

Abstract
Background:
Cystic renal neoplasms of the kidney can be benign or malignant. Multicystic nephroma (MCN) represents a rare benign cystic lesion of the kidney, which usually presents as a unilateral multicystic renal mass without solid elements. According to the World Health Organization (WHO) classification of the renal neoplasms, it is grouped along with mixed epithelial–stromal tumor of the kidney.
Materials and Methods:
We report a retrospective review of six cases of MCN of kidney. Patient demographics, imaging findings, operative details and final histology were recorded.
Results:
All patients had suspicious/malignant features on radiological examination, leading to a radical nephrectomy. However, microscopically these lesions were lined by cuboidal epithelium, and in a few places hobnail epithelium. No cells with clear cytoplasm, blastemal or immature elements were seen. In one case, foci of inflammatory cells and histiocytes were present.
Conclusions:
MCN is a benign cystic lesion and clinical presentations are nonspecific with symptoms such as abdominal pain, hematuria and urinary tract infection. These nonspecific clinical presentations and confusing radiological features create difficult preoperative differentiation from malignant cystic renal neoplasms.
Keywords: Cystic nephroma, imaging, multicystic renal mass
INTRODUCTION
Multicystic nephroma (MCN) is a rare, benign cystic neoplasm of the kidney. It was first described in 1892 as cystic adenoma of the kidney and over 200 cases have been reported in the literature so far.[1] Its etiology and histogenesis is debatable, and in the past they were considered to be developmental lesions with malignant potential. The name multicystic nephroma was first proposed in 1951 and later modified and further subdivided into cystic nephroma and cystic partially differentiated nephroma depending on the absence and presence of blastemal element, respectively.[2]
MCN is an uncommon, benign cystic lesion of the kidney with bimodal age distribution, occurring in both infants and adult population. Although it has been described in neonates, MCN is more commonly seen in the age group of 2–4 years (of which 73% are in males). Below 4 years of age, male to female ratio is 3:1 and boys are affected more than girls. In adults, it is seen in the 4th–6th decade with its male to female ratio being 1:8.[3–6] Adult-onset cystic nephroma is histogenetically and morphologically different from pediatric cystic nephroma.[7–9] According to the World Health Organization (WHO) classification of renal neoplasms, MCN is grouped with the mixed epithelial and stromal tumors (MEST).[10] The term renal epithelial and stromal tumor (REST) can be used to encompass both MCN and MEST.[11]
Surgical intervention is the effective method at present to exclude malignant cystic lesions of kidney. However, nephron-sparing surgery can be an option depending on the site and size of the lesion. We performed a retrospective review of six cases of MCN with regards to clinical, radiological and pathological features. This case series proves that despite recent advances in radiology and pathology, MCN still remains a surgically treated lesion with no definitive features that allow confident pre-operative diagnosis.
MATERIALS AND METHODS
Following a search of multidisciplinary records and our department's pathology results server between 2002 and 2009, all cases of adult MCN were identified. This revealed six cases of MCN, all of which were confirmed as MCN following histological examination. The patients' medical case notes were then accessed from the Medical Records department to enable clinical details to be collated. The radiology information server was then used to access the relevant imaging performed. The initial radiological reports were read, and in addition the images were retrospectively evaluated.
RESULTS
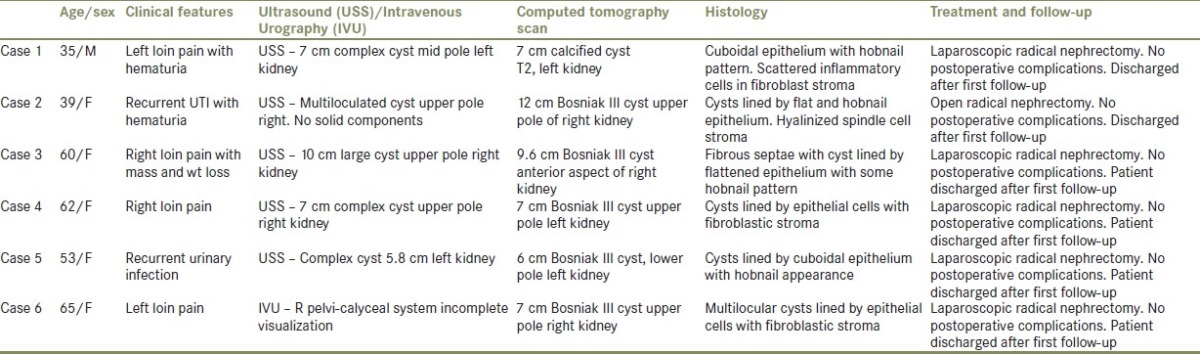
In all patients, a computed tomography (CT) scan suggested a Bosniak III type cyst. Five patients underwent a laparoscopic nephrectomy. Clinical, radiology, pathology and management details are presented in Table 1.
Table 1.
Patient characteristics, radiological and histological features of cases of cystic nephroma
DISCUSSION
MCN has at least 20–25 synonyms, which include multilocular cystic renal tumor, benign multilocular cystic nephroma, polycystic nephroblastoma, and so on.
The pathogenesis of MCN is controversial and its classification is confusing. There are numerous proposed theories indicating the etiology as a developmental defect.[12] It has also been postulated that it could be neoplastic in origin, probably arising from the ureteral bud.[12] Various pathological criteria have been proposed in the past to differentiate and classify this entity. First diagnostic criteria were formulated in 1951[2] and later modified in 1956[13] and include the following: (a) lesion must be multilocular, (b) the cyst for the most part lined by epithelium, (c) the cyst must not communicate with renal pelvis, (d) the residual renal tissue should be essentially normal, except for pressure atrophy, and finally (e) no fully developed nephrons. The terminology was modified in 1989, which emphasized neoplastic rather than developmental origin.[9] It was broadly segregated into MCN and cystic partially differentiated nephromablastoma.[9] In MCN, multiple cysts showed septa consisting of mature, well-differentiated tubules among the fibrous tissue. Lesions which were predominately cystic without nodular or solid components and containing blastemal elements were noted as cystic partially differentiated nephroma, especially those occurring in the age group less than 2 years. Further subclassification of cystic partially differentiated nephroma was attempted to predict the aggressiveness of this entity based on the content of septal stromal elements, and presence of more than 50% of mature septal element was classified as grade I and less than 50% as grade II.[9]
Patients usually present with nonspecific symptoms. Abdominal pain, hematuria, and urinary tract infection are common in adults. Hematuria can be seen in all age groups and is thought to be due to extension of tumor into the renal pelvis.[14,15] Loin pain was the commonest presentation in this study and only two patients presented with hematuria. Presentation can sometimes be with severe colicky abdominal pain due to spontaneous rupture of the cyst,[16] which can lead to a clinical diagnosis of urinary stone disease. In the present series, case no. 6 had a similar presentation and an intravenous urogram was nondiagnostic. It usually affects single kidney, although rarely bilateral MCN has been reported.[3,6,17] Lower pole of kidney is the most favored site and the upper pole is the least favored; however, it can arise from any portion of the renal parenchyma. Interestingly, in the present series, upper pole was the most common site of presentation.
Distinct radiographic features have been described [Table 2], but are not universally present in all cases. Ultrasound is often the first investigation used in evaluating abdominal masses, confirmed by CT scan. The sonographic findings depend on the amount of stromal tissue and size of locules. Cysts usually show up as hypoechoic lesions delineated by hyperechoic septae [Figure 1], and this feature can be suggestive of MCN but not diagnostic. The mass is often easily demonstrable at ultrasound, with an average diameter of approximately 10 cm.[18] Our six cases had a mean maximum diameter of 8.9 cm. If the cysts are small, the mass may demonstrate internal scattered echoes but without distinct loculations.[3] Calcification has been described as a rare feature of MCN,[6] and curvilinear calcifications may be seen on ultrasound within the septa. None of our patients displayed calcification within the MCN on any imaging modality. If present, as in one of our cases, urinary obstruction may be well demonstrated with ultrasound. Both needle-guided aspiration and color Doppler ultrasound have been proposed to help differentiate between benign and malignant multilocular cystic lesions.[19]
Table 2.
Radiological and pathological features of multicystic nephroma
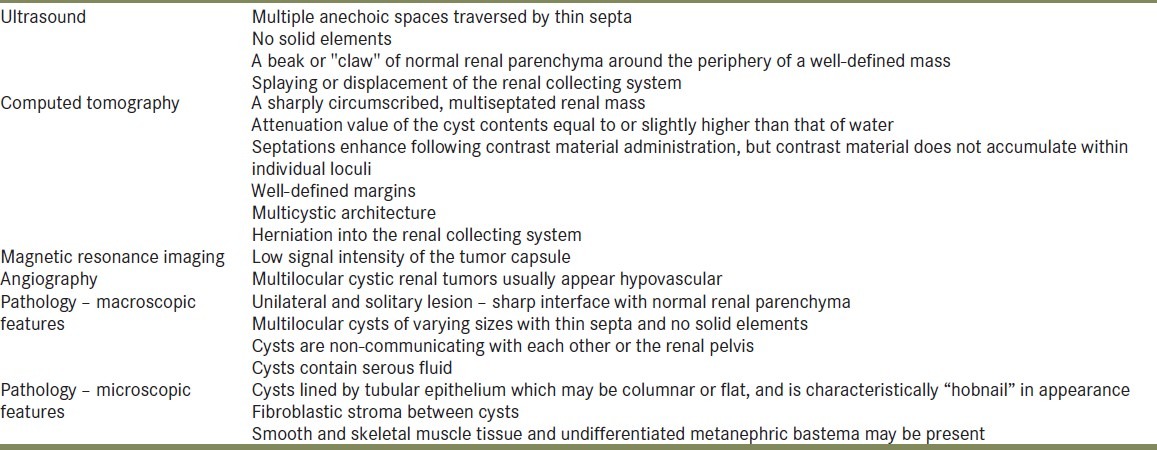
Figure 1.
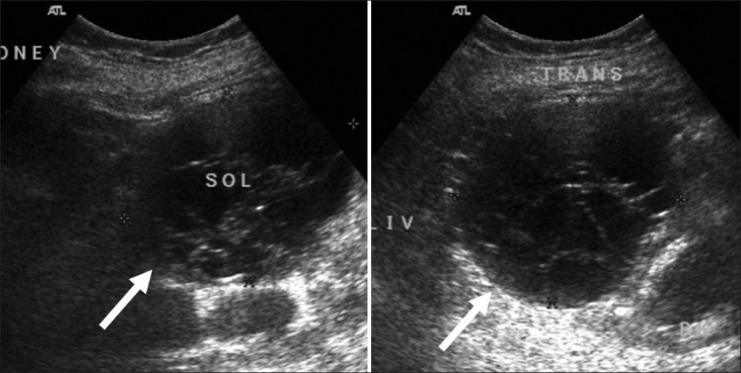
Ultrasound of the right kidney. Longitudinal (left) and transverse (right) images show a well-defined multiseptated cystic lesion (arrows) at the lower pole
CT image features suggestive of MCN are multicystic architecture [Figure 2] with well-defined margins, enhancing septae and herniation into renal pelvis. This herniation often causes hematuria. However, it is interesting to note that the two cases in this series presenting with hematuria did not show any herniation in CT imaging. Calcification is rarely seen; occasionally, however, ossification can occur within septa or within the renal capsule. Central or small peripheral curvilinear calcifications can occasionally be seen at the edge of the herniated pelvic portion.[20] In addition, dense calcium rings in multiple cysts have been reported.[4] If present, calcification may lead to confusion with malignancy as case no. 1 in the present series was reported as a T2 lesion on CT.
Figure 2.
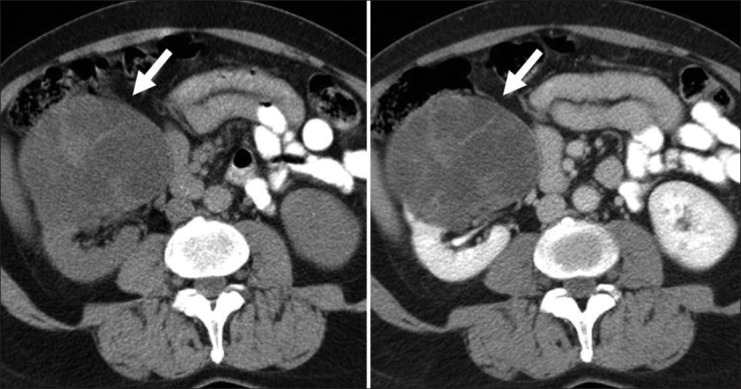
Unenhanced (left) and portal venous phase (right) CT shows an extensive multicystic mass (arrows) bulging the renal capsule at multiple sites
Magnetic resonance imaging (MRI) is rarely indicated, but imaging features include usually hypointense signal on T1-weighted sequences (although this may vary) and hyperintense signal on T2-weighted sequences.[21] Septa are usually hypointense on all sequences due to fibrous content.[22]
Angiography appearances of MCN may appear as avascular or hypervascular. However, this is nonspecific and nondiagnostic, as MCN may be avascular, hypo- or hypervascular.[23]
The pathological features of the multilocular cystic renal neoplasms including cystic nephroma and cystic hamartoma, which show cystic growth pattern, are very difficult to separate radiographically.[24] Fine needle aspiration cytology (FNAC) has been attempted in order to establish a preoperative diagnosis. Papanicolaou staining of the cyst fluid showed markedly atypical cells forming papillary clusters. However, though not very conclusive, low cellularity, absence of necrosis, and paucity of single cells should be viewed with suspicion of MCN.[25] All six cases in this study had lesions lined by cuboidal epithelium [Figure 3], and in a few places hobnail epithelium [Figure 4] was seen. The stroma was composed of varying amounts of hyalinized spindle cells, fibroblasts, and smaller renal tubules lined by single layer of cuboidal epithelium. No cells with clear cytoplasm, blastemal or immature elements were seen. However, foci of inflammatory cells and histiocytes were noted in one case. On immunohistochemistry, all six cases had an ovarian-like stroma in between the cysts, positive for both estrogen receptor (ER) and progesterone receptor (PR). No serological markers or immunohistochemistry features are conclusive in differentiating between MCN, cystic partially differentiated nephroma and cystic renal cell carcinoma.[5] Stromal positivity for ER or PR was seen in all of our cases, indicating that such positivity should support a diagnosis of MCN. Frozen section could be an option in deciding between radical and nephron-sparing nephrectomy, but partially cystic renal cell carcinoma may be potentially missed on frozen section. None of the cases in the present series was deemed suitable for partial nephrectomy because of the size and position of the lesion.
Figure 3.

Cut section of multilocular cystic nephroma
Figure 4.
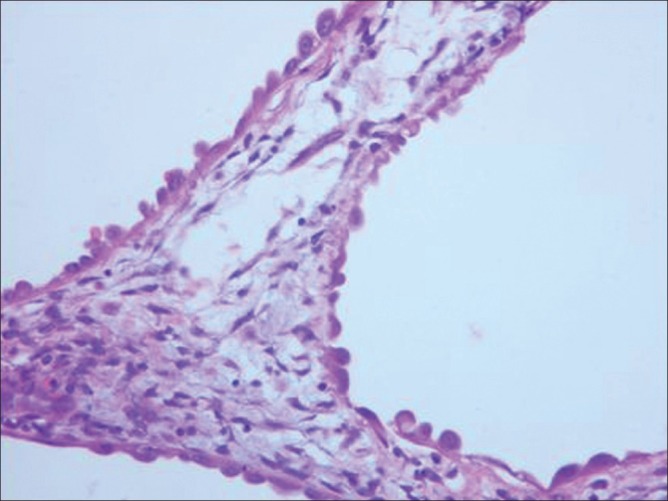
Microscopy showing hobnail appearance of cyst lining ×40
It is widely believed that it is impossible to clinically or radiologically distinguish between the benign entity of MCN and renal cell carcinoma. Our six cases further support this. Following CT and/or ultrasound assessment and then discussion at the local multidisciplinary meeting, all of our cases were treated as Bosniak type III lesions and surgery was therefore advised [Table 1]. Even in retrospect, none of the imaging features would have allowed one to be completely certain of a benign diagnosis. All our cases showed multiloculated cystic lesions with locules of varying sizes, and none of the lesions displayed communication between the cysts or communication between the cysts and the renal pelvis. Some of the lesions contained thin septa and some of the lesions contained both thick and thin septa, displaying measurable enhancement on CT. However, none of the lesions contained solid elements on either imaging or on histological analysis.
Although the MCN is not a pre-malignant condition, there are case reports of co-existing foci of renal cell carcinoma in the lining of the cyst wall. MCN is considered to be of benign nature in adults; tumor recurrences have been observed and whether these recurrences are related to the missed foci of malignant area or sarcomatous degeneration is not clear.[19] These recurrences are more often seen after partial nephrectomy. So far, only four cases of local recurrences have been reported, all following partial nephrectomy.[26] However, in a series of 24 patients who underwent partial nephrectomy for MCN, no recurrences were found after a mean follow-up of 39 months.[6] More recently, a case of percutaneous treatment has been described in treating MCN. Percutaneous endoscopic resection of a portion of the cyst protruding into the renal parenchyma was performed, and follow-up CT 4 weeks later revealed complete resolution.[27] However, 3 years later, the authors reported failure with percutaneous approach.[28]
CONCLUSION
Multilocular cystic nephroma is an uncommon cystic lesion of the kidney and should be considered in the differential diagnosis of malignant cystic renal tumors in both children and adults. Whilst it is important to consider the diagnosis of MCN for any multicystic mass, as our series of six cases has shown, a definitive diagnosis can only be made following surgical treatment with total or partial nephrectomy depending on the size and location of the lesion in the kidney.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Edmunds W. Cystic adenoma of the kidney. Trans Pathol Soc Lond. 1892;43:89–90. [Google Scholar]
- 2.Powell T, shackman R, Johnson HD. Multilocular cysts of kidney. Br J Urol. 1951;23:142–52. doi: 10.1111/j.1464-410x.1951.tb02576.x. [DOI] [PubMed] [Google Scholar]
- 3.Madewell JE, Goldman SM, Davis CJ, Jr, Hartman DS, Feigin DS, Lichtenstein JE. Multilocular cystic nephroma: A radiographic-pathologic correlation of 58 patients. Radiology. 1983;146:309–21. doi: 10.1148/radiology.146.2.6294736. [DOI] [PubMed] [Google Scholar]
- 4.Banner MP, Pollack HM, Chatten J, Witzleben C. Multilocular renal cysts: Radiologic-pathologic correlation. AJR Am J Roentgenol. 1981;136:239–47. doi: 10.2214/ajr.136.2.239. [DOI] [PubMed] [Google Scholar]
- 5.Mukhopadhyay S, Valente AL, de la Roza G. Cystic Nephroma: A histologic and immunohistochemical study of 10 cases. Arch Path Lab Med. 2004;128:1404–11. doi: 10.5858/2004-128-1404-CNAHAI. [DOI] [PubMed] [Google Scholar]
- 6.Castillo OA, Boyle ET, Jr, Kramer SA. Multilocular cysts of kidney. A study of 29 patients and review of literature. Urology. 1991;37:156–62. doi: 10.1016/0090-4295(91)80214-r. [DOI] [PubMed] [Google Scholar]
- 7.Eble JN, Bonsib SM. Extensively cystic renal neoplasms: Cystic nephroma, cystic partially differentiated nephroblastoma, multilocular cystic renal cell carcinoma, and cystic hamartoma of renal pelvis. Semin Diagn Pathol. 1998;15:2–20. [PubMed] [Google Scholar]
- 8.Bisceglia M, Galliani CA, Senger C, Stallone C, Sessa A. Renal cystic diseases: A review. Adv Anat Pathol. 2006;13:26–56. doi: 10.1097/01.pap.0000201831.77472.d3. [DOI] [PubMed] [Google Scholar]
- 9.Joshi VV, Beckwith JB. Multilocular cyst of the kidney (cystic nephroma) and cystic, partially differentiated nephroblastoma. Terminology and criteria for diagnosis. Cancer. 1989;64:466–79. doi: 10.1002/1097-0142(19890715)64:2<466::aid-cncr2820640221>3.0.co;2-v. [DOI] [PubMed] [Google Scholar]
- 10.Bonsib SM. Cystic nephroma. Mixed epithelial and stromal tumor. In: Eble JN, Sauter G, Epstein JI, Sesterhenn IA, editors. World Health Organization classification of tumours. Pathology and genetics of tumors of the urinary system and male genital organs. Lyon: IARC Press; 2004. p. 76. [Google Scholar]
- 11.Turbiner J, Amin MB, Humphrey PA, Srigley JR, De Leval L, Radhakrishnan A, et al. Cystic nephroma and mixed epithelial and stromal tumor of kidney: A detailed clinicopathologic analysis of 34 cases and proposal for renal epithelial and stromal tumor (REST) as a unifying term. Am J Surg Pathol. 2007;31:489–500. doi: 10.1097/PAS.0b013e31802bdd56. [DOI] [PubMed] [Google Scholar]
- 12.Sacher P, Willi UV, Niggli F, Stalmach T. Cystic Nephroma: A rare benign renal tumour. Paediatric Surg Int. 1998;13:197–9. doi: 10.1007/s003830050290. [DOI] [PubMed] [Google Scholar]
- 13.Boggs LK, Kimmelsteil P. Benign multilocular cystic nephroma: Report of two cases of multilocular cyst of kidney. J Urol. 1956;76:530–41. doi: 10.1016/S0022-5347(17)66732-6. [DOI] [PubMed] [Google Scholar]
- 14.Bouhafs A, Cherradi N, Lamaalmi N, Beklachem R, Barahioui M. An unusual case of multicystic Nephroma with prominent renal pelvis involvement. Int J Urol. 2006;13:436–8. doi: 10.1111/j.1442-2042.2006.01330.x. [DOI] [PubMed] [Google Scholar]
- 15.Kural AR, obek K, Ozbay G, Onder AU. Multilocular cystic Nephroma: An unusual presentation. Urology. 1998;52:897–9. doi: 10.1016/s0090-4295(98)00386-0. [DOI] [PubMed] [Google Scholar]
- 16.Fujimoto K, Samma S, Yamaguchi A, Hirayama A, Kikkawa A. Spontaneously ruptured multilocular cystic nephro ma. Int J Urol. 2002;93:183–6. doi: 10.1046/j.1442-2042.2002.00441.x. [DOI] [PubMed] [Google Scholar]
- 17.Cheng EY, Cohn RA, Palmer LS, Fernbach S, Firlit CF. A rare case of bilateral multilocular renal cysts. J Urol. 1997;157:1861–2. [PubMed] [Google Scholar]
- 18.Hattery RP. Benign neoplasms of the renal parenchyma. In: Pollack HM, McClennan BL, editors. Clinical Urography. 2nd ed. Philadelphia, USA: W.B.Saunders Company; 2000. pp. 1429–34. [Google Scholar]
- 19.Hirai T, Ohishi H, Yamada R, Imai Y, Hirohashi S, Hirohashi R, et al. Usefulness of colour Doppler flow imaging in differential diagnosis of multilocular cystic lesions of the kidney. J Ultrasound Med. 1995;14:771–6. doi: 10.7863/jum.1995.14.10.771. [DOI] [PubMed] [Google Scholar]
- 20.Brown RC, Cornell SH, Culp DA. Multilocular renal cyst with diffuse calcification simulating renal cell carcinoma. Radiology. 1970;95:411–2. doi: 10.1148/95.2.411. [DOI] [PubMed] [Google Scholar]
- 21.Kim SH, Choi BI, Han MC, Kim CW, Kim YI. Multilocular cystic nephroma: MR findings. AJR Am J Roentgenol. 1989;153:1317. doi: 10.2214/ajr.153.6.1317-a. [DOI] [PubMed] [Google Scholar]
- 22.Silver IM, Boag AH, Soboleski DA. Best cases from the AFIP: Multilocular cystic renal tumor: Cystic nephroma. Radiographics. 2008;28:1221–5. doi: 10.1148/rg.284075184. [DOI] [PubMed] [Google Scholar]
- 23.Hsiao HL, Wu WJ, Chang MY, Ke HL, Huang CH. Unusual case of multilocular cystic nephroma treated with nephron sparing technique: A case report. Kaohsiung J Med Sci. 2006;22:515–8. doi: 10.1016/S1607-551X(09)70346-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hora M, Hes O, Michal M, Boudová L, Chudácek Z, Kreuzberg B, et al. Extensively cystic Renal Neoplasms in Adults (Bosniak II or III) – possible “Common” Histological Diagnosis: Multilocular cystic renal carcinoma, Cystic Nephroma, and Mixed epithelial and stromal tumour of the kidney. Int J Urol Nephrol. 2005;37:743–50. doi: 10.1007/s11255-005-1201-5. [DOI] [PubMed] [Google Scholar]
- 25.Clark SP, Kung IT, Tang SK. Fine Needle Aspiration of Cystic Nephroma (Multilocular cyst of kidney) Diagn Cytopathol. 1992;8:349–51. doi: 10.1002/dc.2840080408. [DOI] [PubMed] [Google Scholar]
- 26.Bastian PJ, Kulhmann R, Vogel J, Bastian HP. Local recurrence of a unilateral cystic nephroma. Int J Urol. 2004;11:329–31. doi: 10.1111/j.1442-2042.2004.00787.x. [DOI] [PubMed] [Google Scholar]
- 27.Dash A, Wolf JS. Percutaneous treatment of renal cystic nephroma. J Endourol. 2005;19:724–5. doi: 10.1089/end.2005.19.724. [DOI] [PubMed] [Google Scholar]
- 28.Wolf JS, Jr, Dash A. Failure of percutaneous endoscopic resection of a renal cystic nephroma on longer-term follow-up. J Endourol. 2008;22:1505–7. doi: 10.1089/end.2007.0441. [DOI] [PubMed] [Google Scholar]