

Abstract
T-lymphocytic infiltration near the tumor site is an expected immune response in bladder cancers. However, reports of patients with bladder cancer exhibiting small lymphocytic infiltration of the bladder tissue are very rare in the literature. Here, the patient was presented to our group with hematuria, but subsequently diagnosed as exhibiting invasive bladder cancer and chronic lymphocytic leukemia with suspicious lymphocytic infiltration in a transurethral resection specimen. This case emphasizes the importance of lymphocytic infiltration's nature near urothelial carcinoma.
Keywords: Bladder cancer, coincidence, infiltration, leukemia
INTRODUCTION
Patients with chronic lymphocytic leukemia (CLL) have an increased risk of developing a second type of cancer. However, coincidence of CLL and bladder cancer is very rare.[1] Only three cases with CLL and bladder cancer were reported in the literature.[2,3] Healthy bladder does not contain lymphoid tissue; however, T lymphocyte and monocyte infiltrations have been monitored in bladder cancers and these cells are called as tumor infiltrating lymphocytes (TILs). It is important to distinguish these lymphocytes from other pathologies. We report on a case that did not have any risks or properties of a lymphoproliferative disorder preoperatively, and was diagnosed as CLL with the suspicion in transurethral specimen of bladder cancer.
CASE REPORT
A 62 year-old man was referred to our urology unit with a history of painless intermittent hematuria for 3 months. His occupation was long-distance driver; he had no chronic illness and a history of smoking for 45 years. In his physical examination, there were no significant findings such as hepatosplenomegaly, lymphadenopathy, fever or weight loss. Leukocytosis (15700 103/ ul) was determined in the blood cell count and thought to be related to the pyuria in the urinalysis. The left kidney was found at grade three hydronephrosis and a heterogeneous hypoechoic solid mass with irregular borders on the left side of the bladder wall were reported in the abdominal ultrasonography. All papillary masses in the left side of the bladder wall and in the prostatic urethra were resected transurethrally. The transurethral resection specimen was fixed in 10% buffered formaldehyde and routine hematoxylin and eosin preparation was performed for histological examination. Immunohistochemistry was performed on the formalin–fixed, paraffin-embedded tissue sections. Light microscopic examination revealed high grade urothelial carcinoma extending into the muscularis propria. The urothelium of the surrounding bladder mucosa showed carcinoma in situ. Diffuse small lymphocytic infiltration was found along the periphery of the tumor. Immunohistochemical studies revealed that the lymphocytes present in the region were positive for CD20, CD5 and CD43 and transitional cell carcinoma (TCC) [Figures 1 and 2]. After the pathological report the patient was investigated for hematological malignancies. Computer tomography scan of the abdomen, pelvic and chest regions demonstrated asymmetric wall thickening in the left side of the bladder and multiple lymphadenopathies in the pelvis and upper abdomen [Figure 3]. A peripheral blood smear and flow cytometry were performed and resulted in a diagnosis of CLL. The patient's final diagnosis was a coincidence of invasive bladder cancer and CLL. The patient received chemoradiotherapy for bladder cancer. CLL was followed conservatively. The patient died six months after diagnosis as a result of heart attack.
Figure 1.
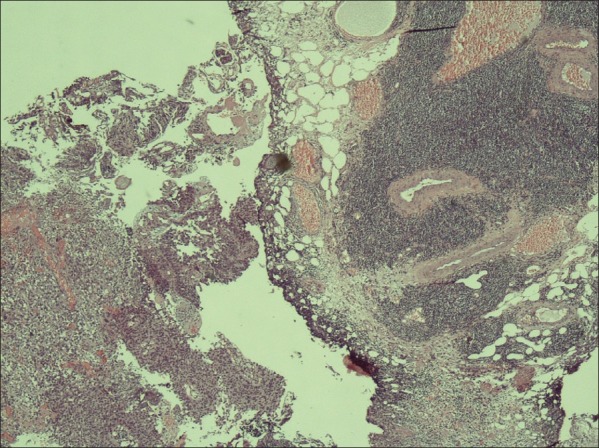
Transitional cell carcinoma with small lymphocytic infiltration (H and E, ×100)
Figure 2.
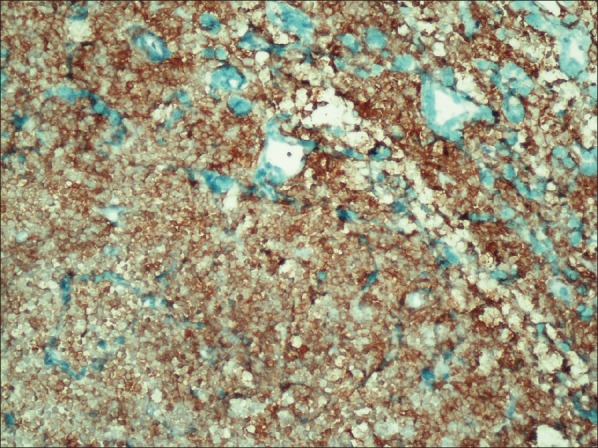
Small lymphoid cells were positive for CD20 (×200)
Figure 3.

Computer tomography scan of the abdomen showing lymphadenopathies in abdomen of the patient
DISCUSSION
Bladder cancer and lymphoproliferative disorders may occur in a patient at the same time due to common etiologic factors such as benzene or dyes;[4] due to the therapies for lymphoproliferative malignancies[5] and bladder cancers.[6] Furthermore, though rare, lymphoproliferative disorders can infiltrate to the urinary bladder. This is not a common occurrence because the healthy bladder does not contain lymphoid tissue.[7] However, T lymphocyte and monocyte infiltrations have been observed in bladder cancers. Activated T cells, natural killer cells and non-T and non-B lymphocytes, collectively called tumor infiltrating lymphocytes (TILs), have cytotoxic activity and migrate to the site of the bladder tumor in order to inhibit the malignant cells.[8] TCC with higher number of TILs is reported to have a favorable prognosis,[9] with fewer occurrences of recurrence[10] and metastates.[11] But this anti-tumor response of the host immune system cannot manage the bladder tumor because mutations within tumor cells prevent tumor eradication by TILs over a prolonged period of time.[8]
The risk of coincident malignancies in patients with CLL, which results from uncontrolled B lymphocytes in the hematopoietic organs, is higher because of the immune dysregulation[12] and treatment with alkylating agents.[13] Breast, skin, brain and prostate cancers have been reported as common coincident tumors of CLL,[14] while in rare cases CLL may infiltrate other solid organs, such as skin, lung, heart and prostate.[15] Urinary bladder involvement in CLL is also a very rare situation.[16] Although the relation between these two tumors is unclear, one possible theory involves glutathione S-transferase M1 (GSTM1) which is important in the metabolism of environmental carcinogens, reactive oxygen species, and chemotherapeutic agents. The cigarette smoke carcinogens inactivate this GSTM1 genotype and these smokers behave as GSTM1 null genotype. Increased bladder cancer risk has been shown with GSTM1 null status and in all the cigarette smokers, even if they were positive for GSTM1, as an effect of tobacco exposure.[17] Also GSTM1 null status and GSTM1 genotype inactivated by chemical agents was higher in patients with CLL.[18]
Although the patients with CLL may present with lymphoproliferative diseases and immunosupression symptoms, pathological findings during the physical examination did not indicate CLL in our case. He had a history of smoking, but not of exposure to chemical agents or medical therapies for other malignancies. The pathological examination of the specimen derived by transurethral resection from bladder carcinoma was identified as invasive urothelial carcinoma with lymphocytic infiltrations. These diffuse small lymphocyte infiltrates were expected to be TILs but were determined by immunohisochemistry to be CD20 positive. Further tests indicated that this patient had both invasive bladder cancer and CLL. As a result, this case indicated to us the importance of the nature of lymphocytic infiltration in bladder carcinoma.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Martín Hernández M, Alonso y Gregorio S, Cansino Alcaide R, Pérez-Utrilla M, Aguilera Bazán A, Regojo Zapata R, et al. Leukemic infiltration of the urinary bladder. A new case and literature review. Actas Urol Esp. 2008;32:563–6. doi: 10.1016/s0210-4806(08)73885-3. [DOI] [PubMed] [Google Scholar]
- 2.Lishner M, Prokocimer M, Ron E, Shaklai M. Primary malignant neoplasms associated with chronic lymphocytic leukaemia. Postgrad Med J. 1987;63:253–6. doi: 10.1136/pgmj.63.738.253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Takács I, Berkessy S, Hártó G. Primary malignant neoplasms associated with chronic lymphocytic leukemia. Postgrad Med J. 1992;68:595–6. doi: 10.1136/pgmj.68.801.595-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kelsh MA, Alexander DD, Kalmes RM, Buffler PA. Personal use of hair dyes and risk of bladder cancer: A metaanalysis of epidemiologic data. Cancer Causes Control. 2008;19:549–58. doi: 10.1007/s10552-008-9123-z. [DOI] [PubMed] [Google Scholar]
- 5.Pathak AB, Advani SH, Gopal R, Nadkarni KS, Saikia TK. Urinary bladder cancer following cyclophosphamide therapy for Hodgkin's disease. Leuk Lymphoma. 1992;8:503–4. doi: 10.3109/10428199209051035. [DOI] [PubMed] [Google Scholar]
- 6.Easton DJ, Poon MA. Acute nonlymphocytic leukemia following bladder instillations with thiotepa. Can Med Assoc J. 1983;129:578–9. [PMC free article] [PubMed] [Google Scholar]
- 7.Bhansali SK, Cameron KM. Primary Malignant Lymphoma of the Bladder. Br J Urol. 1960;32:440. [Google Scholar]
- 8.Liakou CI, Narayanan S, Ng Tang D, Logothetis CJ, Sharma P. Focus on TILs: Prognostic significance of tumor infiltrating lymphocytes in human bladder cancer. Cancer Immun. 2007;7:10. [PMC free article] [PubMed] [Google Scholar]
- 9.Mostofi FK, Sesterhenn I. Plenary lecture: Lymphocytic infiltration in relationship to urological tumors. Natl Cancer Inst Monogr. 1978;49:133–41. [PubMed] [Google Scholar]
- 10.Lipponen PK, Eskelinen MJ, Jauhiainen K, Harju E, Terho R. Tumour infiltrating lymphocytes as an independent prognostic fac-tor in transitional cell bladder cancer. Eur J Cancer. 1993;29:69–75. doi: 10.1016/0959-8049(93)90579-5. [DOI] [PubMed] [Google Scholar]
- 11.Tsujihashi H, Matsuda H, Uejima S, Akiyama T, Kurita T. Immuno-competence of tissue infiltrating lymphocytes in bladder tumors. J Urol. 1988;140:890–4. doi: 10.1016/s0022-5347(17)41851-9. [DOI] [PubMed] [Google Scholar]
- 12.Ramadan KM, Kyle A, McManus D, O'Rourke D, Cuthbert RJ. Urinary bladder infiltration with chronic B-lymphocytic leukemia: Two cases with unusual presentation. Leuk Lymphoma. 2006;47:1184–7. doi: 10.1080/10428190500465341. [DOI] [PubMed] [Google Scholar]
- 13.Krause JR, Ayuyang HQ, Ellis LD. Secondary non-hematopoietic cancers arising following treatment of hematopoietic disorders. Cancer. 1985;55:512–5. doi: 10.1002/1097-0142(19850201)55:3<512::aid-cncr2820550307>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 14.Takács I, Berkessy S, Hártó G. Primary malignant neoplasms associated with chronic lymphocytic leukemia. Postgrad Med J. 1992;68:595–6. doi: 10.1136/pgmj.68.801.595-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hales DS, Cassidy M, Scott R, Lewi HJ. Immunocytoma of prostate. Urology. 1983;22:438–9. doi: 10.1016/0090-4295(83)90434-x. [DOI] [PubMed] [Google Scholar]
- 16.Carver JD, Calverley D, Shen P. Chronic lymphocytic leukemia/small lymphocytic lymphoma presenting in urinary bladder without peripheral blood lymphocytosis: Case report and literature review. Leuk Lymphoma. 2006;47:1163–5. doi: 10.1080/10428190500465283. [DOI] [PubMed] [Google Scholar]
- 17.Engel LS, Taioli E, Pfeiffer R, Garcia-Closas M, Marcus PM, Lan Q, et al. Pooled analysis and meta-analysis of glutathione S-transferase M1 and bladder cancer: A huge review. Am J Epidemiol. 2002;156:95–109. doi: 10.1093/aje/kwf018. [DOI] [PubMed] [Google Scholar]
- 18.Yuille M, Condie A, Hudson C. Relationship between glutathione S-transferase M1, T1 and P1 polymorphisms and chronic lymphocytic leukemia. Blood. 2002;99:4216–8. doi: 10.1182/blood.v99.11.4216. [DOI] [PubMed] [Google Scholar]