

Abstract
Idiopathic external root resorption is a rarely reported condition which has been observed in single or multiple teeth. This is a rare case of multiple idiopathic apical root resorption (MIARR) in a 16-year-old boy. External root resorption of the permanent teeth is a multifactorial process. Well-recognised causes of apical root resorption in permanent teeth include orthodontic therapy, trauma, periapical or periodontal inflammation, tumours, cysts, occlusal stresses, impacted teeth, systemic conditions, endocrine imbalances and dietary habits. When none of these causes are present, it is termed idiopathic root resorption which may be either cervical or apical. MIARR is a rare condition which is usually detected as an incidental radiographic finding. However, it may cause pain and mobility in severe cases.
Background
Idiopathic external root resorption is a rarely reported condition which has been observed either in single or in multiple teeth. Pathological root resorption is related to several local and systemic factors. Orthodontic therapy, trauma, periapical or periodontal inflammation, tumours, cysts, occlusal stresses, impacted and supernumerary teeth, transplantation and reimplantation of teeth are among the local causes that could lead to pathological root resorption.1 Hyperparathyroidism, hypoparathyroidism, hyperphosphataemia, hypophosphataemia, Gaucher's disease, Paget's disease of the bone, Goltz syndrome, Papillon-Lefèvre syndrome, anachoresis, Turner's syndrome as well as dietary habits have been reported as related endocrine disturbances and systemic causes.2
By definition, if an aetiological factor cannot be identified for root resorption, the term ‘idiopathic’ is applied. It should be differentiated from the pathological type and merits to be recognised by a clinician. The most common clinical feature of idiopathic root resorption is that patients are asymptomatic with an occasional complaint of tooth mobility. Resorptive defects are generally coincidentally found after routine radiographic examination.
Two types of idiopathic root resorption have been observed, namely, apical and cervical. Cervical root resorption starts in the cervical areas of the teeth and progresses towards the pulp. In the apical type, the resorption starts apically and progresses coronally causing a gradual shortening and rounding of the remaining root.1
Patients with idiopathic root resorption are commonly asymptomatic clinically with an occasional complaint of tooth mobility; hence, the condition is usually found in routine radiographic examination.3 According to literature review by Cholia et al, the idiopathic apical root resorptions were slightly more common in the upper jaw and molar region than in the lower jaw and single root teeth; however, these differences were not statistically significant. Resorption was also more frequent in men aged between 14–39 years.4
Minimal apical external root resorption may be present in all permanent teeth5 and has been attributed to a variety of causes. However, to date only numerated cases of idiopathic apical root resorption have been reported in the literature. This article describes a case of idiopathic apical root resorption in which no cause could be identified or any reason determined for its occurrence.
Case presentation
A 16-year-old healthy and normally developed Indian boy visited the dental department with a complaint of pain in the right upper back tooth region since 15 days. Clinical intraoral examination revealed a full permanent dentition, tooth 16 was grossly carious and tooth 17 showed a pinkish hue (figure 1). The soft tissues appeared normal. The supragingival calculus and extrinsic stains were present.
Figure 1.

Intraoral photograph.
Multiple apical root resorption was found accidentally on the panoramic view in teeth 14, 15 and 17 (figure 2) and diagnosis was confirmed by the findings on the periapical radiograph (figure 3). The pattern of resorption was blunt and appeared to progress cervically. Regarding the periodontal status, no bone loss was detected. There was no history of trauma, hospitalisation or drug intake, endocrine and systemic disease. The family history of early tooth loss was not reported.
Figure 2.

Panoramic radiograph.
Figure 3.
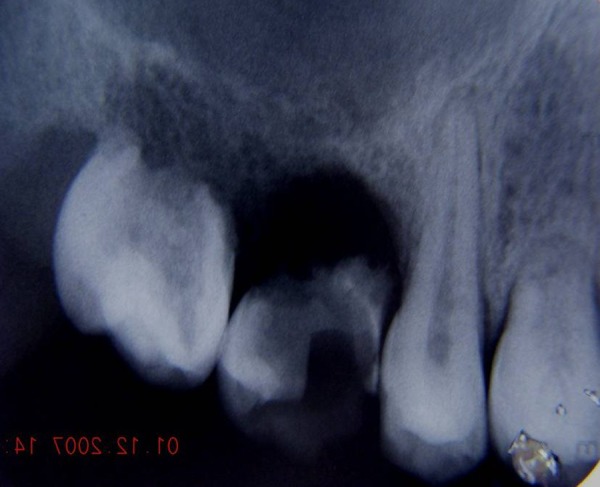
Periapical radiograph.
There was no history of orthodontic therapy and occlusion demonstrated class I molar and class I canine relationship with normal overjet and overbite. No occlusal interferences or detectable tooth mobility was found.
The teeth 14 and 15 showed no response to both electrical and heat pulp tester. Percussion and palpation were unremarkable.
Investigations
Intraoral periapical radiograph
Orthopantomogram
Differential diagnosis
Haematological investigations were within the normal range, so endocrine diseases such as hyperparathyroidism, hypoparathyroidism, hypophosphataemia, hyperphosphataemia and Paget's disease were ruled out. Since abdominal ultrasonography was unfruitful, possibility of Gaucher's disease was eliminated. In Papillon-Lefevre syndrome, the history of premature tooth loss associated with palmar-–plantar hyperkeratosis is remarkable, of which none of them were recognised in the patient. Furthermore, Turner's syndrome is exclusive to women.
Based on history, clinical examination and radiographic findings, a diagnosis of multiple idiopathic apical root resorption (MIARR) was made.
Outcome and follow-up
The patient was asked to follow proper oral hygiene instructions and periodic follow-up was suggested.
Discussion
Few cases of MIARR are reported in the literature. The first well-documented report was in 1930.6 With no absolute aetiological factor identified, we considered this case as MIARR. There was no periodontal or periapical inflammation. Resorption was found incidentally in the panoramic view. No local aetiological factor was detected and clinical appearance of the teeth and periodontium were normal.
Regarding the number of affected teeth in the literature review which were about 18 on average, in this case only three teeth were involved. It may be related to the age of the patient compared with other reported cases. The average reported age was 23.2 years.2 The present case was among a few cases that were under 21years old at the time of detection. The condition has been reported to have a predilection for young women7 and 14 cases of MIARR have been presented in women till now,8 but some published papers reported a predilection of idiopathic root resorption for men.1 2
In an attempt to rule out the possible role of genetics as an aetiological factor, panoramic radiographs of the patient's parents and siblings were obtained which were inconclusive. Laboratory test results indicated no abnormality. Differentiated blood count, calcium, phosphorus and alkaline phosphatase were within the normal range. Owing to the limited number of involved teeth and lack of clinical discomfort in the related tooth, no treatment was advised. Thus, there was no chance for histological and bacteriological analysis in this case.
Schatzle et al reported a case of progressive generalised apical root resorption in a 17-year-old girl. They extracted three involved teeth, histological examination was provided. It showed thickening of cementum layer and accelerated deposition of cellular cementum which normally covered the apical half of the root and furcation. So they diagnosed it as early generalised hypercementosis.1 McMullin9 reported three cases of idiopathic generalised apical root resorption. Reported cases had class II or III malocclusion and one had Down's syndrome. Sogur reported an excessive production of bone surrounding absorbed roots as a compensatory response to osteoclastic activity which had not been seen in previous cases. They also reported a tapering pattern of resorption.10 Treatment usually consists of observation and finally extraction of teeth in advanced lesions. Although the complete root resorption was found in tooth 16 and extraction was planned, due to the presence of the carious lesion we did not consider it as an idiopathic process.
However, root resorption of teeth 14, 15 and 17 cannot be explained by any cause as there were no external forces due to the absence of tooth bud of 18, no history of orthodontic treatment and no history of previous trauma.
Learning points.
Apical root resorption of multiple teeth can be related to no specific aetiology and is known as idiopathic apical root resorption.
Significant idiopathic resorption may present as an accidental radiographic finding, pain or excessive mobility.
It is mostly seen in young adult men; maxillary teeth are more frequently involved.
No preventive or therapeutic regimen is known and monitoring accompanied by periodontal maintenance is recommended.
The prognosis for affected teeth is often poor.
Definitive prosthetic rehabilitation is often best deferred until adulthood due to the potential for further resorption during adolescence in addition to vertical growth considerations.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Aren Schätzle M, Tanner SD, Bosshardt DD. Progressive, generalized, apical idiopathic root resorption and hypercementosis. J Periodontol 2005;2013:2002–11 [DOI] [PubMed] [Google Scholar]
- 2.Moazami F, Karami B. Multiple idiopathic apical root resorption: a case report. Int Endod J 2007;2013:573–8 [DOI] [PubMed] [Google Scholar]
- 3.Rivera EM, Walton RE. Extensive idiopathic apical root resorption. A case report. Oral Surg Oral Med Oral Pathol 1994;2013:673–7 [DOI] [PubMed] [Google Scholar]
- 4.Aldred Cholia SS, Wilson PH, Makdissi J. Multiple idiopathic external apical root resorption: report of four cases. Dentomaxillofac Radiol 2005;2013:240–6 [DOI] [PubMed] [Google Scholar]
- 5.Henry JL, Weinmann JP. The pattern of resorption and repair of human cementum. J Am Dent Assoc 1951;2013:270–90 [DOI] [PubMed] [Google Scholar]
- 6.Mueller E, Rony HR. Laboratory studies of unusual cases of resorption. J Am Dent Assoc 1930;2013:326–34 [Google Scholar]
- 7.Kerr DA, Courtney RM, Burkes EJ. Multiple idiopathic root resorption. Oral Surg Oral Med Oral Pathol 1970;2013:552–65 [DOI] [PubMed] [Google Scholar]
- 8.Gupta R, Prakash V. Bilateral extensive idiopathic apical root resorption in supraerupted maxillary molars: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;2013:44–7 [DOI] [PubMed] [Google Scholar]
- 9.McMullin A, Fleming PS, Dibiase AT. Idiopathic generalized apical root resorption: a report of three cases. Int J Paediatr Dent 2008;2013:312–16 [DOI] [PubMed] [Google Scholar]
- 10.Soğur E, Soğur HD, Baksi, et al. Idiopathic root resorption of the entire permanent dentition: systematic review and report of a case. Dent Traumatol 2008;2013:490–5 [DOI] [PubMed] [Google Scholar]