

TO THE EDITOR: The pathogenesis of microtia, a rare congenital malformation of the external ear, remains elusive. Phenotypes range from minor deformities, such as preauricular tags, to anotia, the complete absence of the external ear (Fig. 1). Prevalence ranges from 0.66 per 10,000 in England to 17.4 per 10,000 in Quito, Ecuador.1 The relative contributions of environmental and genetic factors to microtia were assessed in a classic twin study.
Figure 1. Normal and Malformed Ears in One Pair of Monozygotic Twins.
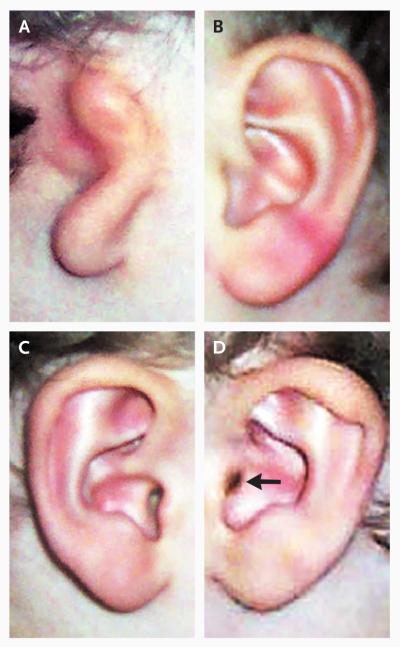
In Twin 1, the right ear shows severe microtia and aural atresia (Panel A), whereas the left ear is unaffected (Panel B). In Twin 2 the right ear is unaffected (Panel C), whereas the left ear (Panel D) shows mild microtia, consisting of a stenotic external ear canal (arrow) and a constricted helix.
In this study, we identified 13 monozygotic and 22 dizygotic twin pairs at three microtia reconstruction centers, one in the United States, one in Ecuador, and one in Colombia. In other words, each twin pair was ascertained because at least one sibling had severe nonsyndromic microtia requiring surgical repair. There was no ear malformation in 40% of subjects, malformation of the right ear in 34%, malformation of the left ear in 13%, and bilateral anomalies in 12%. Ear-malformation laterality was indistinguishable among monozygotic and dizygotic twins. None of the twins reported first-degree relatives with ear malformations, but 20% had at least one, more distant relative with an ear malformation.
The concordance rate for all auricular malformations was higher in monozygotic twins than in dizygotic twins (61.5% and 4.5%, respectively; P = 0.003) (Table 1). Concordance rates for microtia (excluding skin tags and minor pinna malformation) among monozygotic and dizygotic twins were also significantly different – 38.5% and 4.5%, respectively (Table 1).
Table 1.
Concordance and Discordance of Ear Malformations in Monozygotic and Dizygotic Twins.*
| Ear Malformation | Concordant | Discordant | Odds Ratio (95% CI) |
P Value |
|---|---|---|---|---|
| All | 33.4 (3.3–340.3) |
0.003 | ||
| Monozygotic | 8 | 5 | ||
| Dizygotic | 1 | 21 | ||
| Microtia | 12.6 (1.3–122.7) |
0.029 | ||
| Monozygotic | 5 | 8 | ||
| Dizygotic | 1 | 21 |
Twin pairs classified on the basis of all ear malformations (e.g., skin tags, clefts, and microtia) and microtia only were stratified according to zygosity. Zygosity was confirmed when it was determined that the twins were of the same sex with the use of 17 high-heterozygosity microsatellite markers. P values were calculated for association between zygosity and outcome with the use of logistic-regression models, adjusted for correlation among pairs from the same family. CI denotes confidence interval.
A literature review identified 37 twin pairs with microtia in whom other auricular malformations were rarely reported.2-5 When the results of this study are combined with those of our study of 35 twin pairs, the 72 sets of twins show significant differences in the concordance rate for monozygotic twins (10 in 38, or 26.3%), and the concordance rate for dizygotic twins (1 in 34, or 2.9%) (odds ratio, 11.5; 95% confidence interval, 1.4 to 93.7; P = 0.023).
In summary, twin studies indicate that there is a strong genetic contribution to malformations of the external ear. Shared genotype in monozygotic twins increased the risk of auricular malformations by a factor of about 30. Environment also to the risk of contributes auricular malformations, accounting for discordance in 40% of monozygotic twins.
Our data are consistent with two models. A concordance of 60% in monozygotic twins is consistent with a germ-line mutation that is incompletely penetrant. Alternatively, microtia may result from somatic mutations or epigenetic events that occur early in embryogenesis, since monozygotic twins separate by the 12th day after fertilization.
Acknowledgments
Supported by grants from the National Institutes of Health (R01 DC007453, to Drs. C. Seidman and J. Seidman; and UL1-RR025758, to Dr. Betensky), the Eavey Young Investigators Fund of the Massachusetts Eye and Ear Infirmary, Boston (to Dr. Eavey), and the International Fellowship of the American Association of University Women (to Dr. Artunduaga).
Contributor Information
Maria A. Artunduaga, Harvard Medical School Boston, MA
Maria D.L. Quintanilla-Dieck, Harvard Medical School Boston, MA
Steven Greenway, Harvard Medical School Boston, MA
Rebecca Betensky, Harvard School of Public Health Boston, MA
Yamileth Nicolau, University of California School of Medicine San Diego, CA
Usama Hamdan, Global Smile Foundation Lexington, MA
Patricia Jarrin, Fundación Tierra Nueva Quito, Ecuador
Gabriel Osorno, National University of Colombia School of Medicine Bogotá, Colombia
Burt Brent, El Camino Hospital Mountain View, CA
Roland Eavey, Vanderbilt University School of Medicine Nashville, TN
Christine Seidman, Howard Hughes Medical Institute Boston, MA
J.G. Seidman, Harvard Medical School Boston, MA seidman@genetics.med.harvard.edu
References
- 1.Alasti F, Van Camp G. Genetics of microtia and associated syndromes. J Med Genet. 2009;46:361–9. doi: 10.1136/jmg.2008.062158. [DOI] [PubMed] [Google Scholar]
- 2.Neal GS, Hankins GD. Left microtia in one monozygotic twin: a case report. J Reprod Med. 1992;37:375–7. [PubMed] [Google Scholar]
- 3.Hussain M, Ball EA, Moss AL. Ipsilateral microtia in monozygotic twins: an unusual concordant phenotype. Plast Reconstr Surg. 2004;113:1293–4. doi: 10.1097/01.prs.0000110861.47621.45. [DOI] [PubMed] [Google Scholar]
- 4.Wieczorek D, Ludwig M, Boehringer S, Jongbloet PH, Gillessen-Kaesbach G, Horsthemke B. Reproduction abnormalities and twin pregnancies in parents of sporadic patients with oculoauriculo-vertebral spectrum/Goldenhar syndrome. Hum Genet. 2007;121:369–76. doi: 10.1007/s00439-007-0336-0. [DOI] [PubMed] [Google Scholar]
- 5.Digilio MC, Calzolari F, Capolino R, et al. Congenital heart defects in patients with oculo-auriculo-vertebral spectrum (Goldenhar syndrome) Am J Med Genet A. 2008;146A:1815–9. doi: 10.1002/ajmg.a.32407. [DOI] [PubMed] [Google Scholar]