

Abstract
Introduction
Pure hyperextension thoracolumbar spinal fractures are unusual and occur primarily in patients with ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis due to the rigidity of the spine.
Material and methods
A 62-year-old female with osteoporosis presented with a significantly displaced fourth vertebral body fracture after being hit by a motorcycle. An imaging study showed widening of the vertebral height of L4 anteriorly with a horizontal fracture extending across the vertebral body. An in situ instrumented lumbar fusion from the second to fifth lumbar vertebrae was performed. Postoperatively, the patient complained of abdominal pain and difficulty in voiding. Computed tomography and intravenous pyelography showed that the right ureter was impinged between the fractured gaps of the vertebral body of L4.
Results
Solid bony union was obtained with surgical intervention.
Conclusions
This case reports a rare distractive extension injury in the lower lumbar spine with ureteral impingement. One should be aware of possible complications such as ureteral impingement following a pure hyperextension injury in the lower lumbar spine.
Keywords: Lower lumbar spine fracture, Thoracolumbar trauma, Ureteral injury, Extension mechanism, Fracture classification
Introduction
Most injuries of the thoracolumbar and lumbar spine occur secondary to hyperflexion or compression, often in combination with other forces, including rotation, distraction, or translation. Of the injury patterns, pure extension injuries of the thoracolumbar spine are very rare [3, 5, 8, 11]. Due to the rarity, extension injuries have not been classified into the categories of thoracolumbar or lumbar trauma. Trauma in ureter alone accounts for less than 1 % of all urologic injuries mainly because ureters are located deep in the retroperitoneum and are well protected by the psoas muscle, vertebrae and bony pelvis [13]. A rare case of a distractive extension injury with ureteral impingement by the 4th lumbar vertebral body is described and the significant features of this injury are discussed.
Case report
A 62-year-old female was transferred to the emergency department following a traffic accident with a motorcycle. At the time of arrival, the patient had severe back pain and multiple facial lacerations. Regarding past history, the patient had undergone vertebroplasty for L3 osteoporotic compression fracture 5 years ago at another institution.
The initial physical examination at the emergency department revealed no weakness of the lower extremity and severe tenderness in the lower lumbar spine without palpable defects between the posterior spinous processes. Neurologic examination was normal, and there were no associated injuries. The initial radiographs showed widening of the vertebral height of L4 anteriorly with a horizontal, wedge-shaped fracture extending across the vertebral body (Fig. 1a, b). A computed tomographic scan revealed distraction of the fractured body of L4 and anterior cortical disruption by distractive tensile force. A sagittal view of the T2-weighted magnetic resonance imaging demonstrated a horizontal fracture extending across the vertebral body at L4 with high-signal intensity consistent with hemorrhage and edema (Fig. 2a, b). On the fifth day after the accident, an in situ pedicle screw instrumentation with lumbar fusion from the second to fifth lumbar vertebrae was performed. Two days postoperatively, the patient complained of abdominal pain and difficulty voiding. Computed tomography and intravenous pyelography were performed immediately and showed a right congenital duplicated ureter impinged between the fractured gap of L4 (Fig. 3). The patient was referred to a urologist. Two months later, a laparoscopic ureteral resection and ureteroureterostomy with a double J catheter insertion was performed. Two years postoperatively, a solid bony union was obtained and there are no notable neurological or urological complications (Fig. 4a, b).
Fig. 1.
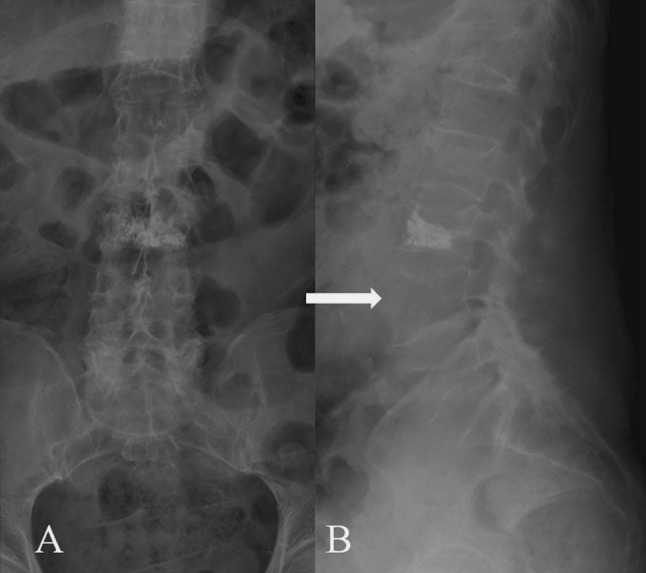
Plain radiographs of lumbar extension injury. Anteroposterior (a) and lateral (b) radiographs of the lumbar spine demonstrate widening of vertebral height of the fourth lumbar vertebra anteriorly with a horizontal fracture extending across the vertebral body (arrow)
Fig. 2.

CT scan of extension injury of the lumbar spine. CT scan of the injured level reveals a fracture through the anterior and middle columns (a). MR scan of a lumbar extension injury. T2-weighted sagittal MR scan demonstrated a horizontal fracture extending across the vertebral body at L4 with high signal intensity consistent with hemorrhage and edema (b)
Fig. 3.
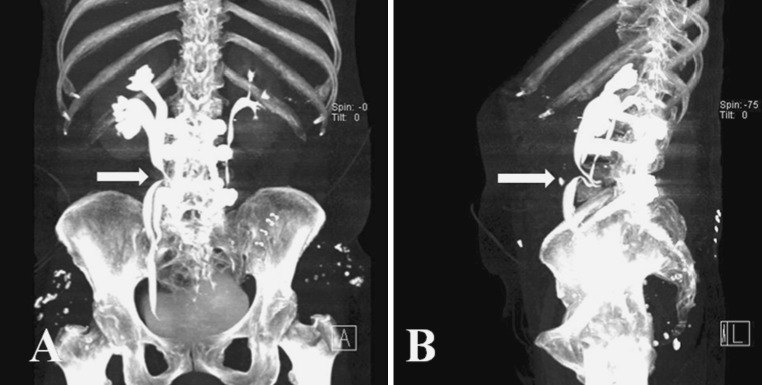
CT urography showed right mid-ureter entrapment at transverse fracture site of L4 body with obstructive hydronephrosis of right kidney (a Coronal view, b sagittal view)
Fig. 4.

Postoperative plain radiographs (a) and CT scan (b). Two year postoperatively, solid bony union was obtained
Discussion
This case reports a rare distractive extension injury in the lower lumbar spine with ureteral impingement, which was treated using fusion from second to fifth lumbar spine, laparoscopic ureteral resection and ureteroureterostomy. Extension injuries of the thoracolumbar and lumbar spine are rare [3, 5, 8, 11]. Due to its rare incidence, extension injuries have not been classified into the categories of thoracolumbar or lumbar trauma. Pure hyperextension thoracolumbar spinal fractures occur primarily in patients with ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis due to the rigid nature of the spine [6, 7, 12]. Burke [3] described 4 of 154 patients with thoracolumbar lesions who presented with hyperextension injuries. In the Burke series of four patients with thoracolumbar extension fractures, all of the injuries occurred in the thoracic region, but not the lower lumbar spine, and resulted in complete and irreversible paraplegia. Hitchon et al. [7] reported that six thoracic and five lumbar fractures were found by reviewing the patient who had been diagnosed with ankylosing spondylitis. Nine fractures were associated with extension deformities and patients with ankylosing spondylitis are at risk of such injury, particularly extension fractures of the thoracic and lumbar spine.
Chance fractures are horizontal splitting fractures of the body and neural arch of the vertebrae, and the mechanism of the injury is flexion around an axis anterior to the anterior longitudinal ligament [4]. The entire vertebra is pulled apart by a strong tensile force. Characteristic radiographic findings include a marked widening of the interspinous distance on the anterior-posterior view. On the lateral view, an increase in the height of the intervertebral foramina and minimum compression of the anterior part of the fractured vertebra is observed [18]. In the present case, initial radiographs showed widening of the vertebral height of L4 anteriorly with a horizontal, wedge-shaped fracture extending across the vertebral body. Sagittal magnetic resonance imaging does not demonstrate disruption of the posterior elements, with the exception of a signal consistent with edema and hemorrhage. In addition, the posterior ligament complex is not disrupted in the surgical field. It shows that hyperextension is the mechanism of injury caused by direct impact on posterior aspect of lumbar spine. Furthermore, acute contraction of back muscles results in severe hyperextension in the lower lumbar spine. Therefore, it is believed that the mechanism of this injury depends on a pure hyperextension force.
The thoracolumbar injury classification and severity score (TLICS) was devised based upon the three most important injury characteristics [17]. According to this score system, patients scoring >5 points should be considered for surgical treatment [16]. Matejka [10] reported that 4 of 965 patients with fractures were satisfied with type B3 of Magerl’s [9] classification. All four patients underwent surgery by stabilization with internal fixation and posterior or combined fusion. In our case, the patient was evaluated according to the TLICS in which the distraction of the principal injury pattern scored four points and the MRI evidence of an indeterminate posterior ligamentous complex integrity scored two points. Subsequently, the patient was assigned to undergo surgical treatment.
It is important to understand the ureteral anatomic relationship, because ureter is located immediately lateral to the aorta on the left and the vena cava on the right and is also adjacent to the anterolateral aspect of the L4–L5 disc space. It can be found resting directly on the anterior longitudinal ligament in the groove between the vertebral body and the psoas muscle. Therefore, when lower lumbar fracture occurs, consideration of possible complications such as ureteral entrapment is recommended. Such complications should be included in the differential when a patient presents with pre- and postoperative flank pain. On admission, our patient showed no signs of ureter injury such as hematuria and voiding difficulty. If abdominal CT scan was done initially in the emergency department, we could have diagnosed the ureter situation earlier. Unfortunately, no further examination was done due to the lack of prominent symptoms or signs. We removed a foley catheter on postoperative day 2, after which the patient began to complain of abdominal pain and voiding difficulty. We then performed CT scan and intravenous pyeolography and found injuries to the ureter. Ureteral injuries are uncommon, seen in approximately 3 out of 10,000 trauma admissions, and occur more in penetrating than in blunt trauma [14]. Some authors reported iatrogenic ureteric injury during lumbar surgery, ureteric injury concomitant to chance fracture of children and pelvic fracture [1, 2, 14, 15]. However, a ureteric injury associated with a pure hyperextension injury in the lower lumbar spine has not been previously reported. Although the current case is extremely rare, it emphasizes the rarity of extension injuries in the lower lumbar with damages to the ureter.
Conclusion
The lower lumbar fracture with a pure hyperextension injury is an uncommon trauma by nature. Ureter impingement caused by fractured vertebral gaps is even more so. After operative treatment with fusion of lumbar vertebral body and urologic laparoscopic surgical intervention, we achieved a solid bony union and release of impinged ureter without notable neurological or urological complications. One should be aware of possible complications such as ureteral impingement following a pure hyperextension injury in the lower lumbar spine.
Conflict of interest
None of the authors have any potential conflict of interest.
References
- 1.Bjurlin MA, Rousseau LA, Vidal PP, Hollowell CM. Iatrogenic ureteral injury secondary to a thoracolumbar lateral revision instrumentation and fusion. Spine J. 2009;9:13–15. doi: 10.1016/j.spinee.2008.12.009. [DOI] [PubMed] [Google Scholar]
- 2.Boszczyk BM, Krause P, Bolay H, Hohmann F, Mayer HM. Spinal epidural abscess following blunt pelvic trauma. Eur Spine J. 2000;9:80–84. doi: 10.1007/s005860050015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Burke DC. Hyperextension injury of the spine. J Bone Joint Surg. 1977;53:3–12. [PubMed] [Google Scholar]
- 4.Chance GQ. Note on a type of flexion fracture of the spine. Br J Radiol. 1948;21:452–453. doi: 10.1259/0007-1285-21-249-452. [DOI] [PubMed] [Google Scholar]
- 5.De Oliveira JC. A new type of fracture dislocation of the thoracolumbar spine. J Bone Joint Surg. 1978;60:481–488. [PubMed] [Google Scholar]
- 6.Ferree BA, Wieser M, Clarke RP. Hyperextension spinal fracture. Orthop Rev. 1989;18:1061–1064. [PubMed] [Google Scholar]
- 7.Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002;97:218–222. doi: 10.3171/spi.2002.97.2.0218. [DOI] [PubMed] [Google Scholar]
- 8.Jacobs RR. Bilateral fracture of the pedicles through the fourth and fifth lumbar vertebrae with anterior displacement of the vertebral bodies. J Bone Joint Surg. 1977;59:409–410. [PubMed] [Google Scholar]
- 9.Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S. A comprehensive classification of thoracic and lumbar injuries. Eur Spine J. 1994;3:184–201. doi: 10.1007/BF02221591. [DOI] [PubMed] [Google Scholar]
- 10.Matejka J. Hyperextension injuries of the thoracolumbar spine. Zentralbl Chir. 2006;131:75–79. doi: 10.1055/s-2006-921391. [DOI] [PubMed] [Google Scholar]
- 11.Miyasaki Y, Satomi K, Sugihara S, Tahara Y, Hayashi T, Ishii Y. Posterior fracture-dislocation of the thoracic spine without neurologic deficit. Spine. 1993;18:2351–2354. doi: 10.1097/00007632-199311000-00039. [DOI] [PubMed] [Google Scholar]
- 12.Nabeshima Y, Iguchi T, Matsubara N, Kinoshita S, Kurosaka M, Mizuno K. Extension injury of the thoracolumbar spine. Spine. 1997;22:1522–1525. doi: 10.1097/00007632-199707010-00020. [DOI] [PubMed] [Google Scholar]
- 13.Shenfeld OZ, Gnessin E. Management of urogenital trauma: state of the art. Curr Opin Urol. 2011;21:449–454. doi: 10.1097/MOU.0b013e32834b4a9e. [DOI] [PubMed] [Google Scholar]
- 14.Siram SM, Gerald SZ, Greene WR. Ureteral trauma: patterns and mechanisms of injury of an uncommon condition. Am J Surg. 2010;199:566–570. doi: 10.1016/j.amjsurg.2009.11.001. [DOI] [PubMed] [Google Scholar]
- 15.Slobogean GP, Tredwell SJ, Masterson JS. Ureteropelvic junction disruption and distal ureter injury associated with a Chance fracture following a traffic accident: a case report. J Orthop Surg (Hong Kong) 2007;15:248–250. doi: 10.1177/230949900701500227. [DOI] [PubMed] [Google Scholar]
- 16.Vaccaro AR, Lehman RA, Jr, Hurlbert RJ, et al. A new classification of thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous complex, and neurologic status. Spine. 2005;30:2325–2333. doi: 10.1097/01.brs.0000182986.43345.cb. [DOI] [PubMed] [Google Scholar]
- 17.Vaccaro AR, Zeiller SC, Hulbert RJ, et al. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005;18:209–215. [PubMed] [Google Scholar]
- 18.Weiss KS, Harris MB, Neitzschman HR. Radiology case of the month: unfortunate chance. Chance fracture at L3. J La State Med Soc. 1997;149:317–318. [PubMed] [Google Scholar]