

Abstract
A 45-year-old man presented with a left-sided pneumothorax following an episode of forceful vomiting. His chest drain revealed biliary contents and his CT chest with oral contrast confirmed the diagnosis of oesophageal rupture. He was transferred for surgical repair to a tertiary centre. Biliary contents within a chest tube are an important clinical finding and should raise suspicion of Boerhaave's syndrome. Any delays should be avoided due to the high mortality.
Description
A 45-year-old man presented with severe shortness of breath, abdominal pain and chest pain following an episode of vomiting. He had a medical history of hypertension and he was only taking antihypertensive medications.
On examination, he was in respiratory distress with the use of accessory muscles tachypnoeic and hypoxic on air. He had absent breath sounds and hyper-resonance on the left. A chest drain was inserted and dark fluid mixed with blood was seen in the chest tube (figure 1). A CT chest with oral contrast was performed which confirmed the diagnosis of oesophageal rupture of the posterolateral lower third of oesophagus on the left side (figure 2).
Figure 1.

Biliary contents in the chest tube.
Figure 2.
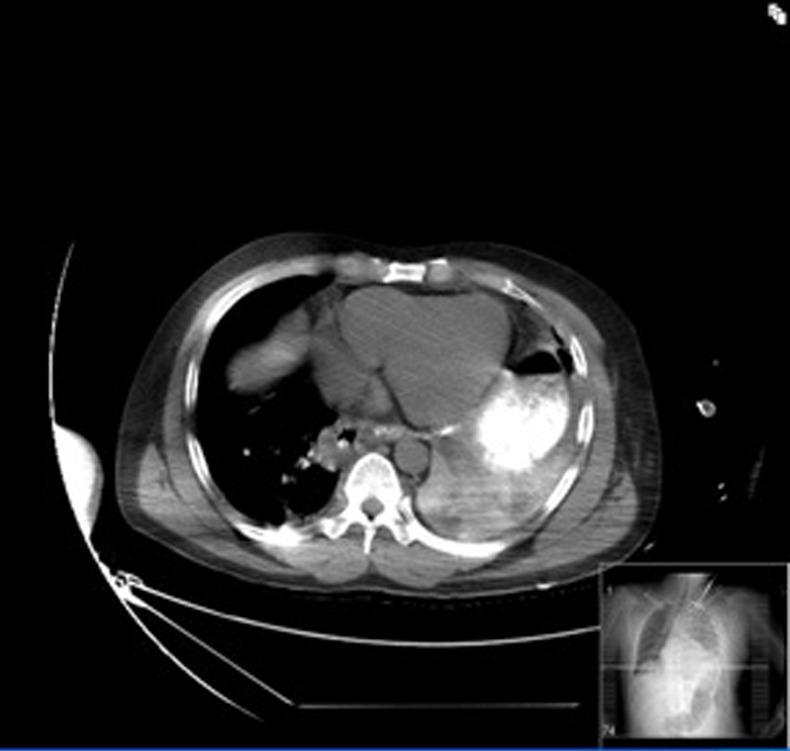
CT chest with oral contrast at the level of gastroesophageal junction demonstrating a contrast leak into the left pleural space thought a tear of the left posteromedial site of the oesophagus.
He was transferred to a tertiary centre for surgery.
The finding of biliary and food contents within the chest drain is highly suggestive of oesophageal rupture and this should not delay treatment as the mortality is up to 31% and this is mainly due to mediastinitis and sepsis.1
The classic Mackler's triad of subcutaneous emphesema, vomiting and chest pain is highly suggestive of the disease, but is only present in a minority of cases.
Learning points.
Beware of the breathless patient after severe vomiting. Oesophageal rupture is rare, but lethal disease.
Finding of biliary contents on the chest drain should initiate the process of referring to a tertiary centre without awaiting for CT and report as any delay has direct impact on the mortality.
The insertion of nasogastric tube is contraindicated in this case due to the potential risk of damage to mediastinal structures.
Footnotes
Contributors : GAD and MSN looked after the patient and reviewed the manuscript. GAD was the main author.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
Reference
- 1.Brauer RB, Liebermann-Meffert D, Stein HJ, et al. Boerhaave’s syndrome: analysis of the literature and report of 18 new cases. Dis Esophagus 1997;2013:64–8 [DOI] [PubMed] [Google Scholar]