

Abstract
Spindle cell lipoma is a relatively uncommon benign adipocytic tumor that usually presents in subcutaneous fat of adult men. These are a rare form of lipoma, accounting for 1.5% of all lipomatous tumors, with a low rate of local recurrence and no risk of malignant behavior/dedifferentiation. Although few studies addressing the histological findings of spindle cell lipoma have been described, only a few descriptions of fine needle aspiration cytology (FNAC) findings have been documented in literature. We present a case of a 55-year-old male with a nodular swelling over left cheek (in the parotid region), which due to its location as well as prominent myxoid background prompted us to include the lipomatous salivary gland lesions in differential diagnosis. Our objective is to document and delineate the characteristic cytological features of spindle cell lipoma, which may permit a confident diagnosis on FNAC smears.
Keywords: Cytology, lipomatous pleomorphic adenoma, spindle cell lipoma
Introduction
Spindle cell lipoma is a slow growing, solitary tumor frequently located in upper back and neck that clinically resembles a usual lipoma. Although few studies addressing the histological findings of spindle cell lipoma have been described, only a few descriptions of fine needle aspiration cytology (FNAC) findings have been documented in literature.[1–4] Needle aspirates from spindle cell lipoma show some cytological features common to other fatty/spindle cell or myxoid lesions, benign as well as malignant. We present a case of a 55-year-old male with a nodular swelling over left cheek, which due to its location (in the parotid region) as well as prominent myxoid background prompted us to include the lipomatous salivary lesions in differential diagnosis. Our objective is to document and delineate the characteristic cytological features of spindle cell lipoma, which may permit a confident diagnosis on FNAC smears.
Case Report
A 55-year-old male presented to the surgical outpatient department with the chief complaint of a slow growing left-sided cheek swelling (in the parotid region) noticed a month ago. On examination, a 3 × 3 cm globular swelling, which was firm, mobile, non-tender, was seen located near the angle of mandible. Patient was referred for an FNA procedure. FNA procedure was performed using a 22-gauge needle attached to a 10-mL syringe that yielded a mucoid aspirate. Both air-dried and 95% alcohol-fixed smears were prepared and stained with Wright's Giemsa and Papanicolaou stain, respectively. Aspirate smears were cellular, showing many spindle-shaped cells in loose cohesive clusters admixed with mature adipocytes with abundant myxoid material in the background. Many clusters show traversing capillaries, scattered mast cells with very occasional epithelial cell cluster [Figure 1]. This occasional epithelial cell cluster could be from adnexal structure/sweat gland from overlying skin; even on complete processing of histopathological specimen, it was not represented in the excision biopsy sample. Due to the site of lesion, abundant myxoid material and adipocytic component, a possibility of lipomatous variant of pleomorphic adenoma/chondroid syringoma and spindle cell lipoma was suggested. Excision biopsy was performed. Peroperatively, an encapsulated lipomatous lesion was seen without any attachment to the parotid. Cut surface was yellowish, gelatinous, and vaguely lobulated. Microscopically, an encapsulated lesion comprising of mature adipose tissue intermingled with benign appearing spindle cells in a myxoid background with ropy collagen fibers and occasional scattered mast cell was noted [Figure 2]. However, no epithelial/myoepithelial component was seen, thus ruling out lipomatous salivary gland lesions. No areas of cellular pleomorphism/floret-like giant cells/lipoblasts/intricately traversing chicken wire capillaries were seen, thus excluding pleomorphic lipoma, liposarcoma, and myxoid liposarcoma.
Figure 1.
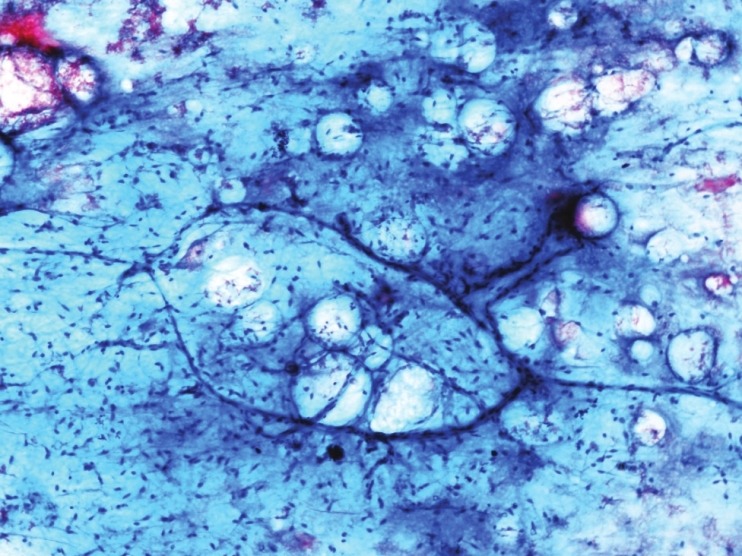
Aspirate smear showing mature adipocytes admixed with benign appearing spindle cells and few traversing capillaries (Pap, ×100)
Figure 2.
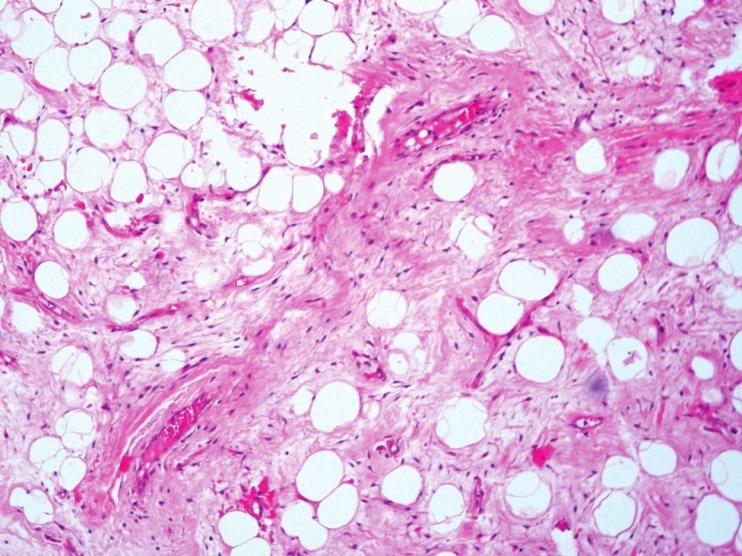
Tissue section revealing intermingled adipocytic and spindle cell component with ropy/wiry collagen fibers (H and E, ×100)
Finally, a diagnosis of spindle cell lipoma was rendered which was confirmed on immunohistochemistry in which spindle cells were diffusely and intensely positive for CD34.
Discussion
Spindle cell lipoma was first reported as a distinct entity in 1975 by Enzinger and Harvey.[5] These are a rare form of lipoma, accounting for 1.5% of all lipomatous tumors, with a low rate of local recurrence and no risk of malignant behavior/dedifferentiation.[6] Cytogenetic analysis reveal characteristic karyotypic aberrations notably loss of material from long arms of chromosomes 13 and 16. Domanski et al.,[1] in the first ever series on FNA of spindle cell lipoma summarized the cytological features as a mixture of mature adipocytes, uniform spindle cells, and collagen fibers in varying proportions. The spindle cells have pale, poorly defined cytoplasm with fusiform/ovoid basophilic nuclei showing mild anisokaryosis and inconspicuous nucleoli. Mast cells were noted in 50% of the cases and corresponded strongly with myxoid changes observed in the aspirate smears. In a couple of cases, small/middle-sized capillaries were observed.[1]
Differential diagnosis in FNA of spindle cell lipoma with a predominance of spindle cells includes neurilemmoma (distinct palisaded buckled nuclei with fibrillar matrix and no collagen/adipocytes), nodular fasciitis (plump myofibroblasts with active looking prominent nuclei), and fibromatosis (loose clusters of bland appearing spindled myofibroblasts without atypia). Spindle cell lipoma with a prominent myxoid component should evoke the differential of myxoma (viscous aspirate with scant bland spindle/stellate-shaped cells), myxoid neurofibroma (clusters of cells with wavy bent nuclei and fibrillar matrix), and myxoid liposarcoma (intricately admixed prominent plexiform chicken wire capillary network). Extensive adipocytic component along with clinical suspicion should prompt the cytopathologist to rule out liposarcoma by meticulous search for lipoblasts.
In the index case, due to the location of the lesion in the parotid region, a possibility of lipomatous salivary gland lesions in particular lipomatous variant of pleomorphic adenoma was considered. Lipomatous pleomorphic adenoma coined by Seifert et al,[7] in 1999, who defined the tumor as otherwise typical pleomorphic adenoma with abundant adipose component of >90% tumor area. Also known as pleomorphic adenoma with extensive lipometaplasia;[8] histogenesis is not clear and possible mechanisms include metaplastic transformation of myoepithelial cells to adipocytes or entrapment of adipose tissue. Other lipomatous salivary gland lesions include sialolipoma, oncocytic lipoadenoma, and lipomatosis.[8]
The present case highlights the fact that though the diagnosis of spindle cell lipoma with classic cytomorphological features is straightforward, but at times due to the site of the lesion in the parotid region and one/more predominant component, it can be a diagnostic challenge on cytology.
To conclude, in case of a swelling in parotid location yielding similar picture on FNA, a possibility of lipomatous salivary gland lesions needs to be excluded before rendering the diagnosis of spindle cell lipoma.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Domanski HA, Carlén B, Jonsson K, Mertens F, Akerman M. Distinct cytologic features of spindle cell lipoma. A cytologic-histologic study with clinical, radiologic, electron microscopic, and cytogenetic correlations. Cancer. 2001;93:381–9. doi: 10.1002/cncr.10142. [DOI] [PubMed] [Google Scholar]
- 2.Lew WY. Spindle cell lipoma of the breast: A case report and literature review. Diagn Cytopathol. 1993;9:434–7. doi: 10.1002/dc.2840090412. [DOI] [PubMed] [Google Scholar]
- 3.Guo Z, Voytovich M, Kurtycz DF, Hoerl HD. Fine-needle aspiration diagnosis of spindle-cell lipoma: A case report and review of the literature. Diagn Cytopathol. 2000;23:362–5. doi: 10.1002/1097-0339(200011)23:5<362::aid-dc17>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- 4.Agoff SN, Folpe AL, Grieco VS, Garcia RL. Spindle cell lipoma of the oral cavity. Report of a rare intramuscular case with fine needle aspiration findings. Acta Cytol. 2001;45:93–8. doi: 10.1159/000327195. [DOI] [PubMed] [Google Scholar]
- 5.Enzinger FM, Harvey DA. Spindle cell lipoma. Cancer. 1975;36:1852–9. doi: 10.1002/1097-0142(197511)36:5<1852::aid-cncr2820360542>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 6.Fletcher CD, Martin-Bates E. Spindle cell lipoma: A clinicopathological study with some original observations. Histopathology. 1987;11:803–17. doi: 10.1111/j.1365-2559.1987.tb01884.x. [DOI] [PubMed] [Google Scholar]
- 7.Seifert G, Donath K, Schäfer R. Lipomatous pleomorphic adenoma of the parotid gland. Classification of lipomatous tissue in salivary glands. Pathol Res Pract. 1999;195:247–52. doi: 10.1016/S0344-0338(99)80042-9. [DOI] [PubMed] [Google Scholar]
- 8.Siddaraju N, Singh N, Muniraj F, Jothilingam P, Kumar S, Basu D, et al. Preoperative cytodiagnosis of pleomorphic adenoma with extensive lipometaplasia: A case report. Acta Cytol. 2009;53:457–9. doi: 10.1159/000325353. [DOI] [PubMed] [Google Scholar]