

Abstract
Objective
This study used prospective, observational methods to evaluate six features of therapist behavior as predictors of homework adherence in cognitive-behavioral therapy (CBT) for adolescent depression, with the goal of identifying therapist strategies with the potential to improve adolescent adherence. Therapist behaviors were expected to interact with initial levels of client resistance or adherence to predict subsequent homework completion.
Method
Participants were 50 referred adolescents (33 females, 54% ethnic minority) ages 14–18 (M=15.9) meeting diagnostic criteria for a depressive disorder, and without co-morbid psychotic disorder, bipolar disorder, autism spectrum disorder, intellectual disability, or concurrent treatments. Therapist homework-related behaviors were coded from audiotapes of Sessions 1 and 2 and used to predict adolescents’ homework adherence, coded from audiotapes of Sessions 2 and 3.
Results
Several therapist behaviors were predictive of subsequent homework adherence, particularly for initially resistant or non-adherent adolescents. Stronger homework rationale and greater time allocated to explaining homework in Session 1 predicted greater adherence at Session 2, particularly for initially resistant adolescents. Stronger rationale and eliciting reactions/troubleshooting obstacles in Session 2 predicted greater adherence at Session 3, particularly for adolescents who were less adherent to prior homework.
Conclusions
Strategies such as providing a strong rationale, allocating more time to assigning homework, and eliciting reactions/troubleshooting obstacles may be effective ways to bolster homework adherence among initially less engaged, depressed teens.
Keywords: Adolescent depression, CBT, homework adherence, engagement, therapist behavior
The assignment of homework is considered important in Cognitive-Behavioral Therapy (CBT) as a means to build and generalize new client skills. A growing body of evidence supports homework as an active ingredient in CBT for adults (see Kazantzis et al., 2010, for a meta-analysis). Although only a handful of empirical studies have examined the role of homework in youth treatments (Clarke et al., 1992; Gaynor, Lawrence & Nelson-Gray, 2006; Hughes and Kendall, 2007; Kazdin, Bass, Siegel, & Thomas, 1989), there is some evidence supporting its positive association with outcome. Two studies of homework in CBT for adolescent depression yielded small to moderate correlations between homework adherence and outcome (Clark et al., 1992; Gaynor et al., 2006). In both studies, adolescents completed about half of assigned homework tasks. Initial results, then, suggest homework completion contributes to better depression outcomes, but adolescent adherence is far from optimal. Thus, one way to improve CBT for adolescent depression could be through increased homework adherence.
A small number of studies in the adult treatment literature have examined therapist behaviors thought to be associated with increased homework adherence. These empirical studies have largely focused on four cognitive therapy strategies originally prescribed by Beck, Rush, Shaw, and Emery (1979), which include: 1) providing clear and specific task instructions and custom-tailoring homework tasks to client problems when possible; 2) providing a rationale for the assignment, stressing the importance and the goals of the task; 3) eliciting patient reactions and possible obstacles to completion of the homework, troubleshooting when necessary; and 4) reviewing assignments from the previous session, summarizing progress made or conclusions drawn from the exercise. Each of these strategies has received some empirical support with adults (Bryant, Simons & Thase, 1999; Detweiler-Bedell & Whisman, 2005; Ryum, Stiles, Svartberg, & McCullough, 2010; Shaw et al., 1999).
Despite suboptimal homework adherence among teens, little is known about processes that improve adherence in youth. Beck and colleagues’ (1979) prescribed strategies provide a framework for examining therapist homework-related behavior with adolescents. From a developmental perspective, the strategy of eliciting adolescent reactions and perceived obstacles to homework completion seems particularly important given that a collaborative approach has been shown to facilitate alliance development with adolescents (Diamond, Liddle, Hogue, & Dakof, 1999), who can be reactive to adult prescriptions or requests.
Of course, “adherence-enhancing behaviors” do not occur in a vacuum. Adolescents vary significantly in their readiness to engage in treatment, and prior research has found that adolescents with higher levels of initial resistance showed poorer subsequent involvement in treatment tasks (Jungbluth & Shirk, 2009). Similarly, early homework adherence has been found to predict subsequent adherence (Addis & Jacobson, 2000). Thus, adolescents who have shown high initial resistance or poor adherence to a previous homework task are likely at greater risk for future non-adherence. It is hypothesized that initially resistant or non-adherent adolescents might benefit most from additional therapist use of adherence-enhancing strategies. Specifically, greater therapist attention to specifying homework tasks, providing a strong rationale, and troubleshooting obstacles, as well as the sheer amount of time devoted to assigning tasks, may be especially relevant for adolescents who are initially resistant or non-adherent to previous assignments. These same therapist behaviors may not be as critical for adolescents with good early engagement or strong prior homework adherence. Teens who have been adherent to prior homework tasks may benefit more from different therapist behaviors, such as more extensive homework review and therapist use of praise.
In summary, this study evaluated six features of therapist behavior as predictors of homework adherence in CBT for adolescent depression. Session recordings from a study of individually delivered, manual-guided CBT for adolescent depression were utilized. Therapist behaviors were expected to interact with initial levels of client resistance and adherence to predict subsequent homework completion. Coding and analysis of therapist adherence-enhancing behaviors were limited to the first two sessions of treatment for two reasons: 1) Previous research with adults has linked early homework to treatment gains (Addis & Jacobson, 2000; Fennell & Teasdale, 1987) and later homework adherence (Addis & Jacobson, 2000); 2) Sample size constrained our ability to evaluate complex interactions in later sessions (when therapist behavior may interact with or depend upon factors from all prior sessions, such as the cumulative effects of resistance, prior therapist behavior, and the trajectory of homework adherence).
Method
Participants
The data were obtained from an open clinical trial of CBT for depressed adolescents in an urban setting in the Rocky Mountain West (see Shirk, Kaplinski & Gudmundsen, 2009, for a detailed description of study procedures, which were IRB approved prior to initiating the study). Current study participants were 50 referred adolescents (33 females), between ages 14 and 18 (M = 15.9), who met diagnostic criteria for Major Depressive Disorder (n=37), Dysthymic Disorder (n=10), or Depressive Disorder, Not Otherwise Specified (n=3), as assessed with the Computerized Diagnostic Interview Scale for Children (C-DISC; Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000). Exclusionary criteria were: diagnoses of co-morbid Psychotic Disorder, Bipolar Disorder, Autism Spectrum Disorder, or Intellectual Disability; concurrent therapy; or medication for depressive symptoms.
Sixty-six percent of the sample met criteria for a comorbid disorder including generalized anxiety disorder (42%), conduct disorder (34%), social phobia (22%), and attention deficit/hyperactivity disorder (12%). Twenty-eight percent of the treatment sample met criteria for three or more disorders. Forty percent reported a lifetime history of attempted suicide.
By self-report, 54 percent of the sample identified as ethnic minority, including 11 African American/Black, 11 Hispanic/Latino, two Native American, two Biracial, and two Other, with some adolescents endorsing multiple categories. Socioeconomic status was indexed by parent occupation on the Hollingshead Index (Hollingshead, 1976), with an average score of 4.1 (SD=2.1), corresponding to skilled manual workers, craftsmen, and small business owners. Fifty adolescents started treatment, with two dropping out before the second session and five more before Session 3. Available sample size varied across primary analyses from 41 to 33 due to client dropout, mechanical audiotape failure, therapist failure to record a session, and, in a small number of cases, insufficient detail on the audiotape for coding of homework adherence, as discussed in greater detail below. Demographic or study variables did not differ across groups with or without missing data.
Procedure
High school site coordinators identified and referred potential participants for inclusion in the study. Participants completed a computer-administered diagnostic interview (C-DISC) and demographic questionnaires at the pre-treatment interview. Participating adolescents received free treatment and monetary compensation for completion of research interviews.
Treatment
A twelve-session, manual-guided, outpatient cognitive-behavioral treatment, adapted for adolescents and evaluated by Rossello and Bernal (1999), was delivered by eight therapists. Goals of the first session were to build rapport, gather information, provide rationale and expectations for treatment, provide education about depression, and introduce mood monitoring homework. The second session included education about negative thinking and its link to mood, followed by introduction of a thought monitoring homework task. In session three, therapists continued discussing negative thinking in relation to depressed mood and introduced skills for challenging negative thoughts, which were then assigned as homework. A review of 25 percent of audiotapes selected randomly indicated high therapist fidelity to the treatment manual, with 83 percent of components delivered (Shirk, Gudmundsen, Crisp Kaplinski, & McMakin, 2008).
Therapists
All eight therapists had doctoral degrees in clinical psychology, attended a daylong workshop, conducted a supervised practice case, and then received 1.5 hours of weekly group supervision by a licensed psychologist with extensive CBT experience.
Homework
Weekly homework assignments were described in the manual, and time was allocated in every session for assigning new homework and reviewing the previous session’s homework. Teens also received workbooks and handouts on which to record assignments. Session 1 homework required adolescents to record daily mood ratings and triggers for negative arousal. Session 2 was the same, but included recording automatic thoughts associated with negative mood or events. Specific guidelines for how to assign homework were not included in the manual.
Measures
Computerized Diagnostic Interview Scale for Children 4.0 (C-DISC)
The C-DISC (Shaffer et al., 2000) is a highly structured diagnostic interview with good reliability and criterion validity for identifying psychiatric disorders among youth (Shaffer et al., 2000). The mood, anxiety, and disruptive behavior modules were computer administered to screen for inclusion and exclusion disorders and to measure depression severity based on total symptoms endorsed.
Homework Adherence
Homework adherence was coded from audiotapes of Sessions 2 and 3, in random order, on a seven-point scale (0=“no effort” to 6=“did more than was asked or exceptional effort”). Reliability of homework adherence coding, based on double coding of 30 percent of sessions (n = 25), was good, with a two-way random effects intraclass correlation (ICC) of .72. Of the 91 existing sessions we set out to code, 84 were given homework adherence ratings. The remaining seven sessions (7.7 percent) could not be coded for one of several reasons: 1) mechanical audiotape error, 2) therapist forgot to record the session, or 3) there was insufficient information on the audiotape to determine a rating. Observed adherence ratings ranged from 0 to 6 (Session 2 M=4.51, SD=1.01 and Session 3 M=4.21, SD=1.12 after outlier adjustment).
Adherence-Enhancing Behaviors
Behaviors thought to promote homework adherence were measured using the Therapist Homework Adherence Behavior Scale (THABS), an adaptation of Bryant and colleagues’ (1999) measure from CT for depressed adults. The scale includes six items: 1) specification of the task, 2) provision of rationale, 3) elicitation of client reactions and troubleshooting of difficulties, 4) review of previous homework assignment, 5) praise for homework adherence, and 6) total time spent assigning the task. The first five items were rated on a scale from zero (not done) to four (very well done) and anchored to enhance reliability. The sixth item was scored as simply the number of seconds devoted to assigning homework. Two-way random effects intraclass correlations (ICCs), based on double coding of 21 percent of available sessions (n = 19), ranged from .27 to .84 (mean ICC = .67; See Table 1 for item descriptions, ICCs, and descriptive data). Item 4 (review of previous homework assignment) was dropped due to low reliability. Four Session 1 tapes could not be coded because of mechanical tape failure (n = 2) and therapists forgetting to tape the session (n = 2). One Session 2 tape could not be coded because a therapist forgot to tape the session.
Table 1.
Adherence-Enhancing Behaviors: Item Descriptions, ICCs and Descriptive Data
| Item | Description | ICC | M(SD) | Observed Range | Sessions Coded |
|---|---|---|---|---|---|
| Specifying Task | Therapist was clear and specific in giving the assignment. Clear expectations were set for what, how, when how often, etc. | .84 | 3.21(.90) | 0–4 | 1, 2 |
| Providing Rationale | Therapist stressed not only the importance of the assignment, but also the goals it aims to accomplish | .81 | 3.18(.83) | 0–4 | 1, 2 |
| Eliciting/Troubleshooting | Therapist elicited reactions to the assignment to get feedback and help foresee and problem-solve possible obstacles or difficulties that might arise when trying to do the assignment | .82 | 2.03(1.57) | 0–4 | 1, 2 |
| Time Spent Assigning | Number of seconds therapist devoted to assigning the task | .73 | 150(70) | 33–502 | 1, 2 |
| Depth of Review | Therapist reviewed the homework assigned in the preceding session and summarized progress made and conclusions drawn from the exercise | .27 | 3.26(.59) | 2–4 | 2 |
| Praising Adherence | Therapist praised any efforts the client made to do the assigned homework. (Not coded if teen did not make any efforts) | .56 | 2.00(1.68) | 0–4 | 2 |
Initial Resistance
Initial resistance was assessed during Session 1 using six items adapted from the observational Vanderbilt Negative Indicators Scale (Suh, Strupp, & O’Malley, 1986). Observers used audiotapes to code a 15-minute segment for each client, beginning five minutes into Session 1. This early segment was chosen to begin after introductions and initial scheduling concerns were addressed but before the therapist had time to build much rapport, to better capture the client’s contribution to process. Client demeanor was rated using five items covering five dimensions: hostile, frustrated, impatient, intellectualizing, and defensive. A sixth item was used to rate client negative reactions to the therapist. All items were rated on a 5-point scale ranging from 1 (not at all) to 5 (a great deal) and totaled. Internal consistency for the scale was good (Cronbach’s alpha = .89) and a one-way mixed random ICC (using 25% of scores) demonstrated strong inter-rater reliability (ICC = .88). Four Session 1 tapes could not be coded for initial resistance, for reasons listed above. Initial resistance, adherence-enhancing behaviors, and homework adherence were coded by separate sets of coders to avoid bias. Scores ranged from 6 to 25 (M=7.54, SD=1.91, after outlier adjustment).
Results
Outliers were identified for three of the Session 1 THABS items (specifying task: 3 outliers; providing rationale: 5 outliers; time spent assigning: 2 outliers), and both homework adherence variables (Session 2 adherence: 5 outliers; Session 3 adherence: 6 outliers). Outliers were adjusted by bringing them in to 1.5 times the interquartile range beyond the first or third quartile to prevent undue influence. Skew and kurtosis were within acceptable ranges for all variables. Examination of Mahalanobis distance for all interaction model variables revealed no multivariate outliers.
Client characteristics
We tested client demographic (age, gender, race/ethnicity) and clinical (initial depression severity) variables as predictors of homework adherence at Sessions 2 and 3. The only predictor was Hispanic/Latino ethnicity (Spearman r = −.31, p = .03), such that adolescents who self-identified as Hispanic/Latino were less adherent for the first homework task. Thus, Hispanic/Latino was included as a control variable in all analyses predicting homework adherence.
Initial resistance
As expected, initial resistance showed a small, though non-significant, association with homework adherence at Session 2 (r = −.26, p = .09) and Session 3 (r = −.23, p = .18). Initial resistance was included as a predictor or moderator in all analyses of therapist behaviors in relation to homework adherence.
Therapist effects
Analyses were conducted to evaluate the possible influence of therapist effects on homework adherence. Two separate univariate Analysis of Variance (ANOVA) models were run with therapists as the independent grouping factor and Session 2 and Session 3 homework adherence ratings as dependent variables. Results showed no significant therapist effects on these variables (p’s > .4).
Correlations among HWA predictors
Pearson correlation coefficients were calculated to examine the association among the six therapist behaviors, as well as the three other predictor variables (initial resistance, Session 2 homework adherence, and Hispanic/Latino ethnicity) to be evaluated as predictors of HWA. These associations are presented in Table 2. Although several of the therapist behaviors were significantly correlated with one another, no correlation exceeded .52 and most associations were very small and non-significant; thus, the coding system appears to have captured relatively discrete, non-overlapping constructs. Also, therapist behaviors were generally not associated with initial resistance or homework adherence at Session 2, and initial resistance and homework adherence at Session 2 were only associated with one another at a trend level. Hispanic/Latino ethnicity was associated greater therapist provision of rationale at Session 2 (r = .29, p < .05).
Table 2.
Correlations Among Session 1 and 2 Predictors of Homework Adherence
| Time point | Measure | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Session 1 | 1. Initial resistance | |||||||||||
| 2. Specifying Task | .24 | |||||||||||
| 3. Providing Rationale | −.04 | .04 | ||||||||||
| 4. Eliciting/Troubleshooting | .22 | .05 | .24 | |||||||||
| 5. Time Spent Assigning | .14 | .42** | .52** | .11 | ||||||||
| Session 2 | 6. Specifying Task | .04 | .06 | .12 | −.08 | .27† | ||||||
| 7. Providing Rationale | .13 | .13 | .03 | .00 | −.15 | .12 | ||||||
| 8. Eliciting/Troubleshooting | .07 | .00 | −.07 | .40** | −.01 | .08 | .11 | |||||
| 9. Praising Adherence | −.19 | −.05 | .03 | .49** | −.13 | −.15 | −.07 | .21 | ||||
| 10. Time Spent Assigning | .17 | .05 | .04 | .05 | .15 | .42** | .38** | .42** | −.33* | |||
| 11. Session 2 Homework Adherence | −.26† | .06 | .25 | −.04 | .38* | .05 | −.34* | −.10 | .14 | .03 | ||
| Pre-Treatment | 12. Hispanic/Latino Ethnicitya | −.13 | .08 | −.17 | .15 | −.24 | .09 | .29* | .15 | .13 | .08 | −.31* |
p < .10.
p < .05.
p < .01.
Spearman correlations are reported for this dichotomous variable.
Session 1 therapist behaviors predicting homework adherence in Session 2
Each of the four Session 1 therapist behaviors were entered into separate multiple regressions. In each regression, therapist behavior was entered along with initial resistance, Hispanic/Latino ethnicity, and the interaction term (therapist behavior centered x initial resistance centered) as predictors of homework adherence at Session 2. Results of these regressions are described below and in Table 3.
Table 3.
Multiple Regression Analyses Predicting Homework Adherence at Session 2 from Therapist Adherence-Enhancing Behaviors in Session 1
| Regression | Predictor | B (SE) | Standardized Beta (β) | Model R2 |
|---|---|---|---|---|
| 1 | Hispanic/Latino | −1.05(.35) | −.44** | .270* |
| Specifying task | .083(.17) | .08 | ||
| Initial resistance | −.11(.09) | −.23 | ||
| Specifying task x initial resistance | −.13(.11) | −.21 | ||
|
| ||||
| 2 | Hispanic/Latino | −.83(.33) | −.35* | .363** |
| Providing rationale | .18(.17) | .15 | ||
| Initial resistance | −.13(.06) | −.27† | ||
| Providing rationale x initial resistance | .15(.07) | .31* | ||
|
| ||||
| 3 | Hispanic/Latino | −.98(.35) | −.41** | .255* |
| Eliciting reactions/troubleshooting | .09(.09) | .15 | ||
| Initial resistance | −.17(.07) | −.37* | ||
| Eliciting/troubleshooting x initial resistance | .03(.05) | .10 | ||
|
| ||||
| 4 | Hispanic/Latino | −.80(.32) | −.33* | .425** |
| Number of seconds spent assigning | .004(.002) | .26† | ||
| Initial resistance | −.19(.06) | −.40** | ||
| Number of seconds x initial resistance | .001(.001) | .30* | ||
p < .10.
p < .05.
p < .01.
Initial resistance demonstrated a small to medium effect across regressions (β’s from −.23 to −.40), as did Hispanic/Latino ethnicity (β’s from −.33 to −.44). In addition, interaction effects were observed for two therapist behaviors: As illustrated in Figure 1, and consistent with our hypothesis, provision of rationale in Session 1 predicted Session 2 adherence more strongly for adolescents who were initially more resistant (interaction term β = .31, p = .03). As illustrated in Figure 2, and also consistent with our hypothesis, the positive predictive association between time spent assigning in Session 1 and adherence in Session 2 appeared stronger for adolescents who were initially more resistant (interaction term β = .30, p = .03). (In Figures 1 and 2, initial resistance was dichotomized at the median into high and low groups for the purposes of illustration.) There was also a trend-level main effect for time spent assigning the homework (β = .26, p = .07) predicting Session 2 adherence.
Figure 1.
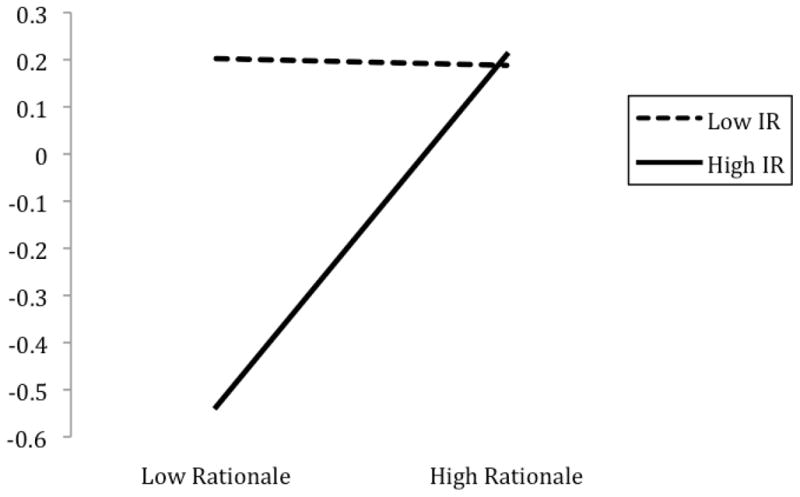
The interaction between initial resistance (IR) and provision of rationale in Session 1 to predict homework adherence at Session 2, controlling for Hispanic/Latino ethnicity.
Figure 2.
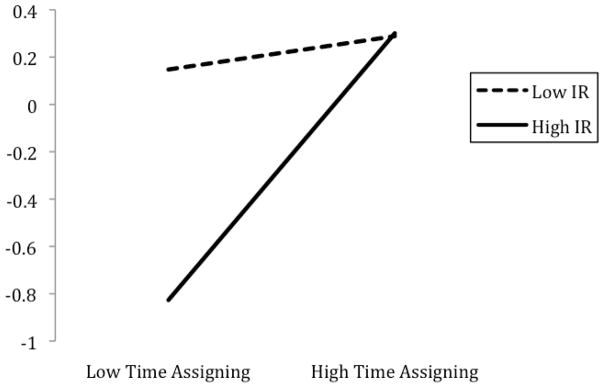
The interaction between initial resistance (IR) and the amount of time therapist spent assigning homework in Session 1 to predict homework adherence at Session 2, controlling for Hispanic/Latino ethnicity.
Session 2 therapist behaviors predicting clients’ homework adherence at Session 3, considering prior adherence
Next, we examined whether the same four adherence-enhancing behaviors, this time measured in Session 2, would interact with clients’ level of prior homework adherence to predict adherence at Session 3. Each of the four therapist behaviors were entered into separate multiple regressions along with Session 2 homework adherence, initial resistance, Hispanic/Latino ethnicity, and the interaction term (therapist behavior centered x Session 2 homework adherence centered). The dependent variable was homework adherence at Session 3. Results of these multiple regressions are described below and displayed in Table 4.
Table 4.
Multiple Regression Analyses Predicting Homework Adherence at Session 3 from Therapist Adherence-Enhancing Behaviors in Session 2
| Regression | Predictor | B(SE) | Standardized Beta (β) | Model R2 |
|---|---|---|---|---|
| 1 | Hispanic/Latino | .16(.56) | .06 | .264 |
| Specifying task | .19(.28) | .12 | ||
| Session 2 Homework Adherence | .38(.22) | .34 | ||
| Initial resistance | −.14(.10) | −.25 | ||
| Specifying task x Session 2 Homework Adherence | −.23(.34) | −.13 | ||
|
| ||||
| 2 | Hispanic/Latino | −.04(.51) | −.01 | .399* |
| Providing rationale | .05(.11) | .07 | ||
| Session 2 Homework Adherence | .48(.20) | .43* | ||
| Initial resistance | −.26(.10) | −.45* | ||
|
| ||||
| Providing rationale x Session 2 Homework Adherence | −.35(.13) | −.45* | ||
| 3 | Hispanic/Latino | −.26(.57) | −.09 | .372* |
| Eliciting reactions/troubleshooting | −.06(.13) | −.07 | ||
| Session 2 Homework Adherence | .48(.21) | .42* | ||
| Initial resistance | −.17(.09) | −.29† | ||
| Eliciting/troubleshooting x Session 2 Homework Adherence | −.31(.13) | −.40* | ||
|
| ||||
| 4 | Hispanic/Latino | .11(.56) | .04 | .269 |
| Number of seconds spent assigning | −.002(.002) | −.13 | ||
| Session 2 Homework Adherence | .43(.25) | .38† | ||
| Initial resistance | −.12(.10) | −.20 | ||
| Number of seconds x Session 2 Homework Adherence | −.002(.003) | −.12 | ||
|
| ||||
| 5 | Hispanic/Latino | −.40(.68) | −.10 | .443** |
| Praise for adherence | −.18(.13) | −.27 | ||
| Session 2 Homework Adherence | 1.14(.33) | .62** | ||
| Initial resistance | −.27(.09) | −.47** | ||
p < .10.
p < .05.
p < .01.
Initial resistance demonstrated a small to medium effect across regressions (β’s from −.20 to −.47), and Session 2 homework adherence demonstrated a medium effect across regressions (β’s from .34 to .43) predicting Session 3 adherence. In addition, interaction effects were observed for two of the therapist behaviors: Consistent with our prediction, and as illustrated in Figure 3, provision of rationale in Session 2 predicted homework adherence at Session 3 most strongly for those adolescents who had shown poorer adherence to the previous homework task (interaction term β = −.45, p = .01). Also consistent with our prediction, and as illustrated in Figure 4, eliciting client reactions and troubleshooting obstacles to adherence in Session 2 was positively associated with homework adherence in Session 3 for adolescents who had shown poorer prior adherence (interaction term β = −.40, p = .026). (In Figures 3 and 4, Session 2 homework adherence was dichotomized into high and low groups for the purposes of illustration. High adherence reflected scores of “5” or higher, and low adherence reflected scores lower than “5” on the homework adherence scale.)
Figure 3.

The interaction between Session 2 homework adherence (HW2) and Session 2 providing rationale to predict homework adherence at Session 3, controlling for level of initial resistance and Hispanic/Latino ethnicity.
Figure 4.
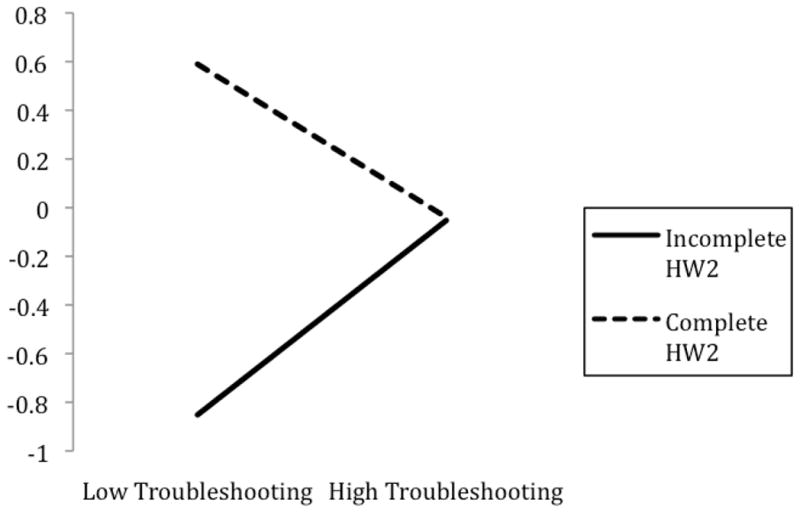
The interaction between Session 2 homework adherence (HW2) and Session 2 eliciting reactions/troubleshooting obstacles to predict homework adherence at Session 3, controlling for level of initial resistance and Hispanic/Latino ethnicity.
Contingent praise in Session 2 was also examined as a predictor of Session 3 homework adherence using multiple regression. Of 33 participants with complete data for this analysis, 28 had completed at least some of the first homework assignment and were included. Praise, Session 2 homework adherence, initial resistance and Hispanic/Latino ethnicity were entered as predictors of Session 3 homework adherence. Results showed significant main effects for Session 2 homework adherence (β = .62, p = .002) and initial resistance (β = −.48, p = .008). The praise term was not significant (p = .18).
Discussion
The current study used prospective, observational methods to examine six therapist behaviors thought to bolster adolescents’ adherence to homework tasks. Consistent with the adult literature, homework adherence was not merely a function of client characteristics, but instead was associated with variations in the way therapists assigned and reviewed homework tasks. Importantly, the positive impact of several therapist behaviors on early homework adherence was conditioned by client behaviors, including early resistance and prior adherence, underscoring the interactive nature of therapy processes.
It was hypothesized that four therapist behaviors—specifying the task, providing rationale, eliciting reactions/troubleshooting obstacles, and amount of time spent assigning—would predict subsequent adherence, with the greatest effects for adolescents who were at risk for poor homework adherence. Adolescents were determined to be at risk for poor adherence if they demonstrated higher levels of initial resistance in Session 1 and if they demonstrated poor adherence on the first homework task, due in Session 2. Consistent with predictions, three therapist behaviors interacted with the risk variables to predict subsequent adherence.
First, adolescents with higher levels of initial resistance and lower levels of initial adherence were more likely to adhere to subsequent homework assignments when therapists provided a strong rationale. This association was not observed with less resistant and initially more adherent adolescents. Greater provision of rationale did not predict adherence with adults (Bryant et al. 1999), but only main effects were examined. Alternatively, provision of a clear rationale may be particularly important for adolescents compared to adults.
Second, the amount of time therapists devoted to assigning homework in Session 1 predicted adherence in Session 2 at a trend level, and this effect was stronger for adolescents who were initially more resistant. This finding suggests therapists may be able to promote greater adherence by setting aside more time in sessions for assigning tasks, especially for relatively disengaged teens. Associations among therapist behavior variables suggest therapists who spent more time assigning homework were also doing a better job specifying the task and providing rationale for it. Time spent in Session 2 did not predict subsequent adherence, perhaps owing to similarity of homework assignments across early sessions.
Third, when adolescents did not show strong adherence to the first homework assignment, therapist efforts to elicit reactions and troubleshoot obstacles in the second session predicted better adherence to the next assignment. This finding converges with three studies with adults indicating positive effects for eliciting reactions and troubleshooting (Bryant et al., 1999, Detweiler-Bedell & Whisman, 2005, & Worthington, 1986). The same therapist behavior, when measured in the first session, did not predict adherence in Session 2, even when initial resistance was considered as a moderator. It may have been easier to identify and address obstacles after they occurred than before.
Another behavior, specifying the homework task, did not predict subsequent adherence in either session, which may reflect that worksheets with clear written instructions were provided. Providing written reminders has been linked to improved medical adherence (Cox, Tisdelle & Culbert, 1988, Stone et al., 2002) and better therapy outcomes for depressed adults (Detweiler-Bedell & Whisman, 2005).
In examining these four therapist behaviors, consideration of context variables (initial resistance and prior adherence) was essential. Contrary to expectations, only one of the four therapist behaviors trended toward a main effect on subsequent adherence. The remaining predictive effects were only significant when considering these moderators, and results begin to address the clinically important question of how to improve low adherence.
There was also an association between Hispanic/Latino ethnicity and adherence to the first homework task; however, this finding is viewed with caution, as Hispanic/Latino ethnicity was not associated with adherence to the second homework task or initial resistance, nor did it predict alliance or outcome in a previous study with the current sample (Shirk, Gudmundsen, Crisp Kaplinski, & McMakin, 2008).
This study had a number of limitations. First, though larger than most prior studies in this literature, sample size was limited. Given power limitations (power for medium effects ranged between .5 and .7) and the exploratory nature of the study, we made no alpha adjustment for the number of analyses conducted; with Bonferroni correction for the main analyses, adjusted alpha would have been .004. Consequently, replication is essential. Second, identified associations were correlational. Future studies should experimentally manipulate therapist behaviors to clarify causality. Third, therapist behaviors were not examined beyond the second session of treatment; thus, current findings may not generalize to middle and later phases of therapy when assignments often become more demanding. Fourth, although standardized homework assignments in the current protocol offered methodological advantages (e.g., variability in adherence across adolescents could not be attributed to variation in homework tasks), this prevented examination of some therapist strategies (e.g., collaborative task generation, individual tailoring) and may have constrained effect sizes for others (e.g., task specification). Similarly, the manual’s specification of homework review likely constrained variation in this behavior. Finally, interrater reliability for therapist praise was suboptimal.
Clinically, therapists faced with depressed adolescents who initially show poor engagement or marginal homework adherence may consider spending more time assigning homework and providing a strong rationale linking homework tasks to recovery. In addition, therapists may be able to improve poor initial adherence by taking time to troubleshoot obstacles that arise. In sum, how therapists address homework relates to how much homework depressed adolescents will do.
Contributor Information
Nathaniel J. Jungbluth, Email: Nathaniel.Jungbluth@SeattleChildrens.org, nathaniel_jungbluth@yahoo.com, Department of Psychiatry and Behavioral Medicine, Seattle Children’s Hospital, Seattle, WA
Stephen R. Shirk, Email: sshirk@psy.du.edu, Department of Psychology, University of Denver, Denver, CO
References
- Addis M, Jacobson N. A closer look at the treatment rationale and homework compliance in cognitive-behavioral therapy for depression. Cognitive Therapy and Research. 2000;24:313–326. doi: 10.1023/A:1005563304265. [DOI] [Google Scholar]
- Beck A, Rush A, Shaw B, Emery G. Cognitive therapy of depression. New York, NY: Guilford; 1979. [Google Scholar]
- Bryant M, Simons A, Thase M. Therapist skill and patient variables in homework compliance: Controlling an uncontrolled variable in cognitive therapy outcome research. Cognitive Therapy and Research. 1999;23:381–399. doi: 10.1023/A:1018703901116. [DOI] [Google Scholar]
- Clarke G, Hops H, Lewinsohn P, Andrews J, Seeley J, Williams J. Cognitive-behavioral group treatment of adolescent depression: Prediction of outcome. Behavior Therapy. 1992;23:341–354. doi: 10.1016/S0005-7894(05)80162-5. [DOI] [Google Scholar]
- Cox D, Tisdelle D, Culbert J. Increasing adherence to behavioral homework assignments. Journal of Behavioral Medicine. 1988;11:519–522. doi: 10.1007/BF00844844. [DOI] [PubMed] [Google Scholar]
- Detweiler-Bedell J, Whisman M. A lesson in assigning homework: Therapist, client, and task characteristics in cognitive therapy for depression. Professional Psychology: Research and Practice. 2005;36:219–223. doi: 10.1037/0735-7028.36.2.219. [DOI] [Google Scholar]
- Diamond G, Liddle H, Hogue A, Dakof G. Alliance-building interventions with adolescents in family therapy: A process study. Psychotherapy: Theory, Research, Practice, Training. 1999;36:355–368. doi: 10.1037/h0087729. [DOI] [Google Scholar]
- Fennell M, Teasdale J. Cognitive therapy for depression: Individual differences and the process of change. Cognitive Therapy and Research. 1987;11:253–271. doi: 10.1007/BF01183269. [DOI] [Google Scholar]
- Gaynor S, Lawrence P, Nelson-Gray R. Measuring homework compliance in cognitive-behavioral therapy for adolescent depression: Review, preliminary findings, and implications for theory and practice. Behavior Modification. 2006;30:647–672. doi: 10.1177/0145445504272979. [DOI] [PubMed] [Google Scholar]
- Hollingshead AB. Four factor index of social status. New Haven, CT: Yale University Press; 1976. [Google Scholar]
- Hughes A, Kendall P. Prediction of cognitive behavior treatment outcome for children with anxiety disorders: Therapeutic relationship and homework compliance. Behavioural and Cognitive Psychotherapy. 2007;35:487–494. doi: 10.1017/S1352465807003761. [DOI] [Google Scholar]
- Jungbluth N, Shirk S. Therapist strategies for building involvement in cognitive–behavioral therapy for adolescent depression. Journal of Consulting and Clinical Psychology. 2009;77:1179–1184. doi: 10.1037/a0017325. [DOI] [PubMed] [Google Scholar]
- Kazantzis N, Whittington C, Dattilio F. Meta-analysis of homework effects in cognitive and behavioral therapy: A replication and extension. Clinical Psychology: Science and Practice. 2010;17:144–156. doi: 10.1111/j.1468-2850.2010.01204.x. [DOI] [Google Scholar]
- Kazdin A, Bass D, Siegel T, Thomas C. Cognitive-behavioral therapy and relationship therapy in the treatment of children referred for antisocial behavior. Journal of Consulting and Clinical Psychology. 1989;57:522–535. doi: 10.1037/0022-006X.57.4.522. [DOI] [PubMed] [Google Scholar]
- Rossello J, Bernal G. The efficacy of cognitive-behavioral and interpersonal treatments for depression in Puerto Rican adolescents. Journal of Consulting and Clinical Psychology. 1999;67:734–745. doi: 10.1037/0022-006X.67.5.734. [DOI] [PubMed] [Google Scholar]
- Ryum T, Stiles T, Svartberg M, McCullough L. The effects of therapist competence in assigning homework in cognitive therapy with cluster C personality disorders: Results from a randomized controlled trial. Cognitive and Behavioral Practice. 2010;17:283–289. doi: 10.1016/j.cbpra.2009.10.005. [DOI] [Google Scholar]
- Shaffer D, Fisher P, Lucas C, Dulcan M, Schwab-Stone M. NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): Description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child & Adolescent Psychiatry. 2000;39:28–38. doi: 10.1097/00004583-200001000-00014. [DOI] [PubMed] [Google Scholar]
- Shaw BF, Elkin I, Yamaguchi J, Olmsted M, Vallis TM, Dobson KS, Imber SD. Therapist competence ratings in relation to clinical outcome in cognitive therapy of depression. Journal of Consulting and Clinical Psychology. 1999;67:837–846. doi: 10.1037/0022-006X.67.6.837. [DOI] [PubMed] [Google Scholar]
- Shirk S, Gudmundsen G, Crisp Kaplinski H, McMakin D. Alliance and outcome in cognitive-behavioral therapy for adolescent depression. Journal of Clinical Child and Adolescent Psychology. 2008;37:631–639. doi: 10.1080/15374410802148061. [DOI] [PubMed] [Google Scholar]
- Shirk S, Kaplinski H, Gudmundsen G. School-based cognitive-behavioral therapy for adolescent depression: A benchmarking study. Journal of Emotional and Behavioral Disorders. 2009;17:106–117. doi: 10.1177/1063426608326202. [DOI] [Google Scholar]
- Stone E, Morton S, Hulscher M, Maglone M, Roth E, Grimsjaw J, Shekelle P. Interventions That Increase Use of Adult Immunization and Cancer Screening Services: A Meta-Analysis. Annals of Internal Medicine. 2002;136:641–651. doi: 10.7326/0003-4819-136-9-200205070-00006. Retrieved from http://www.annals.org/ [DOI] [PubMed] [Google Scholar]
- Suh C, Strupp H, O’Malley S. The Vanderbilt process measures: The Psychotherapy Process Scale (VPPS) and the Negative Indicators Scale (VNIS) In: Greenberg LS, Pinsof WM, editors. The psychotherapeutic process: A research handbook. New York, NY US: Guilford Press; 1986. pp. 285–323. [Google Scholar]
- Worthington E. Client compliance with homework directives during counseling. Journal of Counseling Psychology. 1986;33:124–130. doi: 10.1037/0022-0167.33.2.124. [DOI] [Google Scholar]