

Abstract
We report a case of life-threatening hematemesis due to portal hypertension caused by an isolated arterioportal fistula (APF). Intrahepatic APFs are extremely rare and are a cause of presinusoidal portal hypertension. Etiologies for APFs are comprised of precipitating trauma, malignancy, and hereditary hemorrhagic telangiectasia, but these were not the case in our patient. Idiopathic APFs are usually due to congenital vascular abnormalities and thus usually present in the pediatric setting. This is one of the first cases of adult-onset isolated APF who presented with portal hypertension and was successfully managed through endoscopic hemostasis and subsequent interventional radiological embolization.
Keywords: Arterioportal fistula, Pre-sinusoidal portal hypertension, Hepatic vein pressure gradient, Hepatic artery embolization
INTRODUCTION
Portal hypertension is defined as the increase in porto-systemic resistance and/or flow[1]. The causes of portal hypertension can be divided into pre-, intra-, and posthepatic causes. Moreover, intrahepatic portal hypertension can be further categorized into three groups: pre-, intra-, and postsinusoidal causes. The most common etiology of portal hypertension is due to liver cirrhosis which accounts for 90% of the cases in the United States[2]. It is a cause of intrasinusoidal portal hypertension due to distortion of the hepatic lobular architecture and results in hyperdynamic splanchnic circulation. The second major cause of portal hypertension is due to extrahepatic portal vein thrombosis, accounting for 7% of cases. The remaining 3% of causes of portal hypertension encompasses a variety of rare etiologies, including our case of intrahepatic presinusoidal portal hypertension[2]. While infrequent, the causes for presinusoidal portal hypertension comprise of schistosomiasis, myeloproliferative diseases, sarcoidosis, hepatic portal fibrosis, primary biliary cirrhosis, arsenic toxicity, idiopathic portal hypertension[3].
CASE REPORT
The patient is a 30 year old male who presented to Los Angeles County-University of Southern California Medical Center with a two day history of hematemesis. The physical examination on arrival showed vital signs of a blood pressure of 93/61 mmHg, a heart rate of 135 beats per minute with exam findings significant for splenomegaly and left femoral artery bruit, but otherwise negative for shifting dullness, spider angiomata, palmar erythema, asterixis, and jaundice. Pertinent laboratory values were as follows: alkaline phosphatase 175 units/L, total protein 6.3 g/dL, albumin 3.9 g/dL, total bilirubin 0.6 mg/dL, aspartate aminotransferase 39 units/L, alanine transaminase 72 units/L, prothrombin 14.5 s, INR 1.16, hemoglobin 13.5 g/dL, white blood cells 8.0 k/cumm, and a platelet count of 79 × 103/cumm. Further testing was done and showed all viral hepatitis, autoimmune, and metabolic liver disease markers to be negative. No history of alcohol intake and no history of prescribed, over the counter or supplement medications. His family history was negative for liver disease.
Upon presentation, the patient underwent an emergent esophagogastroduodenoscopy, which showed four columns of esophageal varices with active bleeding. Band ligation of the varices was performed successfully. Subsequent abdominal ultrasound demonstrated splenomegaly (length 14.8 cm) but a normal size, smooth liver surface and homogeneous liver parenchyma, suggesting a non-cirrhotic etiology for the portal hypertension. A multiphase computed tomography (CT) examination of the liver demonstrated the left portal vein was highlighted at the arterial phase, strongly suggesting the existence of a hepatic arterioportal communication (Figure 1A). Based upon this finding, it was speculated that the overflowing of the portal vein due to the shunt between the hepatic artery to the portal vein was causing presinusoidal portal hypertension. In order to further confirm this, a hepatic venous pressure gradient (HVPG) measurement was performed and indicated normal value; 2 mmHg (< 5 mmHg is normal). Along with the signatures of portal hypertension-variceal bleeding and splenomegaly-the normal HVPG was consistent with pre-sinusoidal portal hypertension. To further confirm this, an angiogram was performed. A brisk contrast opacification of the left portal vein was noted upon contrast injection into the left hepatic artery, which branched from left gastric artery, confirming arterioportal shunting (Figure 1B). The shunting was determined not to be direct, but passing through a network of small capillary-like “fuzz” prior to brisk drainage into the portal system (Figure 1C). Furthermore, angiography showed the right superficial femoral artery with pseudoaneurysm and fistula and this additional vascular abnormality support our diagnosis of arterioportal fistulas (APFs) of congenital etiology. Taken all together, it was concluded that the arterioportal fistula is the cause of this patient’s non-cirrhotic portal hypertension. The arterioportal and femoral artery fistulas were also closed with catheter directed embolization utilizing the liquid embolic agent Onyx® (ev3 Endovascular Inc., Plymouth, MN, United States). Following the embolization, no further early portal vein enhancement was seen during left hepatic arteriogram (Figure 1D). Finally, a liver biopsy was performed showing focal portal venule dilatation with dilated outflow vessels, but was otherwise normal, compatible with the clinical diagnosis of presinusoidal portal hypertension secondary to the hepatic artery and portal vein shunt (Figure 2). Post-embolization recovery of the patient has been uneventful, and no additional episodes of upper gastrointestinal bleeding have been reported by the patient on two subsequent clinic visits during the last four months.
Figure 1.
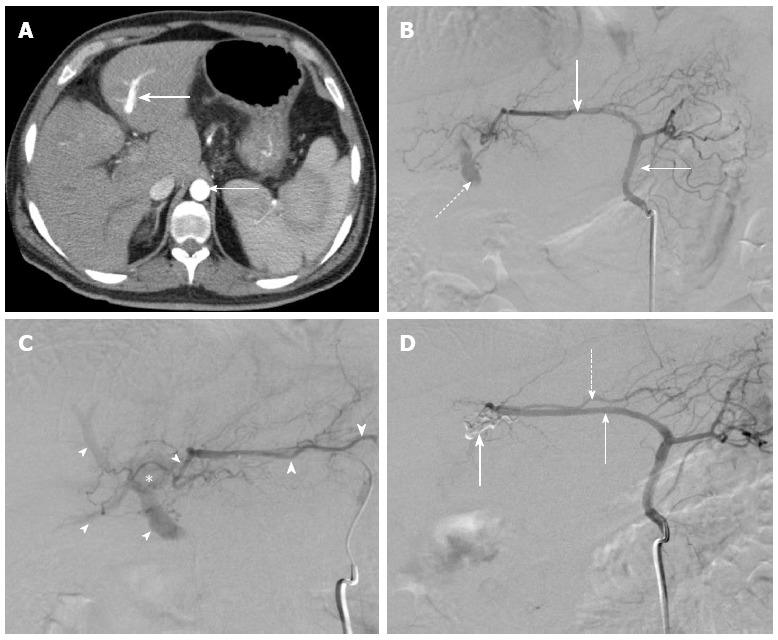
Intrahepatic communication between hepatic artery and portal vein. A: Contrast enhanced axial computed tomography of the abdomen demonstrating similar contrast opacification of the aorta (thin arrow) and the left portal vein (thick arrow); B: Left gastric arteriogram demonstrates gastrohepatic trunk (thin arrow) giving rise to aberrant left hepatic artery (thick arrow). Note early opacification of the portal vein (dashed arrow); C: Selective arteriogram with coaxial microcatheter in the left hepatic artery demonstrates medial branch of the left hepatic artery (large arrowheads) contributing to a parenchymal blush (star) and leading to opacification of the portal veins (small arrowheads). Note the normal appearance of the lateral branch of the left hepatic artery (thick arrow); D: Post-embolization arteriogram in the gastrohepatic trunk demonstrates opacification of the left hepatic artery (thin arrow). Onyx cast (thick arrow) is seen occupying the previously seen medial branch of the left hepatic artery. No further opacification of the portal veins is seen. Note the preserved lateral branch of the left hepatic artery (dashed arrow).
Figure 2.
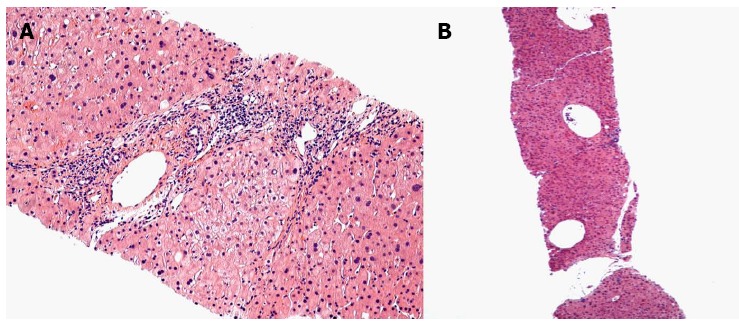
The hepatic histology of arterioportal fistula. A: This low power image shows a small portal tract in the center of the field that has a markedly dilated portal venule. The terminal hepatic (central) venules above and below the portal tract are markedly dilated; B: The portal venule is slightly dilated and there are increased numbers of small portal venous radicals.
DISCUSSION
HVPG measurements often provide valuable information in identification of the site or cause of the portal hypertension[4]. The HVPG is the difference between the wedged and free hepatic venous pressures, which has been shown to correlate well with actual portal vein pressure[5]. Its increase is consistent with sinusoidal portal hypertension and is known to be a predictor of development of varices and ascites[6]. Upon visualization of the hepatic artery and portal vein communication through CT, the measurement of HVPG was conducted. The classic pattern of the prehepatic or intrahepatic presinusoidal portal hypertension shows normal HVPG and free hepatic vein pressure (FHVP) along with the stigmata of portal hypertension. The pathophysiology consists of a presinusoidal block preventing the transmission of the elevated portal pressure to the sinusoid, thus resulting in a normal wedged hepatic vein pressure[5]. In our case, the HVPG value was consistent to the pathophysiology of presinusoidal portal hypertension.
Most of the literature regarding APFs is focused on the following etiologies: precipitating trauma, hepatocellular carcinoma (HCC), congenital, and in the context of hereditary hemorrhagic telangiectasia (HHT)[7]. Clinical presentation of APFs varies from asymptomatic to symptoms related to congestive heart failure (40%-60%), portal hypertension (20%-40%), and diarrhea with abdominal pain secondary to a “steal” phenomenon (20%)[8]. Hepatic trauma is a common cause for APFs. It may be from penetrating trauma such as gunshot wounds, a complication of liver transplantation or from previous liver biopsies[9,10]. HCC can cause APFs and two studies have shown that APFs may occur in up to 60% of patients with HCC[10,11]. Congenital APFs are associated with portal hypertension, failure to thrive, and gastrointestinal hemorrhage in infancy or early childhood[7,12]. In general, it is noted that less than 10% of all APFs are congenital[13]. As for HHT, hepatic involvement has been reported in 8%-78% of cases in retrospective and prospective studies[14]. Our patient did not have the any history suggestive of congenital APF or signatures of HHT. Furthermore, he had no abdominal trauma or surgery, malignancy and no previous liver biopsies. Moreover the incidental finding of the femoral arteriovenous fistula and unique variation of hepatic artery further imply the congenital etiology. Therefore, we believe that this is a case of adult onset congenital APF that likely did not present in infancy or childhood because his fistula is through a capillary connection and probably took multiple decades to develop clinical manifestation. Based our intensive literature search, this is one of the first cases reported to be adult onset portal hypertension due to congenital APFs.
Treatment of the APFs through shunt reduction is either surgical or minimally invasive though interventional radiology (IR) techniques. In the past, surgical ligation of the supplying artery was performed, however with the advancement of interventional radiology techniques, the trend has now shifted to endovascular catheter directed therapy[15]. IR directed therapy offers many advantages over the conventional surgical treatment and is now the preferred technique for treatment. These advantages include decreased morbidity and mortality, reduced risk of subsequent complications, and significant reduction in the time required for recovery. IR directed therapy is accomplished through hepatic artery embolization (HAE)[16]. Embolization is usually performed with metal coils, detachable balloons, or gelfoam[17,18]. However at selected centers such as ours, liquid embolic agents are also utilized. Types of liquid embolic agents include ethylene vinyl alcohol (Onyx®) and N-butyl cyanoacrylate, both of which are predominantly used in congenital APFs per the literature[17,18]. HAE complications do occur, and include non-target embolization, hepatic infarction, and ischemic cholangitis. In a series of 15 patients studied by Chavan et al[19] ischemic cholangitis and/or cholecystitis occurred in three patients and one patient died of hepatic necrosis leading to multi-organ failure. Nevertheless, due to the dual blood supply of the liver (hepatic artery and portal vein), infarctions are rare[16]. In our limited experience with IR therapy of hepatic APFs, no such complications have occurred.
In summary, we described a case of lethal variceal bleeding due to an adult onset congenital APF. The patient was successfully treated through radiological interventional therapy and is being monitored regularly in our outpatient clinic without any further episodes of bleeding.
ACKNOWLEDGMENTS
We would like to acknowledge Dr. Neil Kaplowitz for critical review of the manuscript.
Footnotes
P- Reviewers Diamantis I, Grattagliano I S- Editor Huang XZ L- Editor A E- Editor Zhang DN
References
- 1.Bari K, Garcia-Tsao G. Treatment of portal hypertension. World J Gastroenterol. 2012;18:1166–1175. doi: 10.3748/wjg.v18.i11.1166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.García-Pagán JC, Gracia-Sancho J, Bosch J. Functional aspects on the pathophysiology of portal hypertension in cirrhosis. J Hepatol. 2012;57:458–461. doi: 10.1016/j.jhep.2012.03.007. [DOI] [PubMed] [Google Scholar]
- 3.Sherlock S. Classification and functional aspects of portal hypertension. Am J Surg. 1974;127:121–128. doi: 10.1016/0002-9610(74)90146-9. [DOI] [PubMed] [Google Scholar]
- 4.Nagral A, Patch D, Burroughs AK. Portal hemodynamics in chronic liver disease. Indian J Gastroenterol. 1999;18:78–83. [PubMed] [Google Scholar]
- 5.Kumar A, Sharma P, Sarin SK. Hepatic venous pressure gradient measurement: time to learn! Indian J Gastroenterol. 2008;27:74–80. [PubMed] [Google Scholar]
- 6.Perelló A, Escorsell A, Bru C, Gilabert R, Moitinho E, García-Pagán JC, Bosch J. Wedged hepatic venous pressure adequately reflects portal pressure in hepatitis C virus-related cirrhosis. Hepatology. 1999;30:1393–1397. doi: 10.1002/hep.510300628. [DOI] [PubMed] [Google Scholar]
- 7.Garcia-Tsao G, Korzenik JR, Young L, Henderson KJ, Jain D, Byrd B, Pollak JS, White RI. Liver disease in patients with hereditary hemorrhagic telangiectasia. N Engl J Med. 2000;343:931–936. doi: 10.1056/NEJM200009283431305. [DOI] [PubMed] [Google Scholar]
- 8.Strodel WE, Eckhauser FE, Lemmer JH, Whitehouse WM, Williams DM. Presentation and perioperative management of arterioportal fistulas. Arch Surg. 1987;122:563–571. doi: 10.1001/archsurg.1987.01400170069010. [DOI] [PubMed] [Google Scholar]
- 9.Ngan H, Peh WC. Arteriovenous shunting in hepatocellular carcinoma: its prevalence and clinical significance. Clin Radiol. 1997;52:36–40. doi: 10.1016/s0009-9260(97)80303-0. [DOI] [PubMed] [Google Scholar]
- 10.Redmond PL, Kumpe DA. Embolization of an intrahepatic arterioportal fistula: case report and review of the literature. Cardiovasc Intervent Radiol. 1988;11:274–277. doi: 10.1007/BF02577034. [DOI] [PubMed] [Google Scholar]
- 11.Allison DJ, Jordan H, Hennessy O. Therapeutic embolisation of the hepatic artery: a review of 75 procedures. Lancet. 1985;1:595–599. doi: 10.1016/s0140-6736(85)92142-7. [DOI] [PubMed] [Google Scholar]
- 12.Garcia-Tsao G. Liver involvement in hereditary hemorrhagic telangiectasia (HHT) J Hepatol. 2007;46:499–507. doi: 10.1016/j.jhep.2006.12.008. [DOI] [PubMed] [Google Scholar]
- 13.Vauthey JN, Tomczak RJ, Helmberger T, Gertsch P, Forsmark C, Caridi J, Reed A, Langham MR, Lauwers GY, Goffette P, et al. The arterioportal fistula syndrome: clinicopathologic features, diagnosis, and therapy. Gastroenterology. 1997;113:1390–1401. doi: 10.1053/gast.1997.v113.pm9322535. [DOI] [PubMed] [Google Scholar]
- 14.Kido C, Sasaki T, Kaneko M. Angiography of primary liver cancer. Am J Roentgenol Radium Ther Nucl Med. 1971;113:70–81. doi: 10.2214/ajr.113.1.70. [DOI] [PubMed] [Google Scholar]
- 15.Ridout DL, Bralow SP, Chait A, Nusbaum M. Hepatoportal arteriovenous fistula treated with detachable balloon embolotherapy. Am J Gastroenterol. 1989;84:63–66. [PubMed] [Google Scholar]
- 16.Applbaum YN, Renner JW. Steel coil embolization of hepatoportal fistulae. Cardiovasc Intervent Radiol. 1987;10:75–79. doi: 10.1007/BF02577970. [DOI] [PubMed] [Google Scholar]
- 17.Zanjani KS, Mazloumi M, Zeinaloo A, Hedayati M, Khalilzadeh O, Yazdi HR. Transcatheter embolization of congenital hepatic arteriovenous malformation using ethylene-vinyl alcohol copolymer (Onyx) Diagn Interv Radiol. 2012;18:231–235. doi: 10.4261/1305-3825.DIR.4418-11.0. [DOI] [PubMed] [Google Scholar]
- 18.Cil BE. Transhepatic embolization of a recanalized congenital hepatic arterioportal fistula with NBCA and coils. Cardiovasc Intervent Radiol. 2004;27:172–174. doi: 10.1007/s00270-003-0152-4. [DOI] [PubMed] [Google Scholar]
- 19.Chavan A, Caselitz M, Gratz KF, Lotz J, Kirchhoff T, Piso P, Wagner S, Manns M, Galanski M. Hepatic artery embolization for treatment of patients with hereditary hemorrhagic telangiectasia and symptomatic hepatic vascular malformations. Eur Radiol. 2004;14:2079–2085. doi: 10.1007/s00330-004-2455-5. [DOI] [PubMed] [Google Scholar]