

Abstract
A pericardial cyst is a rare and benign congenital malformation, usually discovered in the third or fourth decade of life. Its clinical presentation is variable, as it may be asymptomatic or present with chest pain, shortness of breath, or rarely with cardiac tamponade and arrhythmias. We present an interesting case of a woman presenting with chest pain who was found to have a pericardial cyst.
Background
A pericardial cyst is a rare and benign congenital malformation, usually discovered in the third or fourth decade of life.1 Its clinical presentation is variable, as it may be asymptomatic or present with chest pain, shortness of breath, or rarely with cardiac tamponade and arrhythmias.2–4
Case presentation
A woman presented with acute pleuritic chest pain that had started after a long road trip. Her medical history included deep venous thrombosis, pulmonary embolism, hypertension and hypothyroidism. She described right shoulder discomfort radiating to the left shoulder, culminating in the substernal area. Review of systems revealed progressive shortness of breath over several months duration. Physical examination including vital signs was unremarkable.
Investigations
Routine blood work showed blood counts, urea nitrogen, creatinine, electrolytes, liver function tests and cardiac enzymes within normal range.
Differential diagnosis
On initial evaluation, we were concerned for a pulmonary embolism. Other differentials included acute coronary syndrome, musculoskeletal chest pain, gastro-oesophageal reflux disease and panic disorder. We proceeded with further investigations as discussed below.
Outcome and follow-up
We obtained a chest x-ray (figure 1) which showed a homogeneous density in the right lower lobe. A CT chest (figure 2) revealed an 11×11 cm fluid-filled pericardial cyst in the right chest without evidence of a pulmonary embolism. The patient had an elective cardiac catheterisation which did not reveal any significant coronary obstruction. She next underwent right thoracotomy with successful removal of the pericardial cyst. Pathologically, it was bilobed with a partition. It measured 11 cm and originated towards the lateral aspect of the pericardium near the right atrium. Her symptoms improved after the surgery. She was discharged with follow-up.
Figure 1.
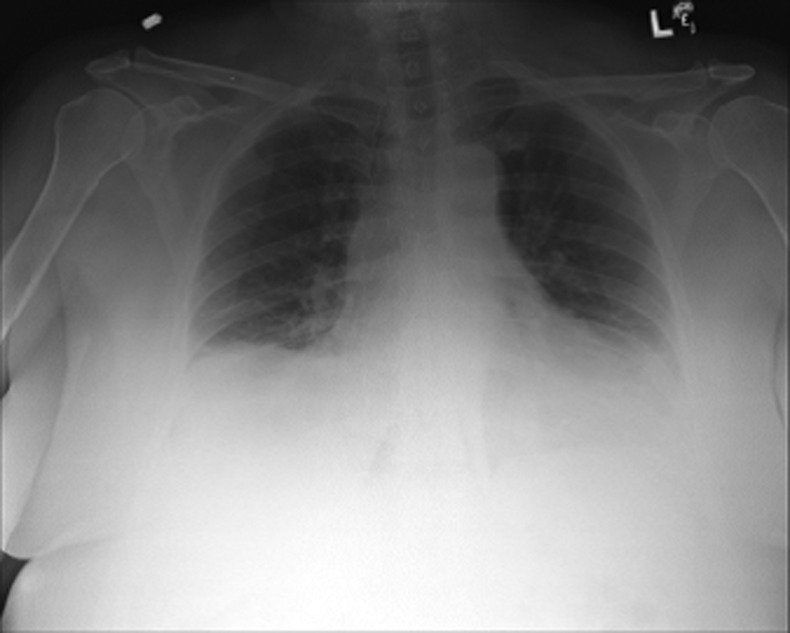
Chest radiograph with right lower lobe opacification.
Figure 2.

CT scan of the chest with contrast revealing a large pericardial cyst encroaching upon the heart.
Discussion
Pericardial cyst occurs in the population at a rate of one in 100 000.1 It constitutes about one-fifth of all mediastinal masses4 and one-tenth of total mediastinal cysts. Seventy-five percent of all pericardial cysts are asymptomatic;5 most discovered incidentally on routine chest roentgenogram or echocardiography.1 They are thought to result from failure of fusion of mesenchymal lacunae during the developmental phase which forms pericardium.1 4 In this case the cyst was quite large, 11 cm in size. Symptoms usually result from compression of adjacent structures, ranging from chest pressure, chest pain, cough, shortness of breath and right bronchus obstruction to life-threatening events such as large vessel obstruction, arrhythmia or tamponade. A few cysts resolve spontaneously, perhaps with rupture into the pleural space. Diagnosis is usually confirmed by imaging with contrast CT, echocardiogram or MRI. No single imaging modality has been found superior to the others. Management of a pericardial cyst includes observation,6 percutaneous aspiration or surgical resection. In asymptomatic patients, observation may be done by serial CT scanning.1 Surgical resection, the only definitive treatment, is another option, depending on the size of the cyst, symptoms, patient's preference and prevention of life-threatening complications. Our patient's cyst was large enough to cause symptoms, so surgical resection was recommended. Approaches for surgical resection include thoracostomy and thoracoscopy.
Learning points.
Pericardial cysts are uncommon benign congenital malformations with size-dependent symptoms from compression affects.
It may be discovered on routine imaging studies in the course of evaluating the patient's symptoms.
Definitive treatment is surgical resection.
Footnotes
Competing interests: None.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Wael FE, Kieran H. Pericardial cyst: an unsual cause of pneumonia. BioMed Central Cases J 2013:26 [Google Scholar]
- 2.Ersin O, Mustafa A, Abdullah H, et al. Giant, dumbbell-shaped pericardial cyst. Tex Heart Inst J 2007;2013:3. [PMC free article] [PubMed] [Google Scholar]
- 3.Thomas K, Prabhat KS, Satyajeet M, et al. Pericardial cyst. Ann Card Anaesth 2008;2013:129–30 [Google Scholar]
- 4.Pankaj K, Kalyana J, Shahme AF, et al. Massive benign pericardial cyst presenting with sinultaneous superior vena cava and middle lobe syndromes. J Cardiothorac Surg 2008;2013:32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.John D, Peter T, Loutsia F. An asymptomatic giant pericardial cyst. Int J Cardiol 2001;2013:185–7 [DOI] [PubMed] [Google Scholar]
- 6.Bradley AS, Helen SB. Pericardial cyst. N Engl J Med 2004;2013:21 [Google Scholar]