

Description
Perilunate dislocations are high-energy injuries that are uncommon. The literature suggests that up to 25% of cases may be missed.1 2 Here we present an acute lunate dislocation in a young man who fell from a height of 12 feet onto an extended, outstretched right hand. Plain radiographs demonstrated classical signs of a perilunate dislocation (figures 1 and 2). He also sustained fractures of the radial and ulnar styloid, indicating a variant of a greater arc injury.3 Following a failed closed reduction the patient proceeded to open reduction and percutaneous Kirschner wire fixation, with repair of the inter-carpal ligaments.
Figure 1.

Anteroposterior (AP) view of the wrist.
Figure 2.

Lateral view of the carpus.
True lunate dislocation is stage 4 of the Mayfield's classification. Key radiological findings include:
Dislocation of the lunate from the lunate fossa (usually volar) into the space of poirier, also known as the ‘spilled tea cup’ sign, with loss of colinearity of the radius, lunate and capitate
Interruption of Gilula's lines
The ‘piece of pie’ sign representing the lunate on true Anteroposterior (AP) x-ray views
Lunate and capitate overlap
An abnormal scapho-lunate angle of >70 or <30°.
Figures 3 and 4 demonstrate the features outlined above, and knowledge of these will reduce the risk of missing these significant injuries. These are important injuries to recognise as complications include median nerve injury, long-term carpal instability and chronic pain.2 3
Figure 3.

Annotated AP view of the wrist. The ‘piece of pie’ classical triangular shape of the lunate is seen (arrow A), with associated greater arc injury with fractures of the radial and ulnar styloid, and interruption of Gilulas lines (labelled B).
Figure 4.
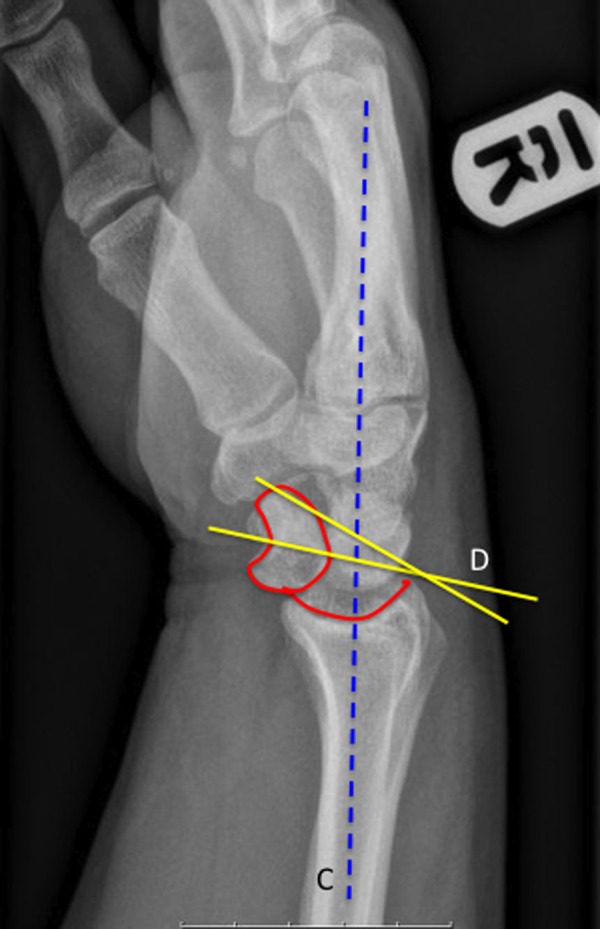
Annotated lateral view of the carpus. The ‘spilt tea cup’ sign can be seen (in red) as the lunate is rotated and displaced volarly with respect to the radial articular surface, with subsequent loss of colinearity (line C) where the lunate does not lie on the collinear axis. The scapolunate angle (D) is abnormal (normal range 30–60°), and the hamate and lunate overlap.
At the patient's last clinic review, the K-wire was kept in situ. Plain x-ray demonstrates a reduced lunate. He remains under clinical follow-up.
Learning points.
Up to 25% of these injuries are missed, with catastrophic long-term consequences for the patient. Therefore, open reduction with repair of the ligamentous structure is often required.
Knowledge of the classical radiological features of lunate dislocation—particularly the ‘spilt tea cup’ sign, the ‘piece of pie’ sign and loss of Gilula's lines. Associated injuries can also be present, which may distract the clinician and result in a missed diagnosis of a lunate dislocation.
Knowledge of the above signs is essential in preventing delayed, or missed diagnosis.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Herzberg G, Comtet JJ, Linscheid RL, et al. Perilunate dislocations and fracture dislocations: a multicenter study. J Hand Surg [Am] 1993;2013:768–79 [DOI] [PubMed] [Google Scholar]
- 2.Newberry JA, Garmel GM. Image diagnosis: perilunate and lunate dislocations. Perm J 2012;2013:70–1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gaebler C. Fractures and dislocations of the carpus. In: Bucholz RW, Heckman JD, Court-Brown C, Tornetta P, Koval KJ. Rockwood and Green's fractures in adults. Philadelphia: Lippincott Williams & Wilkins, 2005;857–908 [Google Scholar]