

Abstract
Purpose of review
Recent technological advances have allowed the in-vivo measurement of impacts sustained to the head during helmeted sports. These measurements are of interest to researchers and clinicians for their potential to understand both the underlying mechanics of concussive injuries and the potential for real-time injury diagnostics. Following an overview of impact biomechanics, this review will evaluate the following: in-vivo technology being used in American football players; impact frequencies and magnitudes; and the biomechanical threshold for concussion.
Recent findings
The average high school athlete sustains over 650 impacts in a season, and the level at which concussion occurs is approximately 100 g and 5500 rad/s/s.
Summary
High school athletes sustain a significant number of head impacts each year. The impacts are similar in both volume and magnitude when compared with collegiate athletes. The magnitude of impact that results in concussion is also the same at both levels of play, although the collegiate athlete may have a higher injury tolerance.
Introduction
The number of concussions occurring during sport participation has been estimated at just under 4 million injuries annually [1]. This figure includes the estimated 50% of injuries that go unreported to medical personnel, coaching staff, or parents [2]. Whereas considerable research has focused on the acute effects of concussion and return-to-play decision-making, perhaps one of the most difficult aspects of concussion management is injury identification. Novel technology is now available that permits the in-vivo tracking of all impacts to the head in helmeted sports. With this methodology comes the possibility of real-time biomechanical based injury diagnostics and injury prevention. That is, should researchers identify the appropriate magnitude for a set of biomechanical variables then athletes could be promptly removed from athletic participation following a blow to the head. In addition, research utilizing these technologies has the potential to improve athletic equipment, thereby decreasing injury risk. This review will focus on the application of recently developed helmet-based impact sensing technology in adolescent American football players.
Impact biomechanics
Concussions occur as a result of a direct or indirect force that is applied to the head that results in the sudden acceleration/deceleration of the brain [3]. In general, it is not the velocity of the athlete or the force of impact that is being measured, but rather the change in velocity or acceleration of the cranium that is measured by helmet-based sensors. This concept is most easily explained using the Newtonian Laws of Motion. Mathematically, Newton’s second law of motion states that a force (F) is equal to the mass (m) of an object multiplied by the acceleration (a) of that object (F¼ma). When applied to athletics, or more specifically football, this equation presents the simplest conceptual quantification of a striking and struck player. Indeed, as the magnitude force from the striking player increases, the head acceleration of the struck player must increase as the mass of the head is fixed. The F¼ma formula is used to calculate linear acceleration – change in velocity occurring in a straight line; but an analogous equation (T¼Ia) is available to calculate rotational acceleration – change in angular velocity around a fixed point. It is believed that linear acceleration is more directly involved in the compression of cerebral tissue following impact, whereas rotational acceleration is more related to shearing of the cerebral neurons. While each may have a distinct influence on injury, there is no clear indication that one plays a bigger role in predicting concussion or concussion severity than the other. Linear acceleration has been suggested by some to be the primary injury predictor [4]; others have indicated that rotational acceleration is the most important [5], and still others have suggested an equal role of both [6,7]. Notably, the current technology used to measure these variables on the athletic field is recording the acceleration of the skull at the center of mass, which is presumed to be the acceleration of the cerebral tissue. Direct measures of cerebral tissue acceleration following an impact are not available at this time.
The evaluation of real-world impacts can also be considered in terms of momentum conservation during the impact. The law of conservation of momentum states that the momentum of the system (e.g. both the striking and stuck players) must be the same before and after the impact. Although some energy is lost to absorption of protective equipment, a transfer of energy will take place between the two athletes. Depending on the point of contact, the energy will be transferred to various parts of the body or isolated to the head (i.e. helmet to helmet contact). The momentum of one athlete is equal to his mass times velocity, whereas the momentum for two athletes colliding can be expressed as:
where m1 and m2 are the mass of athletes 1 and 2, respectively; v1 and v2 are the velocities of athletes 1 and 2 prior to the collision; v3 and v4 are their velocities after the collision.
The equation presented above outlines the most simplistic form of collision whereby all body segments of both athletes are functioning as a single rigid mass at the moment of impact. Realistically, however, this never occurs as the body is comprised of multiple rigid objects (i.e. bones) linked together at joints by soft tissue (i.e. muscle, ligaments, etc.). Although not perfect stabilizers, muscles contracted at the moment of impact will stabilize those joints, allowing the mass from multiple segments to be summed. The summed mass of each linked body segment is termed the effect mass at the moment of impact. For example, if it is assumed that the striking athlete contracts his neck musculature and aligns his head, neck, and spine, then m1 in the equation above would be his full body weight (e.g. 100 kg). Conversely, if the struck athlete does not have his neck musculature contracted at the moment of head impact, then m2 can be divided into m2t (torso mass of 95 kg) and m2h (head mass of 5 kg) and the new equation would read:
or
At the moment of a helmet-to-helmet impact, the full momentum of athlete 1 is transferred to the head (m2h) of athlete 2. In turn, the velocity of the head (v5) must increase to maintain a balanced equation. The greater change in velocity between the pre-impact and post-impact state represents a greater acceleration value and thus places the athlete at greater risk for concussion. This theory has been demonstrated in the laboratory with concussions reconstructed from video footage collected during professional football games [8]. The investigation reported that when the struck player increased his neck tension, and thus the effective mass at impact, there was a 35% reduction in concussion risk. Similarly, the striking athlete is also able to increase his effective mass and momentum transfer by 67% by aligning the head, neck, and torso [9]. Using animal models, others demonstrated how increasing the effective mass at impact can reduce concussion risk.
For example, when the head of a rhesus monkey was allowed to rotate freely following impact, concussion commonly occurred. Yet, when the head was secured externally, no concussion occurred with the application of an equivalent force [5]. Incomparable work, the application of electrical stimulation to the neck musculature of a cat is sufficient to stabilize the head and prevent concussion [10]. While the discussion above presents the scenario of helmet-to-helmet contact, it is important to note that, if the tackling maneuver is carried out appropriately with the initial point of contact at the chest, then less momentum is transferred to the head and the post-impact velocity of the head is reduced.
Neck muscle strength and activation has the potential to reduce cranial and brain acceleration in most sports settings. Some sports, however, benefit from protective equipment that can further reduce impact magnitude. Sporting helmets are designed to prevent more severe cranial injuries (e.g. skull fracture), not to prevent concussive injuries. Indeed, no helmet can completely eliminate concussion risk, but they may be effective in reducing direct energy transfer between an object and the athlete’s head. Helmets function to reduce impact forces by increasing the impact duration through padding. Similarly to a car airbag, as the duration of the impact is increased, the resulting acceleration will decrease. Referring back to Newton’s second law (i.e. F¼ma), as time increases then acceleration will decrease (a¼Dv/Dt). This concept was demonstrated by evaluating the impact characteristics of suspension style and padded football helmets, whereby the padded helmet demonstrated lower peak acceleration, but longer impact duration than the suspension style helmets [11].
The discussion presented here is intended to provide a basic understanding of concussion biomechanics. In no way does this background information capture the complexity of the injury or all of the factors that influence injury susceptibility. Indeed, concussion susceptibility likely involves more than just biomechanical variables. For example, some have speculated that, in addition to athlete size, strength, equipment, impact direction, impact readiness, and anatomical factors, variables such as hydration, fatigue, and genetic profile may all play a role. Regardless, the ensuing sections will summarize what is known about impact biomechanics and how that may influence the risk for injury.
In-vivo head impact monitoring technology
Although a significant amount of laboratory-based research on concussion biomechanics has been conducted, the ability to measure impacts on the field in vivo is relatively new. The Head Impact Telemetry (HIT) System (Simbex, Lebanon, NH) is a wireless accelerometer array capable of tracking head impact location and magnitude in helmeted events. The device consists of two units: the encoder located within the helmet and a sideline computer. The encoder contains six thimble-sized, single-axis accelerometers recording at 1000 Hz, a telemetry unit, data storage device, and battery pack. The memory device can record and store 100 impacts when out of range of the sideline computer. The components are sealed in waterproof plastic and retrofitted between the pads of any standard Riddell football helmet (Fig. 1). At the time of impact, data are transmitted to a sideline computer and stored for later analysis. The sideline computer is capable of receiving impact data from up to 100 players up to 150 yards away. Importantly, those athletes who are involved with the majority of plays (i.e. linemen), but whose impacts are obscured from video capture, can be monitored. The data available from the software contain all pertinent impact data including peak linear acceleration, rotational acceleration, impact duration, location, time stamp, Gadd Severity Index [12], and the head injury criterion (HIC). HIT System-equipped helmets look and function identically to other helmets and meet National Operating Committee on Standards for Athletic Equipment safety standards.
Figure 1.
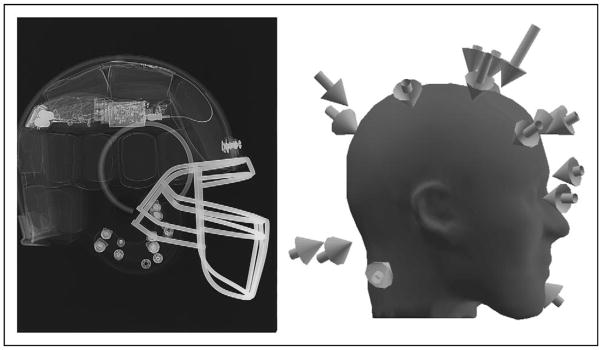
X-ray image showing the HIT System encoder located along the crown of a Riddell helmet. Arrows around the red headform indicate individual impacts with tail length suggesting magnitude. 40 ms of data are recorded as representative of the impact: 12 ms prior to impact and the 28 ms following. HIT, Head Impact Telemetry.
Drawing from the literature employing the HIT System, the following sections will review the current literature on sub-concussive head impact frequency and magnitude and the potential for a concussion threshold in adolescent athletes.
Head impact frequencies and magnitudes
The ability to capture the number of impacts to the head occurring during participation in football is relatively new. A number of investigations have evaluated impact incidence at the collegiate level, but research at this level largely ignores the substantial number of high school athletes. Surprisingly, there have only been two studies on impact incidence at the high school level. The first investigation, conducted by Schnebel et al. [13], evaluated 16 high school football players fitted with the HIT System across a single season of games and practices. The investigators reported that 8326 impacts were collected across 15 practice and nine game sessions. This amounted to an estimated average of 22 impacts per session or 520 impacts per athlete per season. Similar figures were reported in a later investigation of high school football athletes [14&]. In that study, 95 athletes were tracked over 4 years and sustained a mean of 652 (median 626) impacts per player over the 14-week season. This would suggest that the average athlete sustained 46 impacts per week or 6.5 impacts to the head every day of the week for 14 weeks. One athlete was reported to have sustained 2235 during the single season or an estimated 22 impacts per day.
Although the overall number of impacts sustained by the average athlete is staggering, there are clear differences in session type and position that influence the impact count. For example, Broglio et al. [15] reported on 35 interscholastic athletes fitted with the HIT System that recorded 19 224 impacts across 55 practices and 13 games. Game sessions expectedly resulted in a higher number of impacts (24.5) than practices (9.2), but there were also differences in playing positions. Specifically, there was only a 4% difference in impact counts between the offensive and defensive line players; but the defensive linemen sustained 69 and 98% more impacts compared with the offensive and defensive skill players, respectively. When player position was analyzed even more closely, the following impacts per session were reported in practices: the offensive and defensive linemen incurred 10.7 impacts per session; quarterbacks incurred 3.1 impacts per session; wide-receivers, cornerback, and safeties incurred 4.5 impacts per session; and the tight-ends, running-backs, and linebackers incurred 7.1 impacts per session. A similar impact profile was observed during games, but the absolute numbers were doubled: linemen incurred 28.7 impacts compared with 25.6 in quarterbacks, 15.7 in wide-receivers, cornerbacks, and safeties, and 24.0 in tight-ends, running-backs, and linebackers [14&].
High school athletes are reported to sustain between 520 and 652 impacts annually, which is more than reported in collegiate athletes, who may sustain between 257 and 438 [16,17] impacts annually. On the basis of the existing literature the reason for these differences between studies remains unclear. More impacts would be expected among the collegiate athletes as they have a longer competitive season. The standard high school season is nine games, whereas the standard collegiate season is 12 games. The style of play and coaching philosophy (i.e. number of contact practices per week) may also influence the number of annual impacts. Regardless, football athletes at both levels sustain a substantial number of impacts to the head, the long-term consequences of which have yet to be fully defined.
In addition to the frequency at which high school athletes are sustaining impacts on the football field, there have also been reports on the magnitude of those impacts. As one might expect, impact magnitudes during games were slightly higher than during practices [15]. Indeed, the mean linear acceleration incurred during games was 24.8 g, compared with 23.3 g during practice sessions. A similar small magnitude difference has also been reported for rotational acceleration, with the game mean at 1669.8 rad/s/s and practices at 1468.6 rad/s/s. Similar data were reported from a larger sample of high school athletes whereby the mean linear and angular acceleration from all sessions was 25.1 g and 1627 rad/s/s, respectively. As expected, higher acceleration values were recorded during game situations (26.1 g and 1711.2 rad/s/s) relative to practices only (24.2 g and 1554.3 rad/s/s) [7]. Similarly to impact counts, player position also influenced impact magnitude. During game sessions the linear accelerations were greatest among the offensive (26.2 g) and defensive skill (25.0 g) players. The offensive (24.5 g) and defensive linemen (24.0 g) [15] had lower reported values, but the difference between the skill players and linemen is likely negligible. The difference in mean values in both of these investigations likely has little to no clinical significance.
Clearly there are distinct differences in game and practice intensities that the casual observer would interpret as more severe impacts. While the mean values reported from the studies above do not support this conclusion, a difference is indeed present. In game situations there is an increased frequency of high-magnitude impacts at all positions [14&]. Yet, these impacts are not frequent enough to have a meaningful change to the mean acceleration values. Indeed, in a dataset of over 100 000 impacts, it would take a substantial number of high-magnitude impacts for there to be a shift in the overall mean.
Although there is little difference between the overall mean accelerations during games and practices, a look at how frequently large-magnitude impacts occur yields interesting findings. In general, impacts occurring in high school football fall on the low end of the spectrum, with 75% of all impacts resulting in a linear head acceleration of 30 g or less [18], which is far below the levels of a concussive impact. Most important when evaluating impact magnitude distribution is how the high school athlete is compared with the collegiate level athlete. Schnebel et al. [13] were the first to show these differences and reported the top 5, 2, and 1% of all impacts sustained by high school athletes were 56.2, 75.1, and 90.6 g. By comparison, collegiate level athletes were incurring post-impact accelerations of 58.8, 80.6, and 99.2 g among the same percentile rankings (5, 5, and 1%). Data reported by Eckner et al. [19&] showed a similar impact intensity as previously reported.
This finding is actually quite remarkable, as for the first time it quantifies the difference in impact intensity between the high school and collegiate athlete. Collegiate athletes clearly sustain a greater number of high-magnitude impacts, which might lead one to speculate that they are at a greater risk for concussion. Yet, large-scale concussion incidence studies do not support this supposition. In fact, concussion incidence is nearly identical between the two groups with an average occurrence of about 5% in both groups [20–22]. Why the collegiate athlete can more frequently sustain large-magnitude impacts without injury remains unclear at this point, but some have speculated that the more elite collegiate athlete may have a higher injury threshold.
Biomechanical threshold for concussion
In large part, the application of biomechanics to concussion has been in an attempt to identify a variable or set of variables and the associated magnitudes that can predict concussion. The clinical intent of this research was two-fold; first, to produce data that could be used by manufacturers in developing new impact-mitigating equipment that would reduce injury risk. Second, with the advent of telemetered-based accelerometers, many initially speculated that impact magnitudes could be used as a diagnostic criterion for injury, or at a minimum used as an alert to a potentially injured athlete. While significant resources have been dedicated to answering this problem, no investigation has clearly delineated a set of variables that could be sufficiently used for concussion diagnosis.
Of the many variables captured by current technology, linear acceleration, angular acceleration, and impact location have been consistently reported in the literature for use in predicting concussions. Some investigations have reported a case by-case evaluation of concussive impacts [13,23,24]. At the high school level a single study evaluated 13 concussions (taken from 535 63 impacts) that occurred when the peak linear accelerations ranged from 74.0 to 146.0 g and angular accelerations from 5582.6 to 9515.6 rad/s/s. Using a classification and regression tree analysis, clinical decision making points were set for rotational acceleration, linear acceleration, and impact location. For example, based on rotational acceleration alone, if the impact exceeded 5582 rad/s/s then there was a 1.9% chance for injury. If the impact also exceeded 96.1 g of linear acceleration then the risk for injury increased to 6.9%. If the impact was also sustained to the front, side, or top of the helmet then the risk for injury rose to 13.4% [7]. While a 13.4% sensitivity to concussion does not meet the criteria for clinical applicability, this analysis improved upon previous suggestions for a concussion threshold. Indeed, Pellman et al. [4] suggested that 98 g was the threshold for concussion, yet when applied to the high school dataset only 3.5% of the concussions would have been detected. Similarly, a principal component analysis calculation employing linear acceleration, rotational acceleration, HIC, and impact location in excess of 63 [6] would have identified 6% of the concussed athletes [7].
It is widely accepted that concussion outcomes differ between adult and youth players [25,26] and the threshold for injury is commonly thought to differ as well [27]. Yet, if the biomechanical data from concussed collegiate athletes are examined closely, it is apparent that the threshold for concussion is similar at both levels. Indeed, HIT System data captured from 13 concussed collegiate athletes indicate 102.8 g is the mean linear acceleration and 5311.6 rad/s/s the mean rotational acceleration [28], compared with 86.3 g and 6111.4 rad/s/s among concussed high school athletes [29].
Noting the differences in impact magnitudes between the collegiate and high school athletes, the similar concussion threshold among the two groups and the similarity in injury rates (approximately 5%) at both levels of play are remarkable. Given the limitations of the literature, however, we can only speculate why collegiate athletes do not sustain concussions at a higher rate than their high school counterparts. Most obviously the collegiate athlete is more talented and in part may have made it to that level because of an ability to withstand high-magnitude impacts without injury. Explained differently, the elite adult athlete may have a higher tolerance to high-magnitude impacts than the typical high school athlete. Where the tolerance is derived from is not clear. Some have speculated that the additional years of cerebral development and myelination offer a neuroprotecive effect [30]. Other factors, such as anatomical differences in the dura, cerebral vascularization, or cranial topography, may all influence injury tolerance, but are not quantifiable at this time. It is also feasible that collegiate athletes are sustaining more concussions, but reporting fewer of them. It is well documented that high school athletes do not report as many as 50% of their concussions to a coach, medical professional, or parent [2]. Collegiate athletes, however, are known to under-report concussive injuries by as much as 80% [31].
Conclusion
In the final assessment it is clear that there are numerous health and social benefits to participating in football and other athletic endeavors. Yet, as with all activities, there is the risk for injury, and concussion is one such injury. Researchers and clinicians have thus sought to better understand concussion biomechanics in an effort both to reduce injuries and to more rapidly identify those with an injury. Despite the notable increase in our knowledge of the injury, significant gaps remain. It is now known that the average athlete will sustain approximately 15 impacts during a game or practice and the average magnitude of those impacts is well below the risk of concussion (approximately 25 g). Fewer than 1% of impacts that occur on the field will place the athlete at risk for concussion, as these injuries appear to be occurring when the head reaches acceleration values of approximately 95 g, 5500 rad/s/s, with the impact occurring to the front, side, and top.
The introduction of the HIT System and similar devices has vastly increased our understanding of concussion biomechanics. Across a number of investigations it is clear that a combination of linear acceleration, rotational acceleration, and impact location all influence the athlete’s injury risk. Despite this consistency, a number of unmeasured variables may also influence injury risk: cerebral blood flow, cerebrospinal fluid volume, or hydration status; central fatigue; systemic factors; and sleep deprivation or intercurrent illness. As such, the telemetered devices designed to record post-impact head accelerations cannot be used as a clinical diagnostic tool, but rather as a method to identify those athletes who have sustained a large magnitude impact and should be removed from play for further evaluation. Ultimately, the concussion diagnosis is a clinical decision that must be made by a trained medical professional.
References
- 1.Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375–378. doi: 10.1097/00001199-200609000-00001. [DOI] [PubMed] [Google Scholar]
- 2.McCrea M, Hammeke T, Olsen G, et al. Unreported concussion in high school football players: implications for prevention. Clin J Sport Med. 2004;14:13–17. doi: 10.1097/00042752-200401000-00003. [DOI] [PubMed] [Google Scholar]
- 3.McCrory P, Meeuwisse W, Johnston K, et al. Consensus Statement on Concussion in Sport 3rd International Conference on Concussion in Sport Held in Zurich, November 2008. Br J Sports Med. 2009;43:i76–i90. doi: 10.1136/bjsm.2009.058248. [DOI] [PubMed] [Google Scholar]
- 4.Pellman EJ, Viano DC, Tucker AM, et al. Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery. 2003;35:799–814. doi: 10.1093/neurosurgery/53.3.799. [DOI] [PubMed] [Google Scholar]
- 5.Ommaya AK, Gennarelli TA. Cerebral concussion and traumatic unconsciousness: correlation of experimental and clinical observations on blunt head injuries. Brain. 1974;97:633–654. doi: 10.1093/brain/97.1.633. [DOI] [PubMed] [Google Scholar]
- 6.Greenwald RM, Gwin JT, Chu JJ, Crisco JJ. Head impact severity measures for evaluating mild traumatic brain injury risk exposure. Neurosurgery. 2008;62:789–798. doi: 10.1227/01.neu.0000318162.67472.ad. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Broglio SP, Schnebel B, Sosnoff JJ, et al. Biomechanical properties of concussions in high school football. Med Sci Sports Exerc. 2010;42:2064–2071. doi: 10.1249/MSS.0b013e3181dd9156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Viano DC, Casson IR, Pellman EJ. Concussion in professional football: biomechanics of the struck player: part 14. Neurosurgery. 2007;61:313–328. doi: 10.1227/01.NEU.0000279969.02685.D0. [DOI] [PubMed] [Google Scholar]
- 9.Viano DC, Pellman EJ. Concussion in professional football: biomechanics of the striking player: part 8. Neurosurgery. 2005;56:266–280. doi: 10.1227/01.neu.0000150035.54230.3c. [DOI] [PubMed] [Google Scholar]
- 10.Hollister NR, Jolley WP, Horne RG. Biophysics of concussion. WADC Technical Rep. 1958:58–193. [Google Scholar]
- 11.Bishop PJ, Norman RW, Kozey JW. An evaluation of football helmets under impact conditions. Am J Sport Med. 1984;12:233–236. doi: 10.1177/036354658401200313. [DOI] [PubMed] [Google Scholar]
- 12.Gadd CW. Use of weighted-impulse criterion for estimating injury hazard [abstract] Stapp Car Crash J. 1966;29:249–254. [Google Scholar]
- 13.Schnebel B, Gwin JT, Anderson S, Gatlin R. In vivo study of head impacts in football: a comparison of National Collegiate Athletic Association Division I versus high school impacts. Neurosurgery. 2007;60:490–495. doi: 10.1227/01.NEU.0000249286.92255.7F. [DOI] [PubMed] [Google Scholar]
- 14.Broglio SP, Eckner JT, Martini D, et al. Cumulative head impact burden in high school football. J Neurotrauma. 2011;28:2069–2078. doi: 10.1089/neu.2011.1825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Broglio SP, Sosnoff JJ, Shin S, et al. Head impacts during high school football: a biomechanical assessment. J Athl Train. 2009;44:342–349. doi: 10.4085/1062-6050-44.4.342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Crisco JJ, Fiore R, Beckwith JG, et al. Frequency and location of head impact exposures in individual collegiate football players. J Athl Train. 2010;45:549–559. doi: 10.4085/1062-6050-45.6.549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Crisco JJ, Wilcox BJ, Beckwith JG, et al. Head impact exposure in collegiate football players. J Biomech. 2011;44:2673–2678. doi: 10.1016/j.jbiomech.2011.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Broglio SP, Surma T, Ashton-Miller JA. High school and collegiate football athlete concussions: a biomechanical review. Ann Biomed Eng. 2012;40:37–46. doi: 10.1007/s10439-011-0396-0. [DOI] [PubMed] [Google Scholar]
- 19.Eckner JT, Sabin MN, Kutcher JS, Broglio SP. No evidence for a cumulative impact effect on concussion injury threshold. J Neurotrauma. 2011;28:2079–2090. doi: 10.1089/neu.2011.1910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Powell JW, Barber-Foss KD. Traumatic brain injury in high school athletes. JAMA. 1999;282:958–963. doi: 10.1001/jama.282.10.958. [DOI] [PubMed] [Google Scholar]
- 21.Guskiewicz KM, McCrea M, Marshall SW, et al. Cumulative effects associated with recurrent concussion in collegiate football players: the NCAA concussion study. JAMA. 2003;290:2549–2555. doi: 10.1001/jama.290.19.2549. [DOI] [PubMed] [Google Scholar]
- 22.Guskiewicz K, Weaver NL, Padua DA, Garrett WE. Epidemiology of concussion in collegiate and high school football players. Am J Sports Med. 2000;28:643–650. doi: 10.1177/03635465000280050401. [DOI] [PubMed] [Google Scholar]
- 23.Brolinson PG, Manoogian S, McNeely D, et al. Analysis of linear head accelerations from collegiate football impacts. Curr Sports Med Rep. 2006;5:23–28. doi: 10.1097/01.csmr.0000306515.87053.fa. [DOI] [PubMed] [Google Scholar]
- 24.Duma SM, Manoogian SJ, Bussone WR, et al. Analysis of real-time head accelerations in collegiate football players. Clin J Sport Med. 2005;15:3–8. doi: 10.1097/00042752-200501000-00002. [DOI] [PubMed] [Google Scholar]
- 25.Field M, Collins MW, Lovell MR, Maroon JC. Does age play a role in recovery from sports-related concussion? A comparison of high school and collegiate athletes. J Pediatr. 2003;142:546–553. doi: 10.1067/mpd.2003.190. [DOI] [PubMed] [Google Scholar]
- 26.Baillargeon A, Lassonde M, Leclerc S, Ellemberg D. Neuropsychological and neurophysiological assessment of sport concussion in children, adolescents and adults. Brain Inj. 2012;26:211–220. doi: 10.3109/02699052.2012.654590. [DOI] [PubMed] [Google Scholar]
- 27.McKeever CK, Schatz P. Current issues in the identification, assessment, and management of concussions in sports-related injuries. Appl Neuropsychol. 2003;10:4–11. doi: 10.1207/S15324826AN1001_2. [DOI] [PubMed] [Google Scholar]
- 28.Guskiewicz KM, Mihalik JP, Shankar V, et al. Measurement of head impacts in collegiate football players: relationship between head impact biomechanics and acute clinical outcome after concussion. Neurosurgery. 2007;61:1244–1252. doi: 10.1227/01.neu.0000306103.68635.1a. [DOI] [PubMed] [Google Scholar]
- 29.Broglio SP, Eckner JT, Surma T, Kutcher JS. Postconcussion cognitive declines and symptomatology are not related to concussion biomechanics in high school football players. J Neurotrauma. 2011;28:2061–2068. doi: 10.1089/neu.2011.1905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Giedd JN, Blumenthal J, Jefferies NO, et al. Brain development during childhood and adolescence: a longitudinalMRI study. Nat Neurosci. 1999;2:861–863. doi: 10.1038/13158. [DOI] [PubMed] [Google Scholar]
- 31.Sefton JM, Pirog K, Capitao A, et al. An examination of factors that influence knowledge and reporting of mild brain injuries in collegiate football [abstract] J Athl Train. 2004;39:S52–S53. [Google Scholar]