

Abstract
Background:
Queuing theory is the mathematical approach to the analysis of waiting lines in any setting where arrival rate of subjects is faster than the system can handle. It is applicable to healthcare settings where the systems have excess capacity to accommodate random variations.
Materials and Methods:
A cross-sectional descriptive survey was done. Questionnaires were administered to patients who attended the general outpatient department. Observations were also made on the queuing model and the service discipline at the clinic. Questions were meant to obtain demographic characteristics and the time spent on the queue by patients before being seen by a doctor, time spent with the doctor, their views about the time spent on the queue and useful suggestions on how to reduce the time spent on the queue. A total of 210 patients were surveyed.
Results:
Majority of the patients (164, 78.1%) spent 2 h or less on the queue before being seen by a doctor and less than 1 h to see the doctor. Majority of the patients (144, 68.5%) were satisfied with the time they spent on the queue before being seen by a doctor. Useful suggestions proffered by the patients to decrease the time spent on the queue before seeing a doctor at the clinic included: that more doctors be employed (46, 21.9%), that doctors should come to work on time (25, 11.9%), that first-come-first served be observed strictly (32, 15.2%) and others suggested that the records staff should desist from collecting bribes from patients in order to place their cards before others. The queuing method employed at the clinic is the multiple single channel type and the service discipline is priority service. The patients who spent less time on the queue (<1 h) before seeing the doctor were more satisfied than those who spent more time (P < 0.05).
Conclusion:
The study has revealed that majority of the patients were satisfied with the practice at the general outpatient department. However, there is a need to employ measures to respond to the suggestions given by the patients who are the beneficiaries of the hospital services.
Keywords: Hospital, patients, queue, satisfaction
INTRODUCTION
Queuing theory deals with the study of queues which abound in practical situations and arise so long as arrival rate of any system is faster than the system can handle.1,2 Queuing theory is applicable to any situation in general life ranging from cars arriving at filling stations for fuel, customers arriving at a bank for various services, customers at a supermarket waiting to be attended to by a cashier and in healthcare settings.3,4 Queuing theory can be applied to the analysis of waiting lines in healthcare settings. Most of healthcare systems have excess capacity to accommodate random variations, so queuing analysis can be used as short term measures, or for facilities and resource planning. Other use of queuing analysis and simulation in healthcare includes the following:
Walk-in patient clinic, emergency room arrivals, phone calls from physician office to health management organization, outpatient clinics and outpatient surgeries, physician offices, pharmacy, inventory control. Healthcare resource and infrastructure planning for disaster management and public health.5–7
The need for application of queuing theory in healthcare settings is very important because the well being and life of someone is concerned. The time spent by a patient while waiting to be attended to by a doctor is critical to the patient and to the image of the hospital before the public.8–10
Various attempts by the Federal Government of Nigeria to improve on health care services will not yield good results except the issue of time spent by patients at various hospital points is addressed.9
The aim of this report is to study the queuing system at the general outpatient clinic in relation to time spent by patients on the queue and patient satisfaction. The finding should be helpful in improving services at the clinic.
Definition of terms
Queue: Is an aggregation of items waiting for a service function
Arrival Rate: Is the mean rate of arrivals per unit of time and it is often denoted by the Greek letter lambda (λ)
Service Rate: Is the average number of service rendered per unit of time. It is always represented by the Greek letter Mu (μ)
- Service Discipline: Gives the value by which customers to be served are selected. Example:
- First come first served (FIFO)
- Last come first served (LIFO)
- Priority selection rule e.g., male or female customers first
- Behavior of calling population has the following connotations:
- Reneging: A situation whereby someone on a queue decides to leave the service completely
- Baulking: A situation where a customer does not join the queue at all, the customer just wonders around looking for a possible space to shunt the queue
- Jockeying: A situation whereby a particular customer on a queue moves back and forth among queues seeking for the fastest moving queue
- Blocking: Is a situation when a queue system places a limit on queue length.
MATERIALS AND METHODS
This was a cross sectional study carried out at the General Outpatient Clinic of the Ahmadu Bello University Teaching Hospital, Zaria, Nigeria in August-September 2011. Structured questionnaires were administered to all consenting patients who attended the general outpatient clinic during the study period to see a doctor. The first and third authors and medical students collected the data and patients who could not read or write were assisted in filling the questionnaire. The questionnaire sought the patients' demographic characteristics, nature of illness, time spent before reaching the hospital, on the queue to see the doctor and with the doctor. The patients' views about the queuing and patient behavior on the queue were sought.
The patients also offered suggestions on how the time they spend on the queue can be shortened.
A sample size of 210 was obtained using the formula: n = N/1 + Ne2 (Where n is the sample size, N is the total population of patients who attended the clinic over a period of 3 months, e is the degree of freedom i.e., 0.05.
The doctors who attend to the patients were also observed. The queuing method and discipline was observed, as well as the behavior of the queuing population.
Data obtained from the study was analyzed using the statistical package Excel Analyse_it®. The level of statistical significance was set at 0.05.
RESULTS
Demographics
There were 83 males (39.5%) and 127 females (60.5%), aged 4-70 years (Median 30 years). Ninety three (44.3%) of patients were Hausas, 23 (10.9%) Ibos, 20 (9.6%) Yorubas, while 74 (25.2%) were of other tribes including Ebira, Idoma and Igalas.
Seventy three (34.8%) of the patients were students, 46 (21.9%) civil servants, 36 (17.1%) of other professions, 27 (12.8%) businessmen and women, 13 (6.3%) artisans, 8 (3.8%) farmers and 7 (3.3%) were retired.
Nature of patients' medical complaint
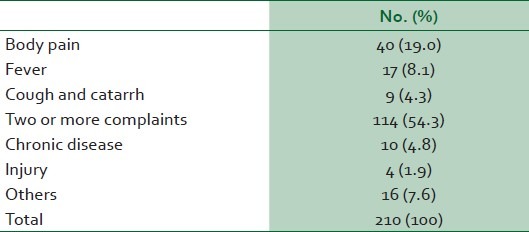
One hundred and fourteen (54.3%) of the patients came to hospital with two or more complaints, 40 (19.0%) with pain in various parts of the body, 17 (8.1%) had fever, 9 (4.3%) cough and catarrh, 10 (4.8%) had chronic disease like hypertension and diabetes, 4 (1.9%) various injuries and 16 (7.6%) had other complaints [Table 1].
Table 1.
Nature of complaint
Estimate time from leaving home to arriving at the general outpatient department
One hundred and forty five (69%) of the patients spent less than an hour to get from home to the General Outpatient Department, 52 (24.8%) 1-2 h, 10 (4.8%) >2-3 h, 2 (0.9%), between >3-4 h and one (0.5%) >4-5 h.
Mode of transportation to the hospital
One hundred and seventy five patients (83.4%) lived within Zaria, 28 (13.3%) outside Zaria but within Kaduna state and 7 (3.3%) other states in Nigeria. One hundred and forty three (68.1%) came to the hospital by public vehicle, 49 (23.3%) by private vehicle, 9 (4.3%) by bicycle or motor cycle, 3 (1.4%) by foot and 6 (2.9%) by various combinations of the above.
Time spent on the queue before seeing the doctor
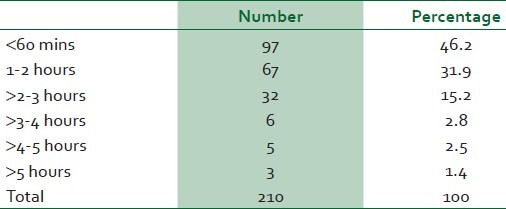
Ninety seven (46.2%) spent less them one hour on the queue before seeing the doctor, 67 (31.9%) 1-2 h, 32 (15.2%) >2 to 3 h, 6 (2.8%) >3-4 h, 5 (2.5%) >4-5 h and 3 (1.4%) above 5 h [Table 2]. Overall, the time spent on the queue before seeing a doctor was 5 min-300 min (median 97.2 min).
Table 2.
Time spent on the queue before seeing the doctor
Time spent with the doctor
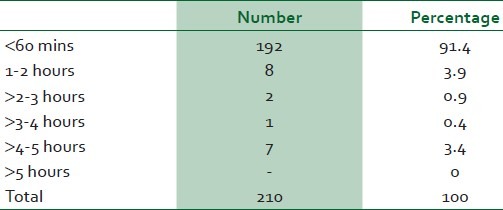
One hundred and ninety two (91.4%) spent less than an hour with the doctor, 8 (3.9%) >1-2 h, 2 (0.9%) >2-3 h, one (0.4%) >3-4 h, 7 (3.4%) >4-5 h and no one spent above 5 h [Table 3]. Overall, the time spent by the patients with the doctor was 20 min-4 h (median 30.3 min).
Table 3.
Time spent with the doctor
Patients' behavior on the queue
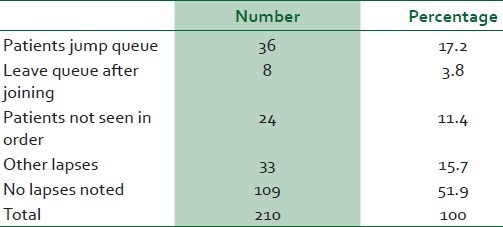
One hundred and nine (51.9%) of the patients did not notice any disorder on the queue for seeing doctor, 36 (17.2%) noticed jumping of queue by patients, 33 (15.7%) a combination of the above, 24 (11.4%) noticed patients being moved by health workers to jump the queue, and 8 (3.8%) left the queue before it got to their turn to be seen by the doctor [Table 4].
Table 4.
Patients’ behavior on the queue
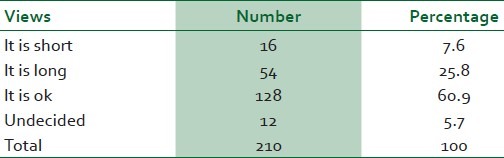
Views on time spent on the queue before being seen by the doctor
One hundred and forty four (68.5%) of patients were satisfied with the time they spent on the queue before being seen by the doctor, 54 (25.8%) felt it was long, and 12 (5.7%) were undecided [Table 5].
Table 5.
Views on time spent on the queue before being seen by the doctor
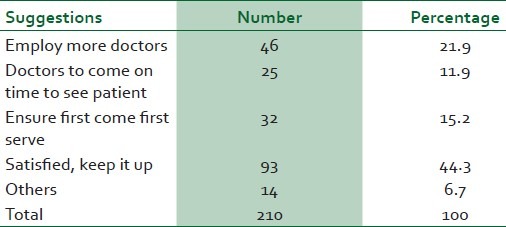
Patients' suggestions
Ninety three (44.3%) were satisfied with the service they received, 46 (21.9%) suggested more doctors be employed, 32 (15.2%) suggested the hospital authorities ensure first come first serve is observed, 25 (11.9%) suggested that the doctors should endeavor to come on time and 14 (6.7%) had other suggestions like making sure that the records clerks do not take bribe from patients in order to put their cards forward before others and a few suggested that the staff of the outpatient clinic be more cordial in handling patients [Table 6].
Table 6.
Suggestions on how to improve on services and especially the time spent on the queue before seeing the doctor
Observations on the queuing system and service discipline by study team
The Multiple Single-Server queuing model is employed at the out-patient department. This implies that patients on arrival to the clinic join a queue to see any out of about 6 to 9 doctors who are consulting at the same time. Each doctor has a line of patients waiting to be attended to and the patients are directed to the queues by the nurses and record staff of the clinic. The patients are directed to queues in the order they arrived. From the point they are seen by the doctor, they proceed to the pharmacy, paying center, the laboratory or home.
The service discipline employed at the outpatient clinic is the priority service, which means that patients are attended to as they are on the queue, but if a very sick patient arrives; the very sick will be taken to see the doctor immediately by passing those on the queue.
DISCUSSION
The queuing system employed at the outpatient department of the Ahmadu Bello University Teaching Hospital is the multiple Single-server queuing model. Once a patient's card is allocated to a doctor, that patient must be seen by that doctor except a more senior doctor request for that patient's card. The implication is that patients can hardly practice jockeying, baulking or reneging and the system cannot be blocked.
The service discipline employed at the general outpatient department is priority service. This implies that patients queue to see the doctor but on the arrival of a very sick patient, the nurses will take the patient immediately to see the doctor, by-passing those on the queue. This may explain why some of the patients suggested that first come-first-serve should be observed at the clinic.
Majority of patients spent less than 2 h on the queue before being seen by a doctor and in the present report, 68.5% of the patients were satisfied with the time they spent on the queue before being seen by the doctor and felt it was short.10 One report found that 56% of patients waited for less than 1 h to see a doctor at a University clinic.11 This is similar to findings in another report where 45% of the respondents were satisfied with their use of the University clinic.11
On patients behavior on the queue 51.4% did not notice any abnormality while a small number (3.8%) were noticed to leave the queue after joining. It may well be that those that left the queue did so to go and collect investigation results to show the doctor. They needed to present first at the clinic to catch a space. This is more likely as no patient is likely to come all the way to the hospital and then leave without seeing a doctor.
Useful suggestions were on how to better position the queuing and other service related practices at the clinic in order to satisfy patients better. A researcher stated that, “The salesman, like a medical doctor must always remain a human being; warm hearted, sympathetic, alive and immediately responsive to every shade or mood of the buyer (or patient).”12 Although the doctors at the clinic are not trained in marketing during medical school, they most likely possess the above qualities since none of the patients complained of maltreatment from the doctors. Some of the suggestions from patients included more doctors be employed to reduce waiting time on the queue, doctors need to come on time to avoid stagnation of patients at the clinic, first-come-first serve discipline should be observed on the queue to ensure fair play, and records staff should not take bribe from patients for the purpose of jumping the queue. In one report from a University clinic, 92% of patients with a complaint were against the records staff.11 A study found similar complaints amongst customers of two commercial banks who felt that the time they spent in the banking hall before being attended to was long (35-40%). The same author found that influential customers and friends of bank managers or senior bank staff do not follow the queue.13 The present study has shown that the time patients spend on the queue before seeing a doctor affects their satisfaction significantly.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Adan I, Resing J. Netherlands: Eindhoren University of Technology Eindhoren; 2002. [Last accessed on 2012 May 22]. Queuing theory department of mathematics and computing science; pp. 1–123. Available from: http://www.queuing.pdf . [Google Scholar]
- 2.Beasley JE. OR-Notes Queuing theory. Queuing theory basics (2000–2009) [Last accessed on 2019 May 22]. Available from: http://www.queue.com.html, & http://www.EventHelix.com .
- 3.Copper RB. Encyclopedia of Computer Science. In: Ralston A, Reilly DE, Hernmentding D, editors. Queuing Theory. 4th ed. Hoboken New Jersey: John Wiley and Sons; 2001. pp. 1496–8. [Google Scholar]
- 4.Fomundans and Hermann. A survey of Queuing theory applications in healthcare (12) 1 SR Technical Report 24. 2007 [Google Scholar]
- 5.Green L. Queuing Analysis in Healthcare. In: Hall RW, editor. Patient flow: Reducing delay in healthcare delivery. New York: Springer; 2006. pp. 201–308. [Google Scholar]
- 6.Mcclain JO. Bed planning using queuing theory models of hospital occupancy: A sensitivity analysis. Inquiry. 1976;13:167–76. [PubMed] [Google Scholar]
- 7.Nosek RA, Jr, Wilson JP. Queuing theory and customer satisfaction, a review of terminology, trends, and applications to pharmacy practice. Hosp Pharm. 2001;36:275. [Google Scholar]
- 8.Schlechter K. The patrioit-News. Hershey medical center to open redesigned emergency room. [Last accessed on 2012 Jun 10]. Available from: http://blog.pennlive.com/midstate-impact/print: entry=/2009/03/Hershey-med-to-o 415/2011 .
- 9.Service Compact with all Nigerians. Abuja: Servicom Office; 2006. The Servicom Book; pp. 1–29. [Google Scholar]
- 10.Akpan AB. 1st ed. Zaria: Kola Ola and Sons; 2003. Total Quality Marketing. [Google Scholar]
- 11.Amuta IA. Being a project submitted to the postgraduate school of Ahmadu Bello University, zaria in partial fulfillment of the requirement for the Award of the degree of Master in Public Health. Zaria: (MPH); 2003. Utilization of university health care facilities by the staff: A case study of the university of agriculture, Makurdi, Nigeria. [Google Scholar]
- 12.Maigida RP. Sale of ethical and nonethical products: A comparative study of the pharmaceutical, food and beverage industries being a project submitted to the postgraduate school of Ahmadu Bello University, zaria in partial fulfillment of the requirement for the Award of the degree of master of Business administration (MBA) 2005 [Google Scholar]
- 13.Ukwenya AA. Customer satisfaction in commercial banking in Nigeria: A comparative study of selected banks in Kaduna state. A postgraduate project submitted in partial fulfillment of the requirement for the award of masters of business administration (MBA) degree. 2002 [Google Scholar]