

Abstract
Stroke is an important clinical problem and some strokes are caused by a cardiac thrombus. Although large thrombus in the left atrium (LA) is known, small-sized LA thrombus is rare. LA thrombus or a left atrial appendage (LAA) thrombus is well known to cause ischaemic stroke in patients with atrial fibrillation (AF). For patients with AF, anticoagulants are recommended to prevent stroke. 64-slice multidetector CT (64-MDCT) can estimate not only the coronary artery stenosis, but LAA thrombus and small pulmonary vein thrombus (PVT). This study demonstrated the thrombi in the left lower pulmonary vein to LA in a 70-year-old man without AF by 64-MDCT. The LA thrombi were identified by transthoracic echocardiography, the size of which was 30.2 mm×8.1 mm. PVT and the small LA thrombus seem to have been significantly underestimated. 64-MDCT is a useful tool to estimate PVT and LA thrombi promptly.
Background
Ischaemic stroke is the third-leading cause of death and the most common cause of long-term disability, which is a primary clinical problem with significant morbidity, mortality and socioeconomic impact worldwide.1 There are various causes of cerebral ischaemia, but the primary pathophysiological mechanisms are intracranial small artery disease, and cardiac embolism.
Cardiac embolism accounts for more than 15% of ischaemic strokes, which is usually derived from a thrombus at left atrial appendage (LAA). Patients with non-valvular AF may be categorised as high-risk patients. About two-third to three-fourth of ischaemic stroke events occur in non-valvular AF. The cause for stroke is primary embolisation of the thrombi formed in the left atrium (LA) or the left atrial appendage (LAA) in patients with atrial fibrillation (AF). Long-term anticoagulation with warfarin is an option for the prevention of stroke in patients with AF. But many of stroke patients do not have AF.
A left ventricle (LV) thrombus is formed in patients with ischaemic cardiomyopathy, dilated LV, lower ejection fraction and apical aneurysm.
The LA thrombi are uncommon and may be associated with thrombosis such as cerebral infarction. Although the large LA thrombi are reported by transthoracic echocardiography (TTE), transoesophageal echocardiography (TEE) or MRI, the report of small LA thrombus is in a few cases.
Pulmonary vein thrombosis (PVT) is a potentially life-threatening condition and is thought to be rare. The symptoms of PVT can be non-specific and subtle before occurring systemic thrombosis such as cerebral infarction, so the disease is often undiagnosed. And the ways to detect the disease is unclear. But in 2012, we had reported two cases of the small pulmonary vein thrombi by using 64-slice multidetector CT (64-MDCT).2 3
The 64-MDCT angiography has recently become an optional diagnostic method to assess coronary artery plaque.4 The advantage of the MDCT angiography is that the modality is a non-invasive technique that enables evaluation of vascular anomalies and thrombus not only in LAA but in the pulmonary vein in the same study.
In this study, 64-MDCT demonstrated the thrombi, which expanded from the right lower pulmonary vein to the LA in patients without AF.
Case presentation
The patient was a 70-year-old man with angina pectoris. He had been treated with percutaneous coronary intervention, and had had four stents in the coronary artery (#1,#6, #11 and high lateral). He was treated with 100 mg aspirin, but no previous treatment with warfarin had been provided. The patient was referred to our hospital for the evaluation of restenosis of stents in the coronary artery. The chest roentgenogram showed no lung cancer. The patient had no symptoms of cough, sputum or cerebral infarction. The large thrombi in the left lower pulmonary vein and in the LA were detected in axial (figure 1) and sagittal (figure 2) images as the defect of enhancement by 64-MDCT scan. TTE demonstrated the thrombi in the left atrium, and the size of the thrombus was 30.2 mm×8.1 mm (figure 3). The patient had no thrombus in the LAA.
Figure 1.
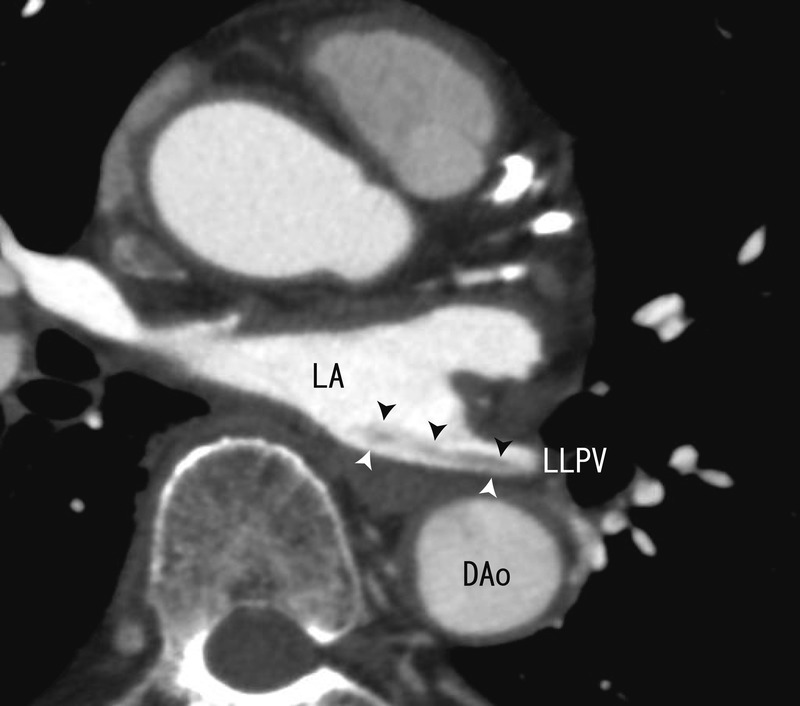
The 64-multidetector CT axial images showing the thrombi from the left lower pulmonary vein to left atrium (white and black arrow head) as the defect of enhancement. Dao, descending aorta, LA, left atrium, LLPV, left lower pulmonary vein.
Figure 2.
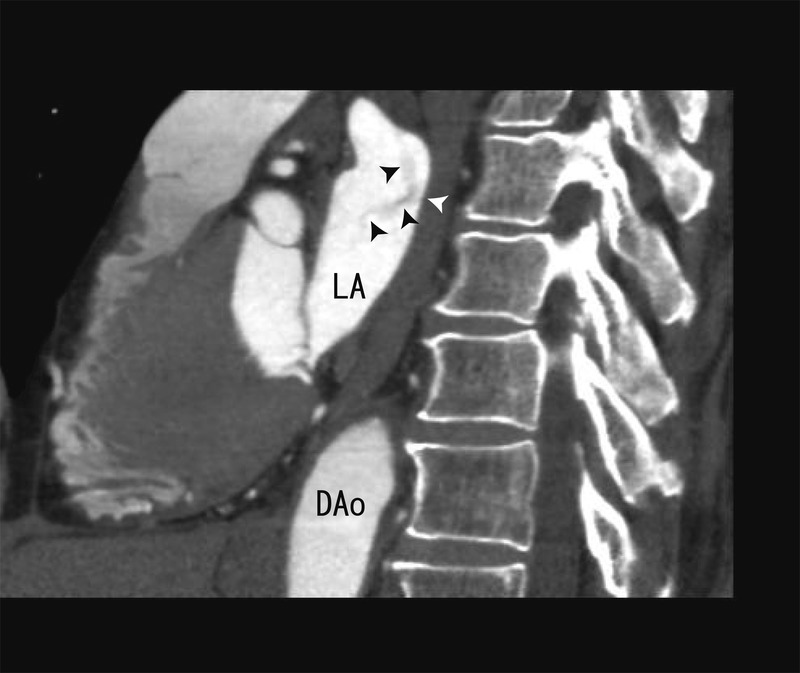
The 64- multidetector CT sagittal images showing the thrombi from the left lower pulmonary vein to left atrium (white and black arrow head). The merge of the thrombi was vague. A part of the thrombi seemed to be attached to the posterior wall of LA. Dao, descending aorta, LA, left atrium.
Figure 3.

Images of transthoracic echocardiography. The thrombi in the left atrium were surrounded by white arrow head, which were located at the posterior wall side in LA. The echo level of the thrombi was high, which represented that the thrombi was fibrous. The size of thrombi was 30.2 mm×8.1 mm. LA, left atrium, LV, left ventricle, RA, right atrium, RV, right ventricle.
Treatment
100 mg aspirin intradermally.
Discussion
The symptoms of PVT are non-specific or subtle before systemic thrombosis such as ischaemic stroke occurs, so the disease has been undiagnosed. The ways to detect the disease are being searched. In 2012, we reported two cases of the PVT by using 64-MDCT scan, which is small thrombi in the right upper pulmonary vein2 and in the left upper pulmonary vein.3 In the present case, we reported a large thrombi in left lower pulmonary vein, which were connected to thrombi in LA. And thrombi in LA could be identified by TTE (figure 3).
Although large LA thrombi are confirmed by TTE, TEE or MRI, the reports of the small LA thrombi are few. But, in the present case, the thrombi in LA are not so large compared with what had already been reported. It is difficult to distinguish small-sized thrombi from artefacts by only TTE. We can confirm the LA thrombi by 64-MDCT scan. 64-MDCT scan can identify not only PVT but small LA thrombus.
AF is a common arrhythmia with an incidence that is as high as 10% in the elderly population. AF is responsible for 10% of all ischaemic strokes and half of all cardioembolic strokes.5 In this case, the patient had no AF. When we assess the patients with angina pectoris (AP), we need to check the thrombi in pulmonary vein or in LA, which are often connected.
Despite a large thrombus in the left lower pulmonary vein and in LA, patients had no systemic thrombosis such as cerebral infarction. The feature of the thrombi in the pulmonary vein and in LA may be different from the thrombi forming DVT. A part of thrombus of DVT is often separated from DVT and goes into pulmonary artery, which forms pulmonary embolism. But the thrombus in PVT seems not to be separated so easily. And the thrombi in LAA did not cause stroke so easily. There is a possibility that the cardiac thrombi does not result in stroke so easily. But in some cases, that the cardiac thrombi will evoke stroke is certain.
This study has shown 64-MDCT to be reliable for the detection of PVT and the LA thrombus.
Learning points.
The 64-multidetector CT (64-MDCT) is reliable for the detection of the pulmonary vein thrombi (PVT) and left atrium (LA) thrombi.
If small LA thrombus is suspected on transthoracic echocardiography (TTE), then 64-MDCT may certify it.
There is a possibility that PVT and the small LA thrombus are not rare.
The relationship between the cardiac thrombus and cardioembolic stroke is unclear.
64-MDCT is superior to TTE for depicting the thrombi within not only the pulmonary vein but LA and can therefore potentially contribute in identifying the LA thrombus.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Hankey GJ, Warlow CP. Treatment and secondary prevention of stroke: evidence, costs, and effects on individuals and populations. Lancet 1999;2013:1457–63 [DOI] [PubMed] [Google Scholar]
- 2.Takeuchi H. A thrombus of the right upper pulmonary vein: detection by the use of a 64-MDCT. BMJ Case Rep Published 14 Sept 2012. doi:10.1136/bcr.12.2011.5446 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Takeuchi H. 64-MDCT showed the thrombus in the pulmonary vein of the patient with angina pectoris. BMJ Case Rep Published 13 Oct 2012. doi:10.1136/bcr.02.2012.5839 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Takeuchi H. Warfarin improved CT values of the coronary artery artherosclerotic plaque: evaluation by 64-MDCTA. BMJ Case Rep Published 24 Sept 2012. doi:10.1136/bcr.02.2012.5941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hart RG, Pearce LA, Rothbart RM, et al. Stroke with intermittent atrial fibrillation: incidence and predictors during aspirin therapy, J Am Coll Cardiol 2000;2013:183–7 [DOI] [PubMed] [Google Scholar]