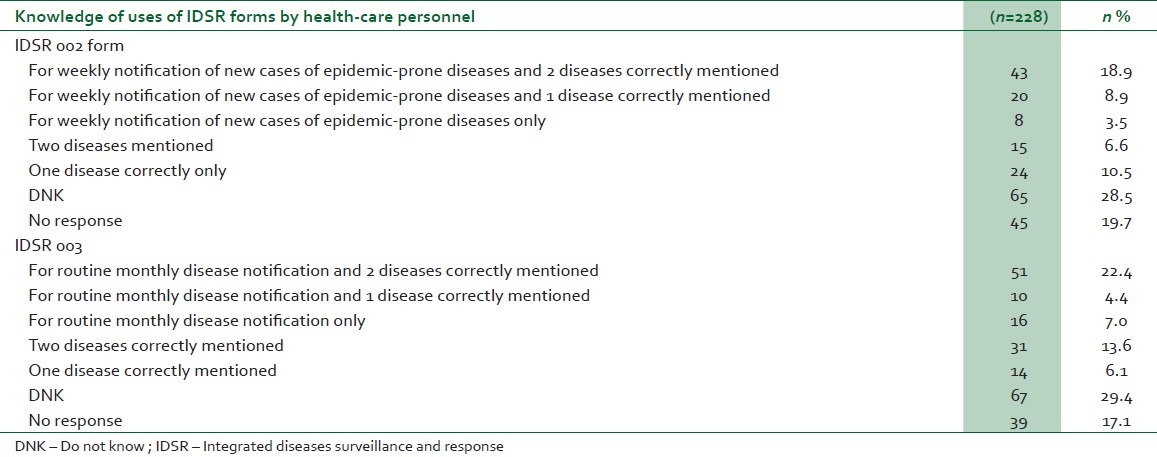
Tables 1 and 2 show that although 89.8% health-care workers were aware of the DSN system, only 33.3% of them knew that the form IDSR 001 (IDSR: Integrated Diseases Surveillance and Response) was used for immediate/case-based reporting, whereas 17.1% knew the correct use of the IDSR 001 form, mentioning correctly two diseases reported using it. Similarly, 31.1% knew that the IDSR 002 form was used for weekly notification of epidemic-prone diseases and 18.9% knew also at least two that could be notified using it. Furthermore, 33.7% said that the IDSR 003 form was used for monthly notification of diseases, whereas only 22.4% correctly mentioned two diseases notified using it.
Table 1.
Knowledge of use of IDSR forms among health-care personnel

Table 2.
Knowledge of use of IDSR forms among health-care personnel
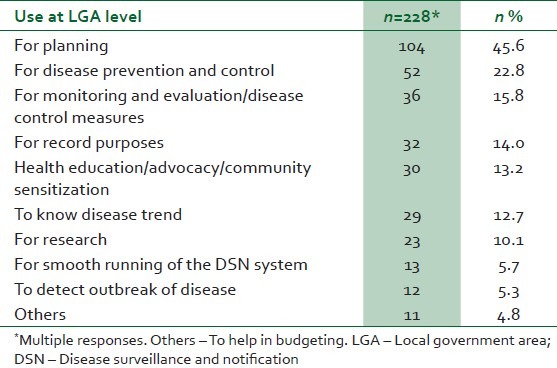
The knowledge of the subjects about the use of the IDSR forms at the facility and LGA levels are shown in Tables 3 and 4. The common uses of DSN records at the facility level include knowing changes in the trend of occurrence of disease (32.9%), prevention and control of disease (32.5%), statistics and planning (28.9%), and detecting and notifying outbreaks of disease (25.4%), whereas at the LGA level, the uses include planning (45.6%), prevention and control of disease (22.8%), monitoring and evaluation of disease control measures (15.8%), and purposes of record (14.0%).
Table 3.
Knowledge of health-care workers about use of DSN records at the facility level
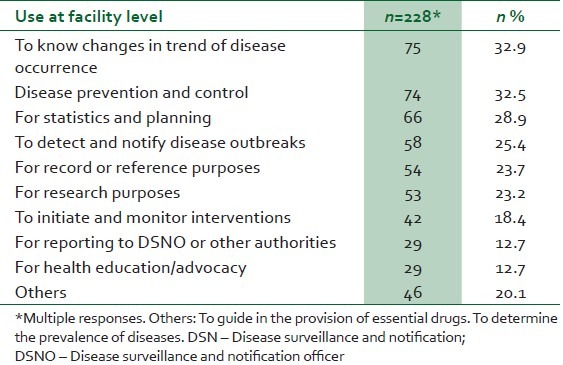
Table 4.
Knowledge of health-care workers about use of DSN records at the LGA level
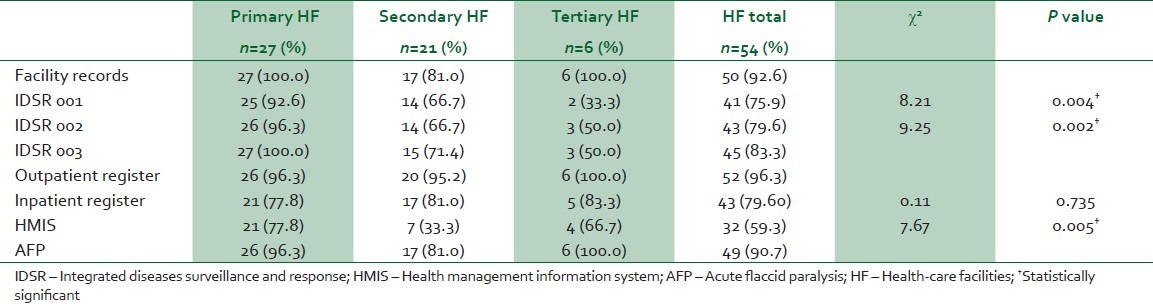
As shown in Table 5, the IDSR 001 and IDSR 002 forms were predominantly found in primary health-care facilities. However, the HMIS forms were less likely to be available in secondary health-care facilities (χ2=7.67, P=0.005).
Table 5.
Availability of facility records on observation
The KII finding shows that DSNOs have been sponsored to attend several workshops so far this year. However, most of them said there was no provision for in-service training to further their education. It was also reported that only the DSNOs attended these workshops, thus making it difficult for the other health-care workers to appreciate the principle of DSN and the role they are expected to perform. They also added that when such opportunities and sponsorships by the state and local government to further their education were offered, the wrong personnel had often been sent. One of them said, "If you no sabi person, no one go select you. Even those that are selected do not teach others when they come back and some of them are not selected for training on the areas where they do their work."
The desk review showed that there was no existing state-specific data or policies on the functional status of DSN system in Anambra State.
DISCUSSION
The findings of this study revealed that the awareness of DSN system for reporting the occurrence of disease in the country was high. Overall, 89.8% of the respondents were aware of the existence of the DSN system. This is contrary to the report by Oyegbite, where there was insufficient awareness of DSN among health-care personnel.10 It also differs from the finding of a study in northern Nigeria, which revealed that only 38.2% of health-care personnel studied were aware of the national disease surveillance system.16 This high awareness is probably because of the findings of the KII, where the DSNOs reported that they had been sponsored to attend several workshops on DSN. It was however reported that there were no such workshops for other health-care workers. This is not surprising, as previous training on DSN was done at the national and regional levels.17
In this study, despite the fact that the awareness of DSN was high, the depth of knowledge was poor when the knowledge of uses of the individual IDSR forms was considered. For instance, as regards the knowledge of the health-care workers about the respective forms and correct mentioning of two diseases under each of the categories, only 33.3% of the health-care personnel studied knew that IDSR001 form was used for immediate/case-based reporting, 31.1% knew that IDSR002 form was used for weekly notification of epidemic-prone diseases, whereas 33.7% knew that IDSR003 form was used for monthly notification of diseases of public health-care importance. Some studies showed that the knowledge of diseases that must be reported vary significantly from 39 to 96%.18–20 However, the findings of this study conform with those of other studies which showed poor knowledge of health-care personnel on reporting of infectious diseases and notifiable conditions.9,10,16,21 In Benin Nigeria for instance, only 11.9% of doctors studied had a good knowledge of DSN. This showed that lack of knowledge of reporting requirements seems to be a major factor affecting DSN. The resultant negative effect was that these health-care workers were unable to detect and notify the occurrence of diseases that have high case fatality rates and are of public health-care importance.
This study has only 63.0% of the 228 subjects being aware of the DSN system and having copies of the standard case definitions for notifiable diseases. This no doubt negatively affects the functionality of the DSN system. The presence of simple and standard case definitions has been emphasized by several authors as a prerequisite for an effective surveillance system.21,22
Majority (92.6%) of the health-care facilities had facility records. All the primary and tertiary health-care facilities had facility records, whereas 81% of the secondary health-care facilities had records. About 76, 79.6, and 83.3% of the facilities had IDSR 001, IDSR 002, and IDSR 003 forms, respectively. The finding of the quantitative survey is contrary to that of Bawa et al.,9 where only 8.0% of the facilities had IDSR forms. It also differs from that of Adindu,23 which showed that health-care facilities had inadequate supply of IDSR forms.
CONCLUSION
In conclusion, the awareness of the DSN system for reporting occurrence of disease in the country was high but the adequacy of knowledge of the use of the various IDSR forms was low perhaps because of unavailability of some of these forms. Therefore, there should be training and retraining programs on disease surveillance for health-care facility workers at the local government level and on a regular basis too. For data collection to be effective, the forms for reporting of disease should be readily available. Furthermore, there should be regular provision of IDSR forms, copies of the standard case definitions, transportation, as well as other necessary logistics to the health-care facility by the local and state governments.
ACKNOWLEDGMENTS
This work was part of a dissertation submitted to the West African College of Physicians in part fulfillment of the requirements for the award of the Fellowship of the College in Community Health. We remain indebted to all the Consultants in the Department of Community Medicine, Nnamdi Azikiwe University Teaching Hospital, Nnewi The authors would like to thank Mr Dan Umeh (the Anambra State Epidemiologist) and the Disease Surveillance and Notification Officers of the six LGAs studied (Mrs Ejimbe U, Mrs Onwuka E, Mr Emeh J, Mr Anaeto C, Mrs Okoye C and Mrs Nweke J) for their active support for this research.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.World Health Organization. Technical Report Series No. 593. 1976 [Google Scholar]
- 2.Last JM, editor. A dictionary of Epidemiology. 4th ed. London: Oxford University Press; 2001. Centres for Disease Control: Comprehensive plan for emergency surveillance. Atlanta, Georgia, 1996; pp. 174–5. [Google Scholar]
- 3.Communicable Disease Surveillance and Response (CSR) [Last accessed on 2009 May 19]. Available from: http://www.who.int/emc/surveill/index.html .
- 4.Eylenbosch WJ, Noah ND. Surveillance in health and disease. In: Last JM, editor. A dictionary of epidemiology. 4th ed. London: Oxford University Press; 2001. p. 175. [Google Scholar]
- 5.Whitehead M, William F. Legacy to the study of inequalities in health. Bull World Health Organ. 2000;79:86–7. [PMC free article] [PubMed] [Google Scholar]
- 6.Olumide EA. Ibadan: Kemta Publishers; 1997. Fundamentals of health service management for doctors and senior health workers in Africa; pp. 74–8. [Google Scholar]
- 7.Last JM. 4th ed. London: Oxford University Press; 2001. A dictionary of epidemiology; p. 125. [Google Scholar]
- 8.National Integrated Disease Surveillance and Response News of the Public Health Department Federal Ministry of Health, Abuja. 2002:1. [Google Scholar]
- 9.Bawa SB, Olumide EA, Umar US. The Knowledge attitude and practices of reporting of notifiable diseases among health workers in Yobe State, Nigeria. Afr J Med Sci. 2003;32:49–53. [PubMed] [Google Scholar]
- 10.Oyegbite KS. Abuja, Nigeria: Proceedings of the conference on National Health Management Information System; 1992. Health data in Nigeria; review of existing situation, form and format; pp. 42–4. [Google Scholar]
- 11.Osibogun A, Jaksic J, Idowu JA, Alausa OK, Oluwole FA. For better data, better utilized. World Health Forum. 1996;17:274–6. [PubMed] [Google Scholar]
- 12.Vol. 94. Abuja: 2006. National Population Commission. Provisional Census Results. Federal Republic of Nigeria Official Gazette, 15/5/07; p. 24. [Google Scholar]
- 13.2nd ed. Awka: 2007. Anambra State of Nigeria. State Economic Empowerment and Development Strategy (SEEDS) [Google Scholar]
- 14.Araoye MO. 2nd ed. Saw-mill, Ilorin: Nathadex Publications; 2008. Research methodology with statistics for health and social sciences; pp. 115–22. [Google Scholar]
- 15.Nigerian Population Commission. Nigeria: State and Local Government Demographic Profile, 1991.2010. Abuja. 1991 [Google Scholar]
- 16.Ofili AN, Ugwu EN, Ziregbe A, Richards R, Salami S. Knowledge of disease notification among doctors in government hospitals in Benin City, Edo State, Nigeria. Public Health. 2003;117:214–7. doi: 10.1016/S0033-3506(02)00021-5. [DOI] [PubMed] [Google Scholar]
- 17.Nasidi A, Ojo O, Udoh FA, Ayele T, Lecky M. Situation analysis of notifiable diseases in Nigeria (1990-1994) Niger Bull Epidemiol. 1995;4:2–29. [Google Scholar]
- 18.Chorba TL, Berkelman RL, Safford SK. Mandatory reporting of infectious disease by clinicians. J Am Med Assoc. 1989;262:3018–26. [PubMed] [Google Scholar]
- 19.Weiss BP, Strassburg MA, Fannin SL. Improving disease reporting in Los Angeles County: Trial and results. Public Health Rep. 1988;103:415–21. [PMC free article] [PubMed] [Google Scholar]
- 20.Konowitz PM, Petrossian GA, Rose DN. The underreporting of disease and physicians’ knowledge of reporting requirements. Public Health Rep. 1984;99:31–35. [PMC free article] [PubMed] [Google Scholar]
- 21.Federal Ministry of Health (Epidemiology Division, Lagos). National conference on Disease Surveillance, September. 1988 [Google Scholar]
- 22.Thacker SB, Gibson PR, Frederick L. Trowbridge, Surveilllance group.A method of evaluating systems of epidemiological surveillance 1988. World Health Stat Q. 1988;41:11–18. [PubMed] [Google Scholar]
- 23.Adindu AU. USA: University of Hull; 1995. The effect of incongruity on quality of health information system: Bama Nigeria.Primary Health Care case study (dissertation) [Google Scholar]