

Abstract
Objective
MicroRNA plays a vital role in gene expression, and microRNA dysregulation is involved in carcinogenesis. The miR-196a-2 polymorphism rs11614913 is reportedly associated with cancer susceptibility. This meta-analysis was performed to assess the overall association of miR-196a-2 with cancer risk.
Methods
A total of 27 independent case-control studies involving 10,435 cases and 12,075 controls were analyzed for the rs11614913 polymorphism.
Results
A significant association was found between rs11614913 polymorphism and cancer risk in four genetic models (CT vs. TT, OR=1.15, 95%CI=1.05–1.27; CC vs. TT, OR=1.23, 95%CI=1.08–1.39; Dominant model, OR=1.17, 95%CI=1.06–1.30; Additive model, OR=1.08, 95%CI=1.01–1.14). In the subgroup analysis of different tumor types, the C allele was associated with increased risk of lung, breast, and colorectal cancer, but not with liver, gastric, or esophageal cancer. In the subgroup analysis by ethnicity, a significantly increased risk of cancer was found among Asians in all genetic models, but no associations were found in the Caucasian subgroup.
Conclusions
The meta-analysis demonstrated that the miR-196a-2 polymorphism is associated with cancer susceptibility, especially lung cancer, colorectal cancer, and breast cancer among Asian populations.
KEY WORDS: MIRN196 microRNA, human, polymorphism, neoplasms, meta-analysis
Introduction
Cancer, as a major public health problem, is reportedly one of the leading causes of death worldwide [1]. Moreover, cancer is a very complex genetic disease, the mechanism of which has not been completely elucidated. Studies have suggested that cancer development results from gene–environment interactions [2]. The presence of high-frequency low-penetrance susceptibility genes may be important in carcinogenesis.
MicroRNA (miRNA) are 21 to 24 nucleotide-long, single-stranded, non-coding RNA. These evolutionarily highly conserved miRNA play vital roles in the regulation of gene expression through mRNA cleavage or translational repression [3,4]. To date, 678 human miRNA have been characterized; they regulate the expression of approximately one-third of human genes[5,6]. miRNA are possibly involved in many biological processes, including cell differentiation, proliferation, and apoptosis [7]. Evidences also suggest that miRNA may play important roles in tumor development and prognosis [8,9].
Two types of single nucleotide polymorphisms (SNPs) were discovered in miRNA genes based on their location. One type is located in the mature regions of the miRNA and the other is located in the pre-miRNA regions. The former may directly regulate both the binding to target mRNA and pre-miRNA maturation, whereas the latter may only influence the maturation of pre-miRNA [10,11].
The SNPs in pre-miRNA have drawn increasing attention because they influence the maturation of miRNA, and they play potential roles in tumor development and progression[12]. In 2008, Hu et al. [13] identified a polymorphism in miR-196a-2 with a T to C change (rs11614913). Rs11614913 is located in the 3′ passenger (3p) strand mature sequence of miR-196a-2. This functional polymorphism is reportedly associated with the susceptibility of various tumors, including lung cancer [14,15] and breast cancer [16], and with lower survival rates of non-small cell lung cancer [13], gliomas [17], gastric cancer [18], gallbladder cancer [19], head and neck cancer [20], esophageal cancer [21], and hepatocellular carcinoma [22,23]. Since then, many epidemiologic studies have examined the associations between SNPs and the risks of various cancers in diverse racial/ethnic populations. However, the results of these studies are inconclusive because of their small sample size or lack of replication. Therefore, this meta-analysis was employed to investigate the association of the miR-196a-2 rs11614913 polymorphism with cancer risk.
Materials and Methods
Literature search
A meta-analysis was conducted based on all case-control studies that examined the association between miR-196a2 rs11614913 polymorphism and cancer risk. The terms rs11614913, polymorphism, and cancer were used to search in the PubMed, EMBASE, Cochran library, and Web of Knowledge databases. The last search was completed on January 31, 2012. No language restrictions were imposed in the meta-analysis. Two independent investigators performed the search, Zhang H and Su YL. The studies that fulfilled the inclusion criteria were selected for evaluation. A manual search was also conducted through reviewing the references cited by the selected articles.
Inclusion criteria
The inclusion criteria for our meta-analysis were as follows: (1) a case-control study design; (2) an association reported between miR-196a2 rs11614913 polymorphism and cancer risk; (3) number of subjects in each genotype available or sufficient allele frequencies for estimating odds ratio (OR), and 95% confidence interval (CI).
Data extraction
Two independent investigators evaluated all the studies selected and extracted the data as shown in Table 1. When a discrepancy was found, a third investigator was invited for discussion until a consensus was reached. The extracted data included the name of the first author, year of publication, country origin, ethnicity, cancer type, source of controls (population- or hospital-based), total number of cases and controls, and the number of different genotypes in the respective cases and controls.
Table 1. Characteristics of studies included in the meta-analysis.
| No. | Study | Year | Ethnicity | Cancer type | Source of controll† | Genotyping method | HWE control | Case |
Control |
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TT | CT | CC | TT | CT | CC | ||||||||||
| 1 | Min KT [24] | 2011 | Asian | colorectral | PB | PCR-RFLP | 0.633 | 125 | 201 | 120 | 148 | 254 | 100 | ||
| 2 | Zhang M [25] | 2011 | Asian | breast | PB | PCR-RFLP | 0.904 | 148 | 89 | 11 | 133 | 93 | 17 | ||
| 3 | Zhan JF [26] | 2011 | Asian | colorectral | HB | PCR-RFLP | 0.849 | 56 | 128 | 68 | 163 | 267 | 113 | ||
| 4 | Zhou B [27] | 2011 | Asian | squamous cell cancer | HB | PCR-RFLP | 0.077 | 57 | 123 | 46 | 82 | 169 | 58 | ||
| 5 | Hong YS [14] | 2011 | Asian | lung | HB | TaqMan | 0.163 | 96 | 224 | 86 | 134 | 198 | 96 | ||
| 6 | Zhang XW [28] | 2011 | Asian | hepatocellular | PB | PIRA-PCR | 0.52 | 277 | 449 | 208 | 477 | 817 | 328 | ||
| 7 | Zhu LJ [29] | 2011 | Asian | colorectral | NC | TaqMan | 0.79 | 130 | 303 | 140 | 172 | 295 | 121 | ||
| 8 | Chen H [30] | 2011 | Asian | colorectral | HB | PCR-LDR | 0.788 | 35 | 64 | 27 | 107 | 206 | 94 | ||
| 9 | Okubo M [31] | 2010 | Asian | gastric | HB | PCR-RFLP | 0.51 | 166 | 281 | 105 | 223 | 350 | 124 | ||
| 10 | Dou T [17] | 2010 | Asian | glioma | HB | PCR-LDR | 0.119 | 189 | 343 | 111 | 208 | 305 | 143 | ||
| 11 | Wang K [32] | 2010 | Asian | esophageal | NC | SNaPshot | 0.6 | 48 | 262 | 148 | 111 | 250 | 128 | ||
| 12 | Peng S [18] | 2010 | Asian | gastric | HB | PCR-RFLP | 0.936 | 43 | 94 | 76 | 50 | 107 | 56 | ||
| 13 | Qi P [33] | 2010 | Asian | hepatocellcular | NC | PCR-LDR | 0.793 | 159 | 286 | 115 | 102 | 197 | 92 | ||
| 14 | Tian T [15] | 2009 | Asian | lung | PB | PCR-RFLP | 0.7 | 293 | 512 | 253 | 307 | 519 | 209 | ||
| 15 | Hu Z [34] | 2009 | Asian | breast | PB | PCR-RFLP | 0.207 | 287 | 483 | 239 | 358 | 517 | 218 | ||
| 16 | Li XD [22] | 2010 | Asian | hepatocellcular | HB | PCR-RFLP | 0.402 | 82 | 150 | 78 | 78 | 102 | 42 | ||
| 17 | Kim JM [35] | 2010 | Asian | lung | PB | PCR-MCS | 0.6 | 162 | 305 | 187 | 185 | 300 | 155 | ||
| 18 | Jedlinski DJ [36] | 2011 | Caucasion | breast | PB | PCR-RFLP | 0.83 | 33 | 86 | 68 | 31 | 82 | 58 | ||
| 19 | Akkiz H [23] | 2011 | Caucasion | hepatocellular | HB | PCR-RFLP | 0.492 | 22 | 86 | 77 | 40 | 87 | 58 | ||
| 20 | Mittal RD [37] | 2011 | Caucasion | bladder | HB | PCR-RFLP | 0.003 | 5 | 131 | 76 | 14 | 127 | 109 | ||
| 21 | George GP [38] | 2011 | Caucasion | prostate | PB | PCR-RFLP | 0.002 | 3 | 101 | 55 | 10 | 114 | 106 | ||
| 22 | Liu Z [20] | 2010 | Caucasion | head and neck | HB | PCR-RFLP | 0.737 | 194 | 565 | 350 | 202 | 545 | 383 | ||
| 23 | Srivastava K [19] | 2010 | Caucasion | gallbladder | PB | PCR-RFLP | 0.068 | 16 | 95 | 119 | 19 | 75 | 136 | ||
| 24 | Catucci I [39] | 2010 | Caucasion | breast | NC | TaqMan | 0.708 | 244 | 842 | 766 | 377 | 1246 | 1116 | ||
| 25 | Hoffman AE [16] | 2009 | Caucasion | breast | NC | Sequenom MassARRAY | 0.583 | 36 | 209 | 181 | 71 | 229 | 166 | ||
| 26 | Ye Y [21] | 2008 | Caucasion | esophageal | HB | SNPlex assay | 0.477 | 83 | 141 | 83 | 59 | 172 | 107 | ||
| 27 | Vinci S [40] | 2011 | Caucasion | lung | NC | HRMA | 0.267 | 12 | 54 | 35 | 10 | 61 | 58 | ||
†, HB:hospital-based; PB:population-based; NC:not clear.
Statistical analysis
The consistency of the data with the Hardy–Weinberg equilibrium (HWE) was determined using a χ2 test after comparing the observed and expected genotypic frequencies in the control populations; a P-value <0.05 was considered statistically significant (Table 1).
The association between miR-196a-2 polymorphism and cancer risk was evaluated by calculating the pooled OR and 95% CI. A Z-test was used to determine the significance of the pooled OR, and P<0.05 was considered statistically significant. The meta-analysis examined the SNP associations in the following models: the co-dominant model (TT vs. CC and CT vs. CC); the dominant model (TT+CT vs. CC), and the recessive model (TT vs. CC+CT).
The χ2-based Q test was used to detect heterogeneity, and I2 index was adopted to measure the extent of heterogeneity [41,42]. A P-value>0.10 [43] in the Q test indicates a lack of heterogeneity among the selected studies. If no heterogeneity was found, the Mantel–Haenszel method was used to estimate the pooled OR of all individual studies in a fixed-effect model [44]. Otherwise the random-effect model (the DerSimonian and Laird method) [44] was used when heterogeneity was observed among the selected studies.
Publication bias was evaluated using the funnel plot wherein the standard error of log(OR) for each study was plotted against its log (OR). The asymmetry of a funnel plot was determined using the Begg’s rank correlation test [45]. Furthermore, the Egger’s linear regression test was used [46] to measure the association between the mean effect estimate and its variance. Subgroup analyses were also performed according to the cancer types and ethnicity. If a cancer type was evaluated only by one study, this was grouped as “other cancer.” The ethnicity was categorized into Asian and Caucasian descent. Moreover, sensitivity analyses were conducted to examine the robustness of the results by excluding one study at a time and recalculating the combined OR and 95%CI of the remaining studies.
All of the analyses were conducted using the STATA software (version 11.0; StataCorp, College Station, TX) and Review Manager (version 5.0.0; The Cochrane Collaboration, Oxford, England), with two-sided P-values.
Results
Characteristics of the studies
A total of 39 articles were initially identified through database searches using different key words and their combinations. After reading the titles and abstracts of the identified articles, the studies that did not meet the inclusion criteria were excluded. During data extraction, additional articles that did not have allelic frequencies available for analysis were also disqualified. Eligible studies were retrieved for detailed full-text evaluation. Manual searches were also done and one relevant article from the references of selected studies was identified. Finally, 27 independent case-control studies [14-40], involving 10,435 cases and 12,075 controls, were included in the meta-analysis for rs11614913. Figure 1 shows the identification and selection of studies.
Figure 1.

Flow diagram of the identification of studies.
The characteristics of the eligible studies are summarized in Table 1. As shown in the table, 10 studies involved Caucasians and 17 involved Asians. Four studies focused on the association of SNPs with lung cancer, 4 with liver cancer, 5 with breast cancer, 4 with colorectal cancer, 2 with gastric cancer, 2 with esophageal cancer, and the remaining 6 studies were associated with other types of cancer. Up to 12 studies used hospital-based controls and 9 used population-based controls. The control sources for the other 6 studies were not identified clearly. The main genotyping method was polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP), which was used in 15 studies. The other genotyping methods employed included MassARRAY, Taqman, DNA sequencing, and high-resolution melting analysis. One study was published in 2008, 3 in 2009, 11 in 2010, and 13 in 2011.
Quantitative synthesis
Minor allele frequencies (MAF) were calculated in the control groups of each study to estimate the racial difference. Figure 2 shows the significant difference (C as the minor allele) in MAF distribution of miR-196a-2 rs11614913 T>C polymorphism among the controls of the different races: Asians and Caucasians. Specifically, the mean MAF in 17 Asian studies was 0.451±0.013. The mean MAF was 0.637+0.020 in the 10 Caucasian studies. The distribution of rs11614913 genotypes in the control subjects followed the HWE in all studies except 2, reported by Mittal et al. [37] and by George et al. [38] (Table 1).
Figure 2.
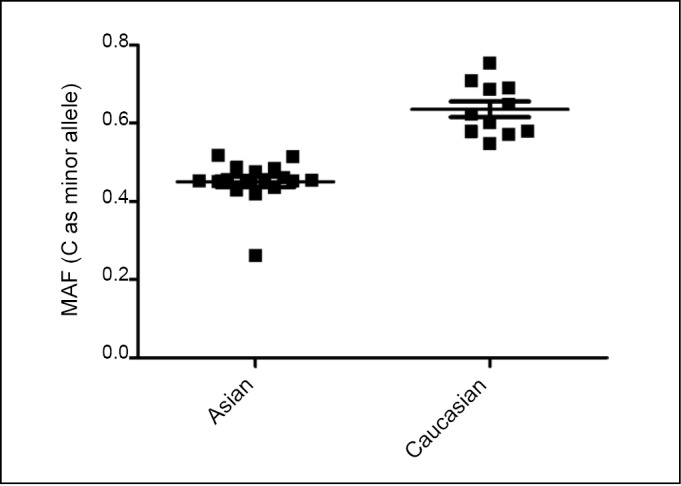
miR-196a-2 rs11614913 MAF distribution in different ethnicity.
Meta-analysis results
The associations of the miR-196a-2 polymorphism with the risk of developing different cancer types among the different racial groups are shown in Table 2. In the meta-analysis of all studies, the rs11614913 polymorphism was significantly associated with the risk of cancer in 4 genetic models (CT vs. TT, OR=1.15, 95%CI=1.05–1.27; CC vs. TT, OR=1.23, 95%CI=1.08–1.39; Dominant model, OR=1.17, 95%CI=1.06–1.30; Additive model, OR=1.08, 95%CI=1.01–1.14).
Table 2. Combined ORs (95% CI) of subgroups for miR-196a-2 rs11614913.
| Subgroup | No. of study | CC vs. TT |
CT vs. TT |
Dominant modela |
Recessive modelb |
Additive modelc |
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | ||
| Total | 27 | 1.23(1.08-1.39)r | <0.00001 | 1.15(1.05-1.27)r | 0.0002 | 1.17(1.06-1.30)r | <0.0001 | 1.06(0.97-1.16)r | <0.0001 | 1.08(1.01-1.14)r | <0.00001 |
| Cancer Type | |||||||||||
| Lung | 4 | 1.26(1.07-1.49)f | 0.26 | 1.15(1.00-1.33)f | 0.13 | 1.19(1.04-1.36)f | 0.21 | 1.07(0.85-1.35)r | 0.07 | 1.12(1.03-1.22)f | 0.15 |
| Liver | 4 | 1.31(0.87-1.95)r | 0.006 | 1.11(0.87-1.43)r | 0.08 | 1.19(0.88-1.61)r | 0.01 | 1.17(0.91-1.49)r | 0.07 | 1.14(0.93-1.40)r | 0.006 |
| Breast | 5 | 1.23(0.92-1.65)r | 0.01 | 1.11(0.98-1.25)f | 0.13 | 1.15(0.93-1.42)r | 0.03 | 1.10(1.00-1.21)f | 0.15 | 1.09(0.96-1.24)r | 0.02 |
| Colorectrol | 4 | 1.44(1.18-1.75)f | 0.28 | 1.17(0.99-1.38)f | 0.19 | 1.25(1.06-1.46)f | 0.20 | 1.30(1.10-1.53)f | 0.38 | 1.20(1.08-1.32)f | 0.28 |
| Gastric | 2 | 1.24(0.94-1.65)f | 0.31 | 1.07(0.85-1.34)f | 0.85 | 1.12(0.90-1.39)f | 0.70 | 1.22(0.96-1.55)f | 0.16 | 1.12(0.98-1.28)f | 0.23 |
| Esophageal | 2 | 1.22(0.26-5.72)r | <0.00001 | 1.19(0.29-4.81)r | <0.00001 | 1.20(0.28-5.11)r | <0.00001 | 1.05(0.63-1.74)r | 0.02 | 1.05(0.55-2.00)r | <0.00001 |
| Other | 6 | 0.98(0.82-1.16)f | 0.63 | 1.19(1.02-1.38)f | 0.29 | 1.10(0.96-1.27)f | 0.53 | 0.82(0.73-0.92)f | 0.33 | 0.95(0.88-1.02)f | 0.78 |
| Ethnicity | |||||||||||
| Asian | 17 | 1.27(1.11-1.46)r | 0.001 | 1.16(1.04-1.28)r | 0.005 | 1.19(1.07-1.32)r | 0.002 | 1.15(1.04-1.27)r | 0.03 | 1.12(1.05-1.20)r | 0.005 |
| Caucasian | 10 | 1.14(0.86-1.51)r | 0.0005 | 1.18(0.92-1.51)r | <0.00001 | 1.16(0.90-1.50)r | 0.0007 | 0.93(0.79-1.08)r | 0.004 | 0.98(0.87-1.11)r | 0.0004 |
| Control Source | |||||||||||
| PB | 9 | 1.24(1.11-1.39)f | 0.53 | 1.04(0.95-1.14)f | 0.46 | 1.10(1.01-1.20)f | 0.47 | 1.09(0.93-1.27)r | 0.008 | 1.07(0.99-1.16)r | 0.07 |
| HB | 12 | 1.18(0.96-1.47)r | 0.0009 | 1.17(1.00-1.37)r | 0.01 | 1.17(0.99-1.38)r | 0.003 | 1.03(0.89-1.20)r | 0.006 | 1.07(0.97-1.19)r | 0.0008 |
| NC | 6 | 1.33(0.90-1.95)r | <0.00001 | 1.32(0.98-1.78)r | 0.0003 | 1.32(0.96-1.83)r | <0.0001 | 1.09(0.92-1.29)r | 0.03 | 1.11(0.95-1.31)r | <0.0001 |
| Lab test method | |||||||||||
| PCR-RFLP | 15 | 1.27(1.15-1.41)f | 0.12 | 1.11(1.02-1.21)f | 0.35 | 1.16(1.07-1.25)f | 0.24 | 1.10(0.95-1.26)r | 0.0004 | 1.09(1.01-1.18)r | 0.005 |
| Others | 12 | 1.14(0.92-1.41)r | <0.00001 | 1.17(0.98-1.39)r | <0.00001 | 1.16(0.97-1.39)r | <0.00001 | 1.03(0.92-1.16)r | 0.01 | 1.06(0.96-1.16)r | <0.0001 |
Ph: P-value of Q-test for heterogeneity test; a, Dominant model (CT+CC vs. TT); b, Recessive model(CC vs. TT+CT); c, Additive model(C vs. T); f, fixed model; r, random model.
The tumor type, race, control source, and lab test methods were adjusted as confounding factors in the overall analysis. Subgroup analysis was performed according to different tumor types, racial groups, control sources, and genotyping methods. In the subgroup analysis of tumor types, the C allele was associated with increased risks for lung cancer, breast cancer, and colorectal cancers, but was not associated with those for liver cancer, gastric cancer, and esophageal cancers. A significant association with lung cancer was observed in all genetic models (CC vs. TT, OR=1.26, 95%CI=1.07–1.49; CT vs. TT, OR=1.15, 95%CI=1.00–1.33; Dominant model, OR=1.19, 95%CI=1.04–1.36; Additive model, OR=1.12, 95%CI=1.03–1.22) except for the recessive model. Similarly, statistically significant associations were found for colorectal cancer in all models (CC vs. TT, OR=1.44, 95%CI=1.18–1.75; Dominant model, OR=1.25, 95%CI=1.06–1.46; Recessive model, OR=1.30, 95%CI=1.10–1.53; Additive model, OR=1.20, 95%CI=1.08–1.32). In breast cancer, the CC genotype was associated significantly with increased risk when compared with TT and CT genotype.
In the subgroup analysis of race, statistically significant associations with increased cancer risk were found among Asians in all genetic models. Specifically, the OR (95%CI) was 1.27 (1.11-1.46) for CC vs. TT, 1.16 (1.04-1.28) for CT vs. TT, 1.19 (1.07-1.32) for CT+CC vs. TT, 1.15 (1.04-1.27) for CC vs. CT+TT, and 1.12 (1.05-1.20) for C allele vs. T allele. However, no significant association was found for Caucasians in any of the genetic models.
In the subgroup analysis of the control source, the CC genotype was associated with cancer when the study used a population-based control (CC vs. TT, OR=1.24, 95%CI=1.11-1.39; Dominant model, OR=1.10, 95%CI=1.01-1.20). Nevertheless, the CT genotype was marginally associated with cancer risk in the hospital-based control subgroup (CT vs. TT, OR=1.17, 95%CI=1.00-1.37).
Subgroup analysis was also performed based on different genotyping methods. Statistically significant associations with increased cancer risk were found in the PCR-RFLP subgroup in all genetic models except for the recessive model. Specifically, OR (95%CI) was 1.27 (1.15-1.41) for CC vs. TT, 1.11 (1.02-1.21) for CT vs. TT, 1.16 (1.07-1.25) for CT+CC vs. TT, and 1.09 (1.01-1.18) for C allele vs.T allele. However, no significant association was found for genotyping methods other than PCR-RFLP in any of the genetic models.
Test of heterogeneity
The heterogeneity of the studies was analyzed in the overall meta-analysis as well as subgroup analysis. The P values in the Q test were also shown in Table 2. The heterogeneity of the study decreased in the subgroup analysis of cancer type. If P>0.10, a fixed-effect model was chosen, otherwise a random-effect model was used.
Sensitivity analysis
In the sensitivity analysis, the meta-analysis was repeated by excluding 1 study each time to assess the influence of the removed study on the pooled ORs. The corresponding pooled ORs were not altered materially for rs11614913 (Figure 3 and Table 3).
Figure 3.

Pooled OR of sensitivity analysis.
Table 3. ORs (95% CI) of sensitivity analysis for rs11614913.
| Omitting literature | CC vs. TT |
CT vs. TT |
Dominant model |
Recessive model |
Additive model |
|||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | |
| All for rs11614913 | 1.23(1.08-1.39) | <0.00001 | 1.15(1.05-1.27) | 0.0002 | 1.17(1.06-1.30) | <0.0001 | 1.06(0.97-1.16) | <0.0001 | 1.08(1.01-1.14) | <0.0001 |
| Ye Y 2008 [21] | 1.26(1.12-1.42) | <0.0001 | 1.18(1.07-1.29) | 0.003 | 1.20(1.09-1.32) | 0.0005 | 1.07(0.98-1.18) | 0.003 | 1.09(1.03-1.16) | <0.0001 |
| Tian T 2009 [15] | 1.22(1.07-1.40) | <0.00001 | 1.16(1.05-1.29) | 0.0002 | 1.18(1.06-1.31) | <0.00001 | 1.05(0.96-1.16) | <0.0001 | 1.07(1.01-1.14) | <0.00001 |
| Hu Z 2009 [34] | 1.22(1.06-1.39) | <0.00001 | 1.16(1.04-1.28) | 0.0002 | 1.17(1.05-1.31) | <0.0001 | 1.05(0.96-1.16) | <0.0001 | 1.07(1.01-1.14) | <0.00001 |
| Hoffman AE 2009 [16] | 1.20(1.06-1.36) | <0.0001 | 1.14(1.03-1.25) | 0.0006 | 1.15(1.05-1.27) | <0.0001 | 1.05(0.96-1.15) | <0.0001 | 1.07(1.00-1.13) | <0.00001 |
| Okubo M 2010 [31] | 1.23(1.08-1.41) | <0.00001 | 1.16(1.05-1.29) | 0.0001 | 1.18(1.06-1.31) | <0.00001 | 1.06(0.97-1.17) | <0.0001 | 1.08(1.01-1.15) | <0.00001 |
| Dou T 2010 [17] | 1.25(1.10-1.42) | <0.00001 | 1.15(1.04-1.28) | 0.0002 | 1.18(1.06-1.31) | <0.00001 | 1.08(0.99-1.18) | 0.002 | 1.08(1.02-1.15) | <0.00001 |
| Wang K 2010 [32] | 1.19(1.05-1.33) | 0.0002 | 1.12(1.02-1.22) | 0.01 | 1.14(1.04-1.24) | 0.002 | 1.05(0.96-1.15) | <0.0001 | 1.06(1.00-1.13) | <0.0001 |
| Peng S 2010 [18] | 1.22(1.07-1.39) | <0.00001 | 1.16(1.05-1.28) | 0.0002 | 1.17(1.06-1.30) | <0.00001 | 1.05(0.96-1.15) | <0.0001 | 1.07(1.01-1.14) | <0.00001 |
| Qi P 2010 [33] | 1.25(1.10-1.42) | <0.00001 | 1.17(1.05-1.29) | 0.0002 | 1.19(1.07-1.32) | <0.0001 | 1.07(0.98-1.18) | <0.0001 | 1.08(1.02-1.15) | <0.00001 |
| Li XD 2010 [22] | 1.21(1.06-1.38) | <0.00001 | 1.15(1.04-1.27) | 0.0002 | 1.16(1.05-1.29) | <0.0001 | 1.05(0.96-1.15) | <0.0001 | 1.07(1.01-1.14) | <0.00001 |
| Kim JM 2010 [35] | 1.22(1.07-1.39) | <0.00001 | 1.16(1.04-1.28) | 0.0001 | 1.17(1.06-1.30) | <0.00001 | 1.05(0.96-1.16) | <0.0001 | 1.07(1.01-1.14) | <0.00001 |
| Liu Z 2010 [20] | 1.24(1.09-1.42) | <0.00001 | 1.16(1.05-1.29) | 0.0001 | 1.18(1.07-1.32) | <0.00001 | 1.07(0.98-1.18) | 0.0001 | 1.08(1.02-1.15) | <0.00001 |
| Srivastava K 2010 [19] | 1.23(1.08-1.40) | <0.00001 | 1.15(1.04-1.27) | 0.0002 | 1.17(1.06-1.30) | <0.00001 | 1.08(0.98-1.18) | 0.0001 | 1.08(1.02-1.15) | <0.00001 |
| Catucci I 2010 [39] | 1.24(1.08-1.42) | <0.00001 | 1.16(1.05-1.29) | 0.0002 | 1.18(1.06-1.32) | <0.00001 | 1.06(0.96-1.17) | <0.0001 | 1.08(1.01-1.15) | <0.00001 |
| Min KT 2011 [24] | 1.22(1.07-1.39) | <0.00001 | 1.17(1.05-1.29) | 0.0002 | 1.18(1.06-1.31) | <0.00001 | 1.05(0.96-1.15) | 0.0001 | 1.07(1.01-1.14) | <0.00001 |
| Zhang M 2011 [25] | 1.24(1.09-1.41) | <0.00001 | 1.17(1.06-1.29) | 0.0003 | 1.19(1.08-1.32) | <0.0001 | 1.07(0.98-1.17) | <0.0001 | 1.08(1.02-1.15) | <0.00001 |
| Zhan JF 2011 [26] | 1.21(1.06-1.38) | <0.00001 | 1.15(1.04-1.27) | 0.0002 | 1.16(1.05-1.29) | <0.0001 | 1.05(0.96-1.15) | <0.0001 | 1.07(1.00-1.14) | <0.00001 |
| Zhou B 2011 [27] | 1.23(1.08-1.40) | <0.00001 | 1.16(1.05-1.28) | 0.0001 | 1.18(1.06-1.31) | <0.00001 | 1.06(0.97-1.16) | <0.0001 | 1.08(1.01-1.15) | <0.00001 |
| Hong YS 2011 [14] | 1.22(1.07-1.40) | <0.00001 | 1.14(1.03-1.26) | 0.0006 | 1.16(1.05-1.29) | <0.0001 | 1.07(0.97-1.17) | <0.0001 | 1.07(1.01-1.14) | <0.00001 |
| Zhang XW 2011 [28] | 1.23(1.08-1.41) | <0.00001 | 1.17(1.06-1.30) | 0.0001 | 1.19(1.07-1.32) | <0.0001 | 1.06(0.96-1.16) | <0.0001 | 1.08(1.01-1.15) | <0.00001 |
| Zhu LJ 2011 [29] | 1.21(1.06-1.38) | <0.00001 | 1.14(1.03-1.27) | 0.0003 | 1.16(1.05-1.29) | <0.0001 | 1.06(0.96-1.16) | <0.0001 | 1.07(1.01-1.14) | <0.00001 |
| Chen H 2011 [30] | 1.24(1.09-1.41) | <0.00001 | 1.16(1.05-1.28) | 0.0002 | 1.18(1.07-1.31) | <0.00001 | 1.07(0.97-1.17) | <0.0001 | 1.08(1.02-1.15) | <0.00001 |
| Jedlinski DJ 2011 [36] | 1.23(1.08-1.40) | <0.00001 | 1.16(1.05-1.28) | 0.0002 | 1.18(1.06-1.31) | <0.00001 | 1.06(0.97-1.16) | <0.0001 | 1.08(1.01-1.15) | <0.00001 |
| Akkiz H 2011 [23] | 1.20(1.06-1.37) | <0.00001 | 1.14(1.04-1.26) | 0.0003 | 1.16(1.05-1.28) | <0.0001 | 1.05(0.96-1.15) | <0.0001 | 1.07(1.01-1.13) | <0.00001 |
| Mittal RD 2011 [37] | 1.22(1.07-1.39) | <0.00001 | 1.14(1.04-1.26) | 0.0004 | 1.17(1.06-1.29) | <0.0001 | 1.08(0.98-1.18) | 0.0001 | 1.08(1.02-1.15) | <0.00001 |
| George GP 2011 [38] | 1.22(1.07-1.39) | <0.00001 | 1.15(1.04-1.27) | 0.0003 | 1.17(1.06-1.29) | <0.00001 | 1.08(0.99-1.18) | 0.0002 | 1.08(1.02-1.15) | <0.00001 |
| Vinci S 2011 [40] | 1.24(1.09-1.41) | <0.00001 | 1.16(1.05-1.28) | 0.0001 | 1.18(1.07-1.31) | <0.0001 | 1.07(0.98-1.17) | <0.0001 | 1.08(1.02-1.15) | <0.00001 |
Ph: P value of Q-test for heterogeneity test.
Publication bias
Begg’s funnel plot and Egger’s test were performed to evaluate the publication bias of the study. The funnel plot for CC vs. TT of miR-196a-2 rs11614913 polymorphism seemed approximately symmetrical (Figure 4). The Egger’s test did not show any evidence of publication bias (t=0.60, df=26, P=0.553).
Figure 4.

Begg’s funnel plot for rs11614913 (CC vs. TT).
Discussion
MiRNAs are important post-transcriptional regulators of gene expression and are reportedly involved in various diseases. Emerging miRNA profiling studies have investigated the differences in miRNA expression between cancer patients and healthy controls. Various miRNAs are upregulated or downregulated in different forms of tumors. However, the regulatory effects of miRNA in cancer occurrence and development are complicated. Although genetic and epigenetic regulation influence miRNA activity, the mechanism of miRNAs involvement in carcinogenesis remains unclear. Considering the extensive regulation of many target genes by miRNA, a single nucleotide polymorphism in the miRNAs gene may affect the expression and activity of various genes or proteins, which further influence the carcinogenic process and tumor progression.
A previous study found 323 SNPs located in 227 human pre-miRNA sequences [10]. Another study integrated 474 human miRNA sequences, and found genetic variants located mainly in the precursor sequences (10%), whereas rare variants were located in the seed region (<1%) [35]. Of these pre-miRNA SNPs, the miR-196a-2 rs11614913 T>C polymorphism is the most studied SNP. This functional polymorphism reportedly has an association with susceptibility to various forms of tumor including lung cancer, breast cancer, glioma, gastric cancer, gallbladder cancer, head and neck cancer, esophageal cancer, hepatocellular carcinoma, as well as shortened survival time in non-small cell lung cancer.
The results of the meta-analysis show that people carrying the variant genotype C have an increased risk of cancer compared to those carrying the wild genotype T. This finding coincides with a previous meta-analysis [47]. The miR-196a-2 polymorphism may play a role in carcinogenesis.
Stratification of the analysis in terms of tumor type revealed that the miR-196a-2 polymorphism was related to lung cancer, colorectal cancer, and breast cancer, but no relationship was seen for liver cancer, gastric cancer, or esophageal cancer. The differences may be attributed to the following: miRNAs may have tissue-specific expression and the same miRNA SNP may play different roles in different tissues, which leads to different degrees of carcinogenesis; the sample size in each subgroup was not large enough to have sufficient study power to generate reliable results. However, our subgroup analysis showed substantial results in accordance with previous studies on various types of cancer. Previous meta-analyses has found that rs11614913 is associated with colorectal cancer risk [48], breast cancer risk[49], and lung cancer risk [47], consistent with the results of our study.
In the subgroup analysis by race, an increased risk of cancer was found among Asians in all genetic models, but not among Caucasians. The distribution of the minor allele in the controls of these populations was also evaluated. Significant differences in the distribution of C allele were observed. Caucasians have a higher frequency of the C allele compared with Asians. This difference in allelic frequency may affect genetic susceptibility in different racial/ethnic groups.
In the subgroup analysis in terms of the control source, the C allele was associated with cancer susceptibility in studies with population-based controls. Moreover, the population-based subgroup was less heterogeneous than the hospital-based subgroup, which indicated that population-based controls are more helpful in reducing the heterogeneity of observational studies.
Finally, the C allele was associated with cancer risk among studies that used PCR-RFLP for genotyping. However, in subgroups using other genotyping methods, no significant association was found. Different genotyping methods may have different capacities for detecting gene polymorphism, which may influence the results. The laboratory test method may be one of the confounding factors in the overall analysis. After adjusting for genotyping method, the rs11614913 C genotype was associated with cancer risk.
Currently, two possibilities explain the association of the miR-196a-2 polymorphism with cancer risk. First, the rs11614913 variant may increase mature miR-196a expression and enhance target mRNA binding [13]. Zhan et al. [26] reported that the miR-196a expression level among C allele carriers was higher than that in those carrying the TT genotype in colorectal cancer. Similarly, Li et al. found increased miR-196a expression among hepatocellular carcinoma patients with Hepatitis B virus infection who carried the C allele [22]. This SNP is associated with G2 cell cycle delay, which plays a vital role in carcinogenesis[17].
The current meta-analysis has several limitations. First, the cancer types included in the analysis were limited. Although the polymorphism and cancer risk in all reported studies were analysed, these studies mainly focused on several tumor types, which may affect the risk estimation. Second, some of the study controls were not from healthy populations. Selection bias could have occurred, which may have confounded the results. Third, the lack of individual information inhibited the calculation needed to adjust the ORs and analyze the gene-environment interaction.
In conclusion, miR-196a-2 polymorphism is associated with cancer risk, especially lung cancer, colorectal cancer, and breast cancer. Asians carrying the miR-196a-2 variant genotype are more susceptible to cancer compared with Caucasians. The SNP in miR-196a-2 may be a key factor in carcinogenesis. Furthermore, well-designed studies involving various ethnic populations and more cancer types are needed to confirm the results. Functional studies are needed to clarify the mechanisms that show the effect of miRNA SNPs on cancer development.
Acknowledgements
This study was supported by the National Natural Science Foundation of China (No. 81071914).
Footnotes
No potential conflicts of interest are disclosed.
References
- 1.Siegel R, Naishadham D, Jemal A: Cancer statistics, 2012. CA Cancer J Clin 2012; 62:10-29 (Epub 2012 Jan 4). [DOI] [PubMed]
- 2.Lichtenstein P, Holm NV, Verkasalo PK, et al. Environmental and heritable factors in the causation of cancer--analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med 2000; 343: 78-85 [DOI] [PubMed] [Google Scholar]
- 3.Lagos-Quintana M, Rauhut R, Lendeckel W, et al. Identification of novel genes coding for small expressed RNAs. Science 2001; 294: 853-858 [DOI] [PubMed] [Google Scholar]
- 4.Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell 2004; 116: 281-297 [DOI] [PubMed] [Google Scholar]
- 5.Bertino JR, Banerjee D, Mishra PJ. Pharmacogenomics of microRNA: a miRSNP towards individualized therapy. Pharmacogenomics 2007; 8: 1625-1627 [DOI] [PubMed] [Google Scholar]
- 6.Lewis BP, Burge CB, Bartel DP. Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell 2005; 120: 15-20 [DOI] [PubMed] [Google Scholar]
- 7.Chen JF, Mandel EM, Thomson JM, et al. The role of microRNA-1 and microRNA-133 in skeletal muscle proliferation and differentiation. Nat Genet 2006; 38: 228-233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gregory RI, Shiekhattar R. MicroRNA biogenesis and cancer. Cancer Res 2005; 65: 3509-3512 [DOI] [PubMed] [Google Scholar]
- 9.Esquela-Kerscher A, Slack FJ. Oncomirs-microRNAs with a role in cancer. Nat Rev Cancer 2006; 6: 259-269 [DOI] [PubMed] [Google Scholar]
- 10.Duan R, Pak C, Jin P.Single nucleotide polymorphism associated with mature miR-125a alters the processing of pri-miRNA. Hum Mol Genet 2007; 16: 1124-1131 [DOI] [PubMed] [Google Scholar]
- 11.Han J, Lee Y, Yeom KH, et al. Molecular basis for the recognition of primary microRNAs by the Drosha-DGCR8 complex. Cell 2006; 125: 887-901 [DOI] [PubMed] [Google Scholar]
- 12.Horikawa Y, Wood CG, Yang H, et al. Single nucleotide polymorphisms of microRNA machinery genes modify the risk of renal cell carcinoma. Clin Cancer Res 2008; 14: 7956-7962 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hu Z, Chen J, Tian T, et al. Genetic variants of miRNA sequences and non-small cell lung cancer survival. J Clin Invest 2008; 118: 2600-2608 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hong YS, Kang HJ, Kwak JY, et al. Association between microRNA196a2 rs11614913 genotypes and the risk of non-small cell lung cancer in Korean population. J Prev Med Public Health; 44: 125-130. [DOI] [PMC free article] [PubMed]
- 15.Tian T, Shu Y, Chen J, et al. A functional genetic variant in microRNA-196a2 is associated with increased susceptibility of lung cancer in Chinese. Cancer Epidemiol Biomarkers Prev 2009; 18: 1183-1187 [DOI] [PubMed] [Google Scholar]
- 16.Hoffman AE, Zheng T, Yi C, et al. microRNA miR-196a-2 and breast cancer: a genetic and epigenetic association study and functional analysis. Cancer Res 2009, 69: 5970-5977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dou T, Wu Q, Chen X, et al. A polymorphism of microRNA196a genome region was associated with decreased risk of glioma in Chinese population. J Cancer Res Clin Oncol 2010; 136: 1853-1859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Peng S, Kuang Z, Sheng C, et al. Association of microRNA-196a-2 gene polymorphism with gastric cancer risk in a Chinese population. Dig Dis Sci 2010; 55: 2288-2293 [DOI] [PubMed] [Google Scholar]
- 19.Srivastava K, Srivastava A, Mittal B.Common genetic variants in pre-microRNAs and risk of gallbladder cancer in North Indian population. J Hum Genet 2010; 55: 495-499 [DOI] [PubMed] [Google Scholar]
- 20.Liu Z, Li G, Wei S, et al. Genetic variants in selected pre-microRNA genes and the risk of squamous cell carcinoma of the head and neck. Cancer 2010; 116: 4753-4760 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ye Y, Wang KK, Gu J, et al. Genetic variations in microRNA-related genes are novel susceptibility loci for esophageal cancer risk. Cancer Prev Res (Phila) 2008; 1: 460-469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li XD, Li ZG, Song XX, et al. A variant in microRNA-196a2 is associated with susceptibility to hepatocellular carcinoma in Chinese patients with cirrhosis. Pathology 2010; 42: 669-673 [DOI] [PubMed] [Google Scholar]
- 23.Akkız H, Bayram S, Bekar A, et al. A functional polymorphism in pre-microRNA-196a-2 contributes to the susceptibility of hepatocellular carcinoma in a Turkish population: a case-control study. J Viral Hepat, 2011; 18: e399-407 [DOI] [PubMed] [Google Scholar]
- 24.Min KT, Kim JW, Jeon YJ, et al. Association of the miR-146aC>G, 149C>T, 196a2C>T, and 499A>G polymorphisms with colorectal cancer in the Korean population. Mol Carcinog (Epub ahead of print). [DOI] [PubMed] [Google Scholar]
- 25.Zhang M, Jin M, Yu Y, et al. Associations of miRNA polymorphisms and female physiological characteristics with breast cancer risk in Chinese population. Eur J Cancer Care (Engl) 2012; 21: 274-80 (Epub 2011 Nov 11). [DOI] [PubMed]
- 26.Zhan JF, Chen LH, Chen ZX, et al. A functional variant in microRNA-196a2 is associated with susceptibility of colorectal cancer in a Chinese population. Arch Med Res 2011; 42: 144-148 [DOI] [PubMed] [Google Scholar]
- 27.Zhou B, Wang K, Wang Y, et al. Common genetic polymorphisms in pre-microRNAs and risk of cervical squamous cell carcinoma. Mol Carcinog, 2011; 50: 499-505 [DOI] [PubMed] [Google Scholar]
- 28.Zhang XW, Pan SD, Feng YL, et a. Relationship between genetic polymorphism in microRNAs precursor and genetic predisposition of hepatocellular carcinoma. Zhonghua Yu Fang Yi Xue Za Zhi 45: 239-243. [PubMed]
- 29.Zhu L, Chu H, Gu D, et al. A Functional Polymorphism in miRNA-196a2 Is Associated with Colorectal Cancer Risk in a Chinese Population. DNA Cell Biol 2012; 31: 349-353 (Epub 2011 Aug 4). [DOI] [PubMed]
- 30.Chen H, Sun LY, Chen LL, et al. A variant in microRNA-196a2 is not associated with susceptibility to and progression of colorectal cancer in Chinese. Intern Med J 2012; 42: e115-119 [DOI] [PubMed] [Google Scholar]
- 31.Okubo M, Tahara T, Shibata T, et a. Association between common genetic variants in pre-microRNAs and gastric cancer risk in Japanese population. Helicobacter 2010; 15: 524-531 [DOI] [PubMed] [Google Scholar]
- 32.Wang K, Guo H, Hu H, et al. A functional variation in pre-microRNA-196a is associated with susceptibility of esophageal squamous cell carcinoma risk in Chinese Han. Biomarkers, 2010; 15: 614-618 [DOI] [PubMed] [Google Scholar]
- 33.Qi P, Dou TH, Geng L, et al. Association of a variant in MIR 196A2 with susceptibility to hepatocellular carcinoma in male Chinese patients with chronic hepatitis B virus infection. Hum Immunol 2010; 71: 621-626 [DOI] [PubMed] [Google Scholar]
- 34.Hu Z, Liang J, Wang Z, et al. Common genetic variants in pre-microRNAs were associated with increased risk of breast cancer in Chinese women. Hum Mutat 2009; 30: 79-84 [DOI] [PubMed] [Google Scholar]
- 35.Kim MJ, Yoo SS, Choi YY, et al. A functional polymorphism in the pre-microRNA-196a2 and the risk of lung cancer in a Korean population. Lung Cancer 2010; 69: 127-129 [DOI] [PubMed] [Google Scholar]
- 36.Jedlinski DJ, Gabrovska PN, Weinstein SR, et al. Single nucleotide polymorphism in hsa-mir-196a-2 and breast cancer risk: a case control study. Twin Res Hum Genet 2011; 14: 417-421 [DOI] [PubMed] [Google Scholar]
- 37.Mittal RD, Gangwar R, George GP, et al. Investigative role of pre-microRNAs in bladder cancer patients: a case-control study in North India. DNA Cell Biol, 2011; 30: 401-406 [DOI] [PubMed] [Google Scholar]
- 38.George GP, Gangwar R, Mandal RK, et al. Genetic variation in microRNA genes and prostate cancer risk in North Indian population. Mol Biol Rep 2011; 38: 1609-1615 [DOI] [PubMed] [Google Scholar]
- 39.Catucci I, Yang R, Verderio P, et al. Evaluation of SNPs in miR-146a, miR196a2 and miR-499 as low-penetrance alleles in German and Italian familial breast cancer cases. Hum Mutat 2010; 31: E1052-1057 [DOI] [PubMed] [Google Scholar]
- 40.Vinci S, Gelmini S, Pratesi N, et al. Genetic variants in miR-146a, miR-149, miR-196a2, miR-499 and their influence on relative expression in lung cancers. Clin Chem Lab Med 2011; 49: 2073-2080 [DOI] [PubMed] [Google Scholar]
- 41.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: 1539-1558 [DOI] [PubMed] [Google Scholar]
- 42.Huedo-Medina TB, Sanchez-Meca J, Marin-Martinez F, et al. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods 2006; 11: 193-206 [DOI] [PubMed] [Google Scholar]
- 43.Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Intern Med 1997; 127: 820-826 [DOI] [PubMed] [Google Scholar]
- 44.Mantel N, Haenszel W.Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 1959; 22: 719-748 [PubMed] [Google Scholar]
- 45.Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994; 50: 1088-1101 [PubMed] [Google Scholar]
- 46.Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315: 629-634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Saunders MA, Liang H, Li WH. Human polymorphism at microRNAs and microRNA target sites. Proc Natl Acad Sci USA 2007; 104: 3300-3305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Chu H, Wang M, Shi D, et al. Hsa-miR-196a2 Rs11614913 polymorphism contributes to cancer susceptibility: evidence from 15 case-control studies. PLoS One 2011; 6: e18108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Guo J, Jin M, Zhang M, et al. A Genetic Variant in miR-196a2 Increased Digestive System Cancer Risks: A Meta-Analysis of 15 Case-Control Studies. PLoS One 2012; 7: e30585. [DOI] [PMC free article] [PubMed] [Google Scholar]