

Abstract
Objective
To provide a contemporary estimate of the prevalence and incidence of rheumatoid arthritis (RA) work disability and examine its permanence over time.
Methods
Data were collected semiannually from 5,384 subjects with rheumatologist-diagnosed RA. We examined prevalence in subgroups formed by ~5-year disease duration intervals using data from subjects age ≤64 years who were employed at disease onset. Annual incidence was examined longitudinally among subjects who supplied data in 2003, 2004, or 2005, were employed at disease onset and in a year's first survey, and were age ≤63 years. For work disability permanence we used longitudinal data from all subjects who became work disabled and observed whether they later returned to work.
Results
Mean age of subjects was 52 years, 82% were female, 63% had more than a high school education, mean disease duration was 14 years, and mean Health Assessment Questionnaire score was 1.0. The prevalence of any premature work cessation was 23% in subjects with 1–3 years duration, 35% in those with 10 years, and 51% in those with ≥25 years RA duration. Arthritis-attributed work cessation was 14%, 29%, and 42%, respectively. Annual incidence of any premature work cessation was ~10% and arthritis-attributed work cessation incidence was ~6%. Thirty-nine percent of subjects who stopped working later returned to work.
Conclusion
Work disability prevalence in this sample was high (35% within 10 years disease duration), but may represent a decline from the 50% prevalence reported in 1987. Annual incidence of work disability was higher than prior studies, but the return to work rate was also higher.
INTRODUCTION
Work disability has been a major and costly effect of rheumatoid arthritis (RA) (1–8). In previous US studies, RA work disability prevalence in clinical samples has varied between 32% and 50% at 10 years of disease duration (4,6–8). The most widely quoted prevalence, 50% at 10 years of duration, was reported by Yelin et al in subjects residing in northern California (4). Annual incidence has been examined less often, but was 6.3% and 5.9%, respectively, in 2 US studies (4,7). Most US studies examining the prevalence and incidence of RA work disability are well over 10 years old, i.e., the 50% prevalence was from data collected retrospectively in the mid-1980s (4). Major changes have occurred since then, including improved RA treatment (9), possible milder disease course (10), and changes in the economy or in the nature of work, prompting speculation that the current prevalence and incidence may be much lower.
The main purpose of our study is to provide a contemporary estimate of the prevalence and incidence of RA work disability in the US. We also wished to make the prevalence and incidence figures we obtained as comparable as possible with figures from previous US studies (4,6–8). Because previous studies used various definitions, samples, and other methods (1,2), the differing prevalence figures (e.g., 32% and 50%) could stem from methodologic differences rather than improved treatment or other changes. To account for this we used work disability and employment definitions used in prior studies and similar sample age and employment history characteristics as well.
Given the prominence of the 50% work disability figure, we primarily used the definitions and sample characteristics used in the study by Yelin and colleagues (4). The definition of work disability in that study is any work cessation prior to age 65 years. Sixty-five years of age has until recently been the expected age for retirement in the US because a full Social Security pension was available then. This definition is considered valid because, as Yelin has pointed out, it is difficult for persons with disabling health conditions to decide to stop working without being influenced by their health (Yelin E: personal communication). However, this is controversial, and some believe the only acceptable definition is work cessation attributed to the disease being studied (11). Such a definition is likely to provide lower figures, and by using this definition, Wolfe and Hawley obtained the 32% prevalence figure (6). Therefore, we examined the impact of both definitions of work disability.
Our study's second purpose is to examine the permanence of work disability. Although work disability is often perceived as a permanent state, some work-disabled persons do return to work, e.g., 10% of subjects in the study by Yelin et al (4). Because of changes that have occurred since that study was conducted, people with RA may now be returning to work more often. We examined the proportion of subjects who returned to work after having ceased working and the proportion of subjects who stopped work repeatedly. The latter represents work instability, another measure of work disability (12).
In addition to major differences in employment rates, countries can have vastly different cultural norms and disability pension programs (1,13). Because of this, the focus of our comparisons was restricted to the US.
SUBJECTS AND METHODS
Data source
We used data from the National Data Bank (NDB) longitudinal study of RA outcomes (NDB-RA). The NDB-RA consists of a cohort of >10,000 subjects with rheumatologist-diagnosed RA who reside throughout the US. NDB subjects are added continuously and ~8% decline to participate per year. Subjects are recruited from 2 sources: patients recruited consecutively from rheumatologists' practices, 90% of which are private, and pharmaceutical company–sponsored registries. Data are collected from NDB subjects every 6 months by mail or online survey.
Subjects
NDB participants have always been queried about employment, but more extensive employment questions were added to the surveys between January 2002 and December 2005. Therefore, subjects initially eligible for our analyses were those who completed ≥1 survey during this time. We then excluded 2 categories of participants. The first was the 12% of participants who filled out short questionnaires containing no questions about employment; these individuals differed from our sample by age (65 versus 51 years), sex (23% versus 18% men), and education (42% versus 63% with education beyond high school). The second category of participants excluded consisted of those from pharmaceutical registries, because they differed from rheumatology practice subjects and likely differed from subjects in other work disability studies. Significant differences included functional limitation (mean Health Assessment Questionnaire [HAQ] score 1.1 versus 1.0) (14), disease duration (13.5 versus 12.0 years), sex (22% versus 18% men), and education (57% versus 63% with education beyond high school). To avoid expected retirement-related work cessation, as done in earlier studies, subjects in our analyses were age ≤64 years when work disability was assessed (4,7). Similar to Yelin and colleagues, we also restricted our samples to subjects who were employed at disease onset (4).
Definitions
Employment status
Employment was defined as any amount of paid work or unpaid work for an enterprise owned by the subject's family. This is the US Current Population Survey definition and the definition used by Yelin et al (4). Current employment status was assessed in 2 questions. First, subjects were queried about whether their main form of work was unemployed, paid work, retired, housework, student, or disabled. Second, they were asked whether they did any amount of employment work. We combined the responses to these questions so subjects were employed if they reported paid work as their main form of work, or, in cases where the main form of work was unemployed, retired, housework, student, or disabled, if they simultaneously reported doing some amount of employment work. In addition, to be considered employed, subjects also had to report weekly or monthly work hours. In each 6-month survey the employment status of 1–2% of subjects (1.7% of the total number of observations) could not be determined because of conflicting responses, and data from these observations were excluded.
Work disability
As in 2 prior studies (4,7), our primary definition of work disability was work cessation prior to age 65 years. We labeled this definition premature work cessation. The second definition was any work cessation prior to age 65 years that the subject attributed to arthritis. We labeled this definition arthritis-attributed work cessation. In the NDB survey, subjects are asked, “Did you ever retire early or permanently stop working because of your arthritis or other pain problem?” A positive response to this question defined arthritis-attributed work cessation.
Analysis
Subject characteristics
Data from each subject's first available survey were used to assess the demographic, disease, and employment characteristics of subjects eligible for analyses. These included age, sex, race, educational attainment, disease duration, functional limitation, employment status at disease onset as well as current, the work characteristics of subjects who were employed, and the main form of work of subjects who were not employed. Functional limitation was assessed by the HAQ (14). Full-time employment was ≥35 hours per week.
Prevalence of work disability
Cross-sectional data were used to calculate prevalence by disease duration; survival analysis was not possible because information on all subjects' dates of work cessation was not available. Previous studies discussed prevalence by 5-year intervals of disease duration. Therefore, we formed subgroups of subjects with data at a particular 5-year disease duration interval. All observations available for each subject in the eight 6-month surveys were used (Figure 1). Because some of the intervals had data from relatively few subjects, we increased the number of subjects who contributed data by broadening the intervals to 1–3 years, 4–6 years, 9–11 years, 14–16 years, 19–21 years, and ≥25 years. We used 1 observation per subject in each disease duration interval, provided the subject completed a survey at a disease duration spanned by the interval. If a subject completed a survey within 1 year of disease duration and a survey within 4 years of disease duration, the subject contributed to prevalence estimates in each of the 1–3-year and 4–6-year intervals. This was done to improve the precision of estimates within the disease duration intervals.
Figure 1.

Derivation of the full data set and the samples used to assess work disability prevalence, incidence, and permanence. RA = rheumatoid arthritis.
For the premature work cessation outcome, all subjects with data at a disease duration interval and who were employed at disease onset and age ≤64 years were eligible for analysis. Those who reported their current main form of work as unemployed, retired, housework, student, or disabled, and also reported no work hours, had premature work cessation. Percentages of subjects with premature work cessation were calculated for each disease duration interval. For the prevalence of arthritis-attributed work cessation, we determined which subjects with premature work cessation reported having stopped work due to arthritis. The number of subjects who stopped work due to arthritis was then used as the numerator in calculating the percentage of subjects in an interval with arthritis-attributed work cessation. We also calculated the proportion of the premature work cessation cases that were arthritis attributed.
Calculation of annual incidence of work disability
Longitudinal data were used to calculate annual incidence of work disability with and without arthritis attribution. A significant portion of subjects filled out surveys on a non-consecutive basis. Because of this, use of standard survival analysis methods was ruled out. Therefore, the annual incidence of work disability was calculated over 3 separate time periods: 2003, 2004, and 2005, in all eligible subjects (Figure 1). Eligible subjects for each of the 3 time periods were those who provided data in 3 consecutive surveys (initial and 2 followup) and in the initial survey were employed currently and at disease onset and were age ≤63 years. Employment status in the 2 followup surveys for the year was then examined. Subjects who were not employed at either followup survey were counted as premature work cessation incident cases. For incidence of arthritis-attributed work cessation, we determined which of the subjects with premature work cessation reported having stopped work due to arthritis. This number was used as the numerator in calculating the percentage of subjects in each time period with incident arthritis-attributed work cessation.
Work disability permanence
We used longitudinal data from the first 7 surveys on all subjects who were employed at disease onset to examine work disability permanence (Figure 1). Subjects who reported not working in a survey immediately subsequent to a survey in which they were working were identified as premature work cessation cases. Some subjects reported >1 episode of such work disability, so the number of subjects with >1 episode and the number of episodes they reported was observed. The work status of subjects with ≥1 episode of premature work cessation was then observed in subsequent surveys, and the proportion of subjects who later returned to work was calculated. We also examined the proportion of subjects with premature work cessation episodes who stopped work due to arthritis, as well as the portion of these subjects who later returned to work. Lastly, among the episodes of premature work cessation we calculated the proportions in which subjects reported being unemployed versus disabled because the former work status is more likely to be temporary than the latter.
RESULTS
Characteristics of subjects
A total of 5,384 subjects were available for analyses. At the first available observation, their mean ± SD age was 51.3 ± 9.1 years (range 19–64 years), 81.9% were women, 88.8% were white, and 63.4% had more than high school educational attainment (Table 1). Mean ± SD disease duration was 13.5 ± 9.5 years and mean ± SD HAQ score was 1.0 ± 0.7. Eighty-five percent of subjects had been employed at disease onset, whereas 58.5% of 5,279 subjects with employment status information at the first available survey were currently employed. Nearly three-quarters (74%) of these employed subjects worked full time, 41% held professional or managerial jobs, and 16% were self employed. Among subjects who were not employed, 7% were unemployed, 20% were retired, 28% were doing housework, 1.4% were students, and 43.5% were disabled.
Table 1.
Sample characteristics of subjects (n = 5,384) with data from the first available survey*
| Characteristic | Value |
|---|---|
| Age, mean ± SD years (range) | 51.3 ± 9.1 (19–64) |
| Women | 4,397 (81.9) |
| White | 4,692 (88.8) |
| > high school education | 3,329 (63.4) |
| HAQ score, mean ± SD† | 1.0 ± 0.7 |
| Employed at disease onset | 4,385 (84.6) |
| Currently employed‡ | 3,087 (58.5) |
| Full time (≥35 hours/week) | 2,118 (74.1) |
| Professional/managerial work | 1,882 (41.4) |
| Self employed | 463 (16.3) |
| Main form of work of subjects not currently employed‡ | 2,192 (41.5) |
| Unemployed | 144 (6.6) |
| Retired | 436 (20.4) |
| Housework | 599 (28.0) |
| Student | 31 (1.5) |
| Disabled | 930 (43.5) |
Values are the number (percentage) unless otherwise indicated.
Health Assessment Questionnaire (HAQ) measure of functional limitation (range 0–3, where 0 = no limitation) (n = 5,309).
Of subjects with employment status data in the first available survey.
Work disability prevalence
The prevalence of premature work cessation increased with years of disease duration, from 22.9% of 214 subjects with 1–3 years duration to 26.3% of 691 subjects with 5 years (range 4–6 years), 35.1% of 447 subjects with 10 years (range 9–11 years), 38.1% of 307 subjects with 15 years (range 14–16 years), 47.8% of 207 subjects with 20 years (range 19–21 years), and 51.1% of 374 subjects with ≥25 years of disease duration (Figure 2). The prevalence of arthritis-attributed work cessation also increased with disease duration but was somewhat lower, beginning with 13.6% in subjects with 1–3 years, increasing to 28.9% in subjects with 10 years, and ending at 42.2% in subjects with ≥25 years of duration. The portion of the premature work cessation cases attributed to arthritis also tended to increase with duration, from 59.2% of 1–3-year cases to 82.7% of ≥25-year cases.
Figure 2.
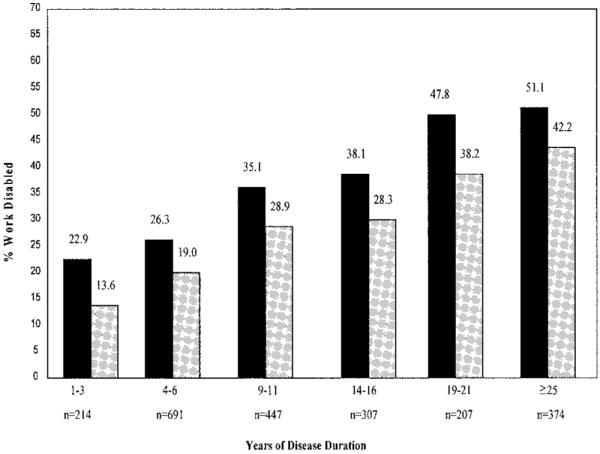
Work disability prevalence by ~5-year intervals of disease duration. All subjects were employed at disease onset. Solid columns represent all subjects age ≤64 years who were no longer employed. Shaded columns represent subjects ≤64 years of age who were no longer employed and attributed this to arthritis. N = subjects with data at a disease time period.
Annual incidence of work disability
The numbers of subjects contributing data to the 3 time periods were 908 in 2003, 828 in 2004, and 866 in 2005 (Table 2). An additional 158, 176, and 176 subjects, respectively, were eligible in the first phase of each time period, but did not supply followup data and therefore were excluded. The annual incidence of premature work cessation was 12.0% in 2003, 8.6% in 2004, and 9.4% in 2005. These figures were only slightly lower, at 10.9%, 7.8%, and 8.6%, respectively, among subjects age <62 years, the first age at which US citizens can take an early retirement Social Security pension. Arthritis-attributed work cessation incidence was lower and decreased slightly over the 3 years (i.e., from 6.7% in 2003 to 5.1% in 2004 and 4.8% in 2005).
Table 2.
Annual incidence of work disability*
| Premature work cessation, age ≤64 years, % | Arthritis-attributed work cessation, % | |
|---|---|---|
| Incidence | ||
| 2003 (n = 908) | 12.0 | 6.7 |
| 2004 (n = 828) | 8.6 | 5.1 |
| 2005 (n = 866) | 9.4 | 4.8 |
All subjects were employed in the first survey and at disease onset, and had data in the 2 subsequent 6-month surveys.
Permanence of work disability
Over the course of the 4-year period, 137 (39.1%) of 350 subjects with ≥1 episode of premature work cessation reported being employed again in a subsequent survey (Table 3). Twenty-three subjects stopped working twice and 4 subjects stopped working 3 times. Combined, 7.7% of subjects stopped working more than once, which is an indication of work instability. Of the 350 subjects with premature work cessation, 136 (38.9%) reported ≥1 episode of arthritis-attributable work cessation, and among these subjects, 32 (23.5%) later returned to work. In about a quarter (24.5%) of episodes of premature work cessation, subjects reported their main form of work as unemployed, and in 18.6% as disabled. Among subjects who later returned to work, 31.0% of episodes were reported as unemployed, and 10.1% as disabled.
Table 3.
Work disability permanence*
| Subjects | No. (%) |
|---|---|
| With premature work cessation | |
| 1 episode | 323 (92.3) |
| 2 episodes | 23 (6.6) |
| 3 episodes | 4 (1.1) |
| Total | 350 |
| Later returned to work | 137 (39.1) |
| With arthritis-attributed work cessation | |
| Total | 136 |
| Later returned to work | 32 (23.5) |
Data from any but the last survey included.
DISCUSSION
In this large US cohort of subjects with rheumatologist-diagnosed RA, a large portion (85%) were employed at disease onset. However, the proportion of subjects who were no longer employed was already substantial in the early disease period, i.e., 23% of subjects with 1–3 years of duration. This proportion increased with duration, such that 35% of subjects with 10 years of duration and 51% of subjects with ≥25 years of disease duration were no longer employed. Much of this premature work cessation type of work disability was arthritis related because the prevalence of arthritis-attributed work cessation was 14% among subjects with 1–3 years of disease duration and 29% among those with 10 years of disease duration.
The work disability prevalence of 35% among subjects with 10 years of disease duration is lower than the estimates obtained by Yelin et al (50%) (4) and Reisine et al (~40%) (7). Data were collected retrospectively in the mid-1980s in the former study and prospectively in the 1990s in the latter study. In a recent comparison of 1987 and 1998 cohorts of women with early-onset RA, Reisine and colleagues found no difference in the cumulative rate of work cessation over 4 years of followup (15). Likewise, there was no difference in the prevalence of work disability in our subjects with 1–3 years of RA and those in the study by Yelin and colleagues (4). Our study used the same work disability and employment definitions, but other methodologic differences exist and could account for the results (4,7).
RA work disability prevalence has generally been higher in European samples than in the US, perhaps due to differences in disability pension accessibility, labor market flexibility, and the link between employment and health insurance in the US (1). Therefore, results among countries are difficult to compare (1,13). However, in a recently published Swedish study, work disability prevalence by 10 years of disease duration was the same as in our study (35%) and similar by 15 years of duration (39% versus 38%) (13). These subjects had early-onset RA at study entry and 28% were already work disabled at entry. The arthritis-attributable work cessation prevalence from our study, 29% in subjects with 10 years of disease duration, is only slightly lower than the arthritis-attributed prevalence of 32% reported by Wolfe and Hawley, using data collected from Kansas residents in 1994 (6). Disease severity in the samples was similar; mean HAQ scores were 1.0 in both. The fact that the difference was small could be due in part to an advantageous employment situation in Kansas during the assessment period (6).
If there has in fact been a general decline in the prevalence of RA work disability, there are several possible explanations. The treatment of RA has been improving, including availability of more potent agents, earlier use of more potent agents, and use of combinations of agents (9). The possibility of a secular decline in the severity of RA has also been noted (10). External factors could play a role as well. Both the unemployment rate and the physical demand of jobs declined in the US between the mid-1980s and 2002–2005 (16,17). The annual incidence of work disability in our study was higher than in prior studies (~10% versus 6%) (4,7). The increase cannot be explained by work disability definition difference because we used the same definition as those studies. The arthritis-attributed work cessation incidence in our study was lower, at ~6% across the 3 annual time periods.
We also found that many cases of work disability were temporary. Thirty-nine percent of 350 subjects with an episode of premature work cessation later returned to work, which is considerably higher than the 10% figure in the study by Yelin et al (4). A quarter of subjects who ceased working reported their work status as unemployed, whereas only 2% of subjects in the study by Yelin and colleagues were unemployed in 1985 (4). We believe some of this difference is related to data collection methods. NDB data were collected prospectively every 6 months, whereas data in the other incidence studies were collected retrospectively or annually, so we probably identified more temporary periods of work cessation than those studies (4,7). Some of the excess incidence of work disability we found may have little relationship to RA; <40% of subjects attributed their work cessation to arthritis.
There are several limitations to our study. First, inability to use survival analysis does not allow precise determination of the time to work cessation for each subject. Second, the NDB-RA is a clinical cohort with most, if not all, subjects receiving care from rheumatologists. The sample therefore may not include as many persons with mild RA as a population-based sample. The mean HAQ score of our sample was 1.0, which represents moderate functional limitation (Wolfe F: personal communication). Because subjects with mild RA may not be fully represented in the NDB sample and may have less work disability, the actual RA work disability prevalence could be lower than we found. On the other hand, because NDB subjects have higher educational attainment and are more often white than the US population, and because these characteristics offer employment advantages, the actual RA work disability rate may be higher than we found.
Given the cost, it is unlikely that a population-based study of RA work disability will ever be conducted. The NDB-RA offers several advantages for the study of RA work disability. One advantage is that RA is well classified based on diagnosis by a rheumatologist. This is a major advantage because studies and experience show that subjects cannot accurately report arthritis diagnoses (18). Other advantages to the NDB-RA are its large number of subjects and its national scope. Lastly, recently collected detailed employment data were available.
We used mail or online surveys to collect data rather than personal interview, and due to the complexity of employment data, this can lead to misclassification of employment status. We excluded NDB participants whose employment status could not be determined because of conflicting data. We also evaluated possible misclassification in 2 ways. First, we calculated work disability prevalence in the subgroup of subjects whose employment data, i.e., all reports of employment status, hours and weeks worked, occupation, etc., were entirely consistent. Then we examined work disability in the subgroup where employment status was defined solely as a report of paid work as the main form of work. This more narrow definition excludes more marginal work and therefore focuses on more economically important employment. Work disability was more extensive in both subgroups. Among 185 subjects with entirely consistent data and 1–3 years of disease duration, 24% were work disabled, and among 413 subjects with 10 years duration, 37% were work disabled. Work disability prevalence by the employment definition of paid work as the main form of work was 25% in 214 subjects with 1–3 years of disease duration and 42% among those with 10 years duration. Incidence by this employment definition was lower, at 9% in 2003 and 7% in 2004 and 2005.
The question used to ascertain whether an episode of premature work cessation was due to arthritis inquired about work cessation at any time, past or present. Therefore, the arthritis-attributed work cessation prevalence we found may be inflated. The figures do, however, reflect the impact of arthritis on employment and could be conservative if subjects underestimate the influence of arthritis on their decisions to stop working.
In conclusion, our data suggest that work disability among persons with RA in the US is still a substantial problem. However, although there was no apparent reduction in work disability among subjects with early disease, our data in comparison with previous US studies also suggest there has been some improvement over the past 15–20 years in those with longer-standing disease. The differences between our findings and those of previous studies, however, could be based on sample or other methodologic differences.
Acknowledgments
Supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases, NIH, Bethesda, Maryland (grant P60-AR47785).
Footnotes
AUTHOR CONTRIBUTIONS Dr. Allaire had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study design. Allaire, Wolfe, LaValley.
Acquisition of data. Allaire, Wolfe.
Analysis and interpretation of data. Allaire, Wolfe, Niu, LaValley.
Manuscript preparation. Allaire, LaValley.
Statistical analysis. Allaire, Niu, LaValley.
REFERENCES
- 1.Verstappen SM, Bijlsma JW, Verkleij H, Buskens E, Blaauw AA, ter Borg EJ, et al. on behalf of the Utrecht Rheumatoid Arthritis Cohort Study Group Overview of work disability in rheumatoid arthritis patients as observed in cross-sectional and longitudinal surveys [review] Arthritis Rheum. 2004;51:488–97. doi: 10.1002/art.20419. [DOI] [PubMed] [Google Scholar]
- 2.Allaire SH. Update on work disability in rheumatic diseases. Curr Opin Rheumatol. 2001;13:93–8. doi: 10.1097/00002281-200103000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Cooper NJ. Economic burden of rheumatoid arthritis: a systematic review. Rheumatology (Oxford) 2000;39:28–33. doi: 10.1093/rheumatology/39.1.28. [DOI] [PubMed] [Google Scholar]
- 4.Yelin E, Henke C, Epstein W. The work dynamics of the person with rheumatoid arthritis. Arthritis Rheum. 1987;30:507–12. doi: 10.1002/art.1780300504. [DOI] [PubMed] [Google Scholar]
- 5.Callahan LF, Bloch DA, Pincus T. Identification of work disability in rheumatoid arthritis: physical, radiographic and laboratory variables do not add explanatory power to demographic and functional variables. J Clin Epidemiol. 1992;45:127–38. doi: 10.1016/0895-4356(92)90005-8. [DOI] [PubMed] [Google Scholar]
- 6.Wolfe F, Hawley DJ. The longterm outcomes of rheumatoid arthritis. Work disability: a prospective 18 year study of 823 patients. J Rheumatol. 1998;25:2108–17. [PubMed] [Google Scholar]
- 7.Reisine S, Fifield J, Walsh SJ, Feinn R. Factors associated with continued employment among patients with rheumatoid arthritis: a survival model. J Rheumatol. 2001;28:2400–8. [PubMed] [Google Scholar]
- 8.Wolfe F, Michaud K. Work disability in a national sample of RA patients [abstract] Arthritis Rheum. 2002;46(Suppl 9):S90–1. [Google Scholar]
- 9.Kremers HM, Nicola P, Crowson CS, O'Fallon WM, Gabriel SE. Therapeutic strategies over a 40-year period. J Rheumatol. 2004;31:2366–73. [PubMed] [Google Scholar]
- 10.Welsing PM, Fransen J, van Riel PL. Is the disease course of rheumatoid arthritis becoming milder? Time trends since 1985 in an inception cohort of early rheumatoid arthritis. Arthritis Rheum. 2005;52:2616–24. doi: 10.1002/art.21259. [DOI] [PubMed] [Google Scholar]
- 11.Kirschstein R. Disease-specific estimates of direct and indirect costs of illness and NIH support: fiscal year 2000 update. 2000 URL: http://ospp.od.nih.gov/ecostudies/COIreportweb.htm.
- 12.Lucas MR, Whitley DM, Kwoh CK, Dorman JS. Work instability in rheumatoid arthritis: an innovative approach [abstract] Am J Epidemiol. 1991;134:744. [Google Scholar]
- 13.Eberhardt K, Larsson BM, Nived K, Lindqvist E. Work disability in rheumatoid arthritis: development over 15 years and evaluation of predictive factors over time. J Rheumatol. 2007;34:481–7. [PubMed] [Google Scholar]
- 14.Fries JF, Spitz PW, Young DY. Dimensions of health outcomes: the Health Assessment Questionnaire, disability and pain scales. J Rheumatol. 1982;9:789–93. [PubMed] [Google Scholar]
- 15.Reisine S, Fifield J, Walsh S, Dauser D. Work disability among two cohorts of women with recent-onset rheumatoid arthritis: a survival analysis. Arthritis Rheum. 2007;57:372–80. doi: 10.1002/art.22620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.US Census Bureau . Unemployment rates, by race and Hispanic origin: 1980–1998. 119th ed Statistical Abstract of the US; Washington (DC): 1999. [Google Scholar]
- 17.Burton W, Morrison A, Maclean R, Ruderman E. Systematic review of studies of productivity loss due to rheumatoid arthritis. Occup Med (Lond) 2006;56:18–27. doi: 10.1093/occmed/kqi171. [DOI] [PubMed] [Google Scholar]
- 18.Kriegsman DM, Penninx BW, van Eijk JT, Boeke AJ, Deeg DJ. Self-reports and general practitioner information on the presence of chronic diseases in community dwelling elderly: a study on the accuracy of patients' self-reports and on determinants of inaccuracy. J Clin Epidemiol. 1996;49:1407–17. doi: 10.1016/s0895-4356(96)00274-0. [DOI] [PubMed] [Google Scholar]