

Abstract
Early childhood caries leads to early damage, discolouration and gross destruction of the maxillary anterior teeth. This leads to difficulty in speech, decreased masticatory efficiency, development of abnormal tongue thrust and subsequent malocclusion, psychological problems and problem with self-esteem, if aesthetics are compromised. Thus, restoration of severely mutilated primary anterior teeth is often considered as a special challenge, especially in an emotionally immature child. This case documents the restoration of severely mutilated incisors in a patient with early childhood caries.
Background
According to the American Academy of Pediatric Dentistry1 early childhood caries (ECC) is the presence of one or more decayed (non-cavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces in any primary tooth in a child 71 months of age or younger. In children younger than 3 years of age, any sign of smooth-surface caries is indicative of severe ECC (S-ECC). From ages 3 through 5, one or more cavitated, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth or a decayed, missing, or filled score ≥4 (age 3), ≥5 (age 4), or 6 (age 5) surfaces constitutes S-ECC.1 The teeth most often involved are maxillary central incisor, lateral incisor, maxillary and mandibular first molars, while the mandibular primary incisors are relatively unaffected.
ECC is a disease that causes transient disability in a child. The early loss of carious primary incisors may affect the patterns of speech by interfering with the pronunciation of tongue tip consonants (ie,‘t’, ‘d’, ‘s’, ‘sh’ and ‘ch’), and the labial sounds of ‘f’ and ‘v’. Other implications of the loss of primary incisors are decreased masticatory efficiency and the development of abnormal tongue habits, and potentially, subsequent malocclusion. The child may also suffer from psychological problems if aesthetics are compromised.2
In the modern civilised, cosmetically conscious world, well-contoured and well-aligned white teeth set the standard for beauty. In spite of all the recent advancements made in dentistry, restoration of primary incisor has still remained a challenge to all the clinicians because of the small size of the teeth, relatively thin enamel and surface area for bonding, issues related to child's behaviour and finally cost of treatment.3 However, more and more emphasis should be placed these days on paediatric aesthetics. For these reasons, restoring a severely mutilated primary incisor becomes a special challenge to the dentists.
A restorative technique which is able to provide efficient, durable and functional restorations, and which is simple to perform would enhance the management of patients presenting with carious maxillary primary incisors. Such a technique could help to ensure the child's cooperation and reduce the anxieties associated with restorative treatment. Owing to the reduced coronal structure, direct restorative procedures do not always give aesthetics and can be better restored by means of prosthodontic techniques.
We report the case of a 4-year-old boy with severely decayed maxillary anterior teeth that were restored using modified dental metal screw posts.
Case presentation
A 4-year-old boy presented to the Department of Pedodontics and Preventive Dentistry of Teerthanker Mahaveer Dental College & Research Centre, Moradabad, for management of severely decayed primary maxillary anterior teeth. Intraoral examination revealed multiple caries lesion and 51,52,61,62 with pulp involvement (figure 1). The child's medical history was unremarkable. The decision to restore the teeth using composite resin crowns with metal screw post was based on the extensive damage that had occurred to the tooth structure. The treatment plan was explained to the child's parents, and their written consent was obtained before treatment.
Figure 1.

Intraoral photograph showing grossly carious teeth.
Investigations
▸ Diagnostic intraoral periapical radiograph (figure 2).
Figure 2.
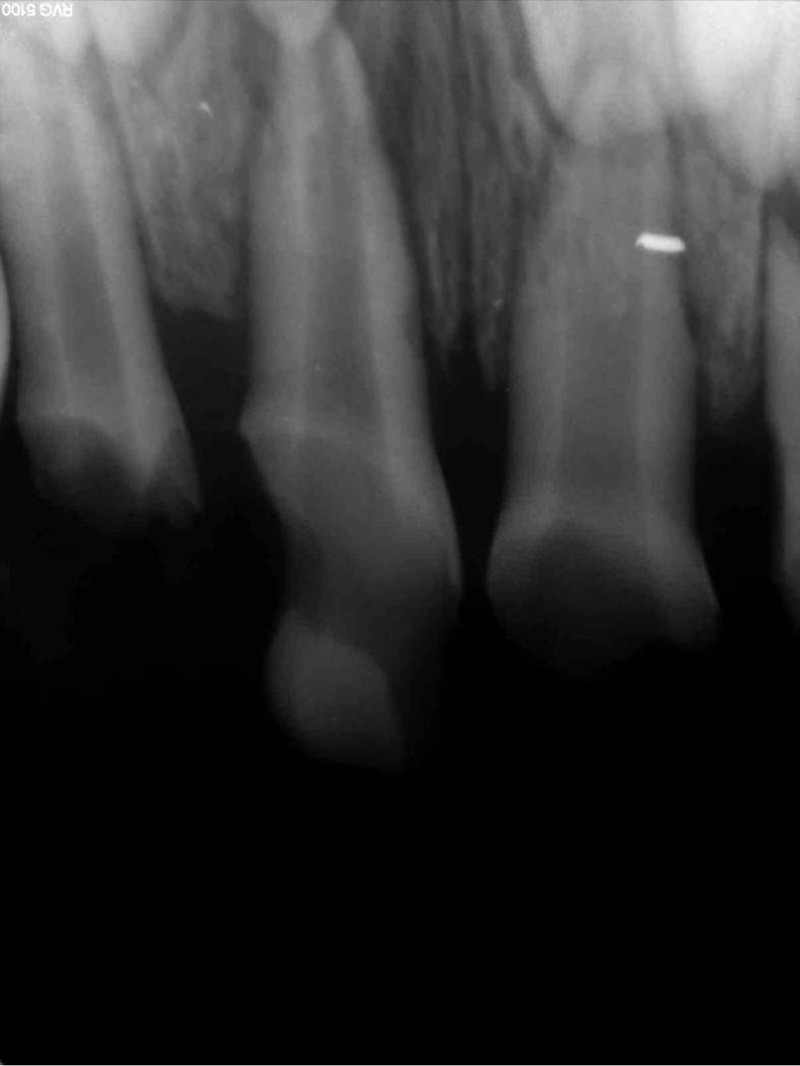
Diagnostic radiograph.
Treatment
Treatment was implemented in two phases, with root canal treatment performed in phase 1 and the construction of the restoration in phase 2. Owing to the patient's age, separate sessions were required for each restoration.
Phase 1
The patient was anaesthetised locally, and the working length of the canal was determined using a number 10 K-file. Canal preparation was performed and enlarged up to 45 number K-file and dried with paper point. The canals were obturated with a calcium hydroxide–iodoform paste (Metapex; Meta Biomed Co, Cheongiu City, Korea), and 3 mm of Metapex was removed and a thin layer of resin-modified glass-ionomer cement (Fuji IX; GC Corporation, Tokyo, Japan) was placed to seal the canal.
Phase 2
Snuggly-fitting number 4 metal screw post (figures 3A and 4) was selected to avoid any fracture because of stress and (Swiss made Dental Gold Plated Screw Posts, Nordin, H, Nordin SA CH-1816 CHAILLY) was modified by trimming its post part to 3 mm and flattening its core part so that strip crown restoration can be easily performed (figure 3B). Intracanal metal short post was luted into the canal using GC Gold Label (figure 5; Glass Ionomer Luting and Lining cement, GC Corporation). Special consideration was given to make sure post is 3 mm into the canal so that it does not interfere with physiological root resorption.
Figure 3.
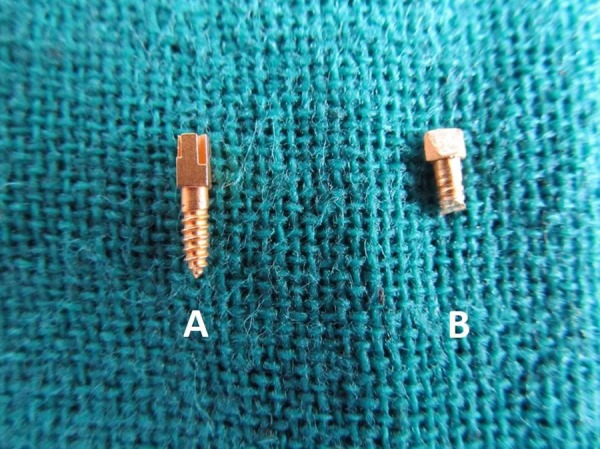
(A) Short number 4 metal screw post. (B) Modified short number 4 metal screw post.
Figure 4.
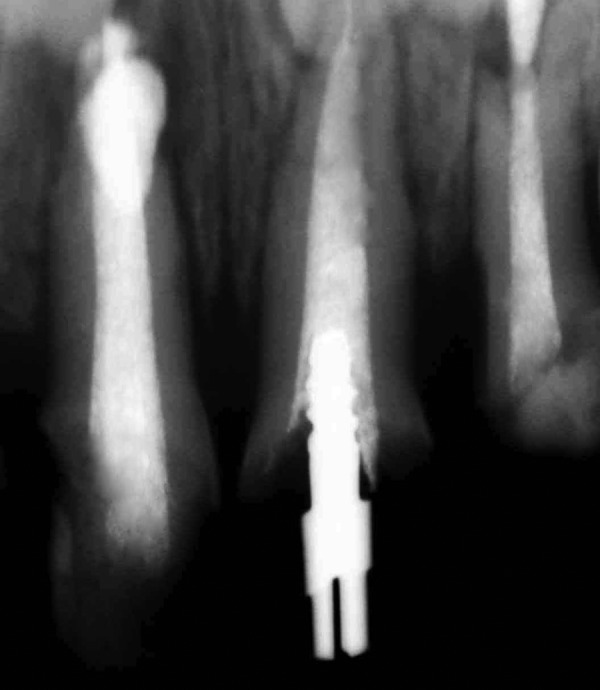
Radiograph showing snuggly-fitted number 4 modified metal screw post.
Figure 5.

Modified metal screw post cemented for better retention and support.
Acid etching was performed followed by bonding of the post and the coronal restoration was completed using celluloid strip crowns (Strip Crown Form-Pedo; 3M/ESPE). Excess composite was removed through small holes punched in the palatal surfaces of the strip crowns, which had been preselected based on tooth mesial and distal width measurements. After polymerisation of the buccal and palatal surfaces, the celluloid crown form was removed by inserting the sharp tip of an explorer at the gingival margin. The occlusion was checked, and the final finishing and polishing was performed using super-snap composite finishing discs by Shofu (figure 6).
Figure 6.

Complete fabrication of the crown.
After the restoration was completed, the patient and his parents were once again instructed on proper dietary and oral hygiene habits as well as the importance of periodic dental visits for preservation of the primary dentition.
Outcome and follow-up
The smile is back, the confidence is back and the happiness on the face of the parents is visible. The patient is functionally and aesthetically sound and after 6 months of follow-up the teeth are intact and stable.
Discussion
Restoring primary anterior teeth that are grossly destructed owing to caries is very challenging for the paediatric dentist. There is a high rate of failure not only because of the absence of tooth structure, poor adhesion of bonding agent to primary teeth, limited availability of materials and techniques, but also because the children who require such restorations are among youngest and least manageable group of patients. To provide shape, function and aesthetics in such teeth, use of intracanal retainer is advised, the remaining coronal structure can be restored with direct or indirect techniques or with single tooth prostheses such as celluloid strip crowns, metal plastic crowns, porcelain veneers, polycarbonate crowns and acrylic resin crowns.4 5
There are a variety of root posts used in paediatric dentistry. A resin composite post building up directly, nickel chromium cast posts, natural teeth from a tooth bank, polyethylene fibres, glass fibre reinforced composite, α-shaped or ω-shaped orthodontic wires or prefabricated metal posts with macroretentive elements.6
The nickel–chromium cast posts, which have been utilised, are not only expensive and require an additional laboratory stage, but also could pose problems during natural tooth exfoliation.6 Natural elements may be used for more aesthetic reasons, but some disadvantages like the need of a tooth bank, donor and recipient acceptance and cross infection make this treatment option impractical.7
Composite post provides satisfactory aesthetics; however, there is risk of loss of retention owing to polymerisation shrinkage. The use of ω-shaped stainless orthodontic wire as an intracanal post is also simple. However, the wire is unable to adequately adapt to the canal form, because it is not the exact copy of the canal thus leading to loss of crown structure.8
The use of conventional prefabricated metal posts is a fast, low cost and simple technique, but is not accepted in paediatric dentistry because of potential interference with physiological root resorption.6
The direct restorative technique used in this report is user friendly and easy to perform, directly in the mouth without any additional laboratory processes; the restoration can be completed in one appointment. Moreover, as there is enough composite material around the core part of the post system to support the strip crown, more aesthetics and shade adaptation are obtained, and no metals show through composite restoration. In addition, the core length of the post system which is placed intracanally is equal to the recommended length for deciduous teeth; 3 mm occupies only the cervical one-third of the canal to avoid interfering with the process of primary tooth root resorption and permanent tooth eruption. The presented technique is simple, economical and easy to perform and practical for all dentists.6
It seems in cases with multiple severe decayed primary anterior teeth, especially in small children with rampant caries, the presented technique is simple, economical and easy to perform and practical for all dentists. However, the possibility of cracked root subsequent to long-term function, especially in children with heavy occlusion or parafunctional habits needs more consideration.
Learning points.
Early loss of primary anterior teeth can lead to psychological disturbances and affect the child's self-esteem and socialisation during the important phase of development.
We can bring back the smile and confidence in the child.
This technique is user friendly, easy to perform and no specialised equipment are required.
Footnotes
Contributors: All the authors have helped in diagnosis and treatment completion.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.American Academy of Pediatric Dentistry. Policy on early childhood caries (ECC): classifications, consequences, and preventive strategies. Pediatr Dent. 2005–2006;27(7 Suppl):31–3. [PubMed]
- 2.Motisuki C, Santos-Pinto L, Giro EM. Restoration of severely decayed primary incisors using indirect composite resin restoration technique. Int J Paediatr Dent 2005;2013:282–6 [DOI] [PubMed] [Google Scholar]
- 3.Paul S, Zahir S. A comparative evaluation of the esthetic crowns for primary anterior teeth, a review of literature. Guident Pedod 2012;2013:52–4 [Google Scholar]
- 4.Usha M, Deepak V, Venkat S, et al. Treatment of severely mutilated incisors: a challenge to the pedodontist. J Indian Soc Pedod Prev Dent 2007;2013:S34–6 [PubMed] [Google Scholar]
- 5.Yui CK, Wei SH. Management of rampant caries in children. Quintessence Int 1992;2013:36–41 [PubMed] [Google Scholar]
- 6.Eshghi A, Esfahan RK, Khoroushi M. A simple method for reconstruction of severely damaged primary anterior teeth. Dent Res J 2011;2013:221–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grewal N, Seth R. Comparative in vivo evaluation of restoring severely mutilated primary anterior teeth with biological post and crown preparation and reinforced composite restoration. J Indian Soc Pedod Prev Dent 2008;2013:141–8 [DOI] [PubMed] [Google Scholar]
- 8.Verma L, Passi S. Glass fibre-reinforced composite post and core used in decayed primary anterior teeth: a case report. Case Rep Dent 2011;2013:4. [DOI] [PMC free article] [PubMed] [Google Scholar]