

Abstract
Distasis recti is a common occurrence in multiparous women (1), caused by repeated stretching of the abdominal wall by the gravid uterus. A small proportion of patients have a persisting weakness which may be symptomatic and present to the surgeon. We would like to present a case which, thus far, has had a successful outcome from laparoscopic plication of the linea alba without mesh. The benefits of this approach are as for any laparoscopic versus open technique, most notably improved recovery time, reduced pain and wound infection. Furthermore, avoidance of a mesh negates the risks associated with insertion of a foreign body.
INTRODUCTION
Laparoscopic repair of diastasis recti has seldom been described in the literature (2) and to our knowledge, never without the use of a mesh. Cosmesis is usually the primary concern of patients but other symptoms include discomfort, nausea as well as an increased risk of developing a midline or paraumbilical hernia (3). There is no current national guidance on the treatment of diastasis recti.
CASE REPORT
A slim 38 year old Caucasian female presented to surgical outpatients clinic with principal concerns of discomfort and difficulty picking up and holding her young child due to a bulge in her upper abdomen. Further history elicited a total of three pregnancies and a physically active lifestyle. She was found to have diastasis recti clinically, extending from the midpoint of the xiphoid process and the umbilicus to the supra-umbilical region. The patient was 18 months post-partum and expressed a wish to have the weakness corrected surgically. A decision to pursue this laparoscopically was made as it was felt that spontaneous resolution was unlikely.
Following routine pre-operative preparation, the patient was placed in the Lloyd-Davies position to allow operator access. A 10 mm port was placed in the supra-pubic region via a modified Hassan approach and a 5 mm port was placed in each iliac fossa. Interrupted nylon horizontal mattress sutures were fixed at approximately 2 cm either side of the midline along the length of the diastasis recti. Reduction in the divarication was confirmed intra-operatively by manual pressure on the anterior abdominal wall. No mesh was inserted.
Fig 1.
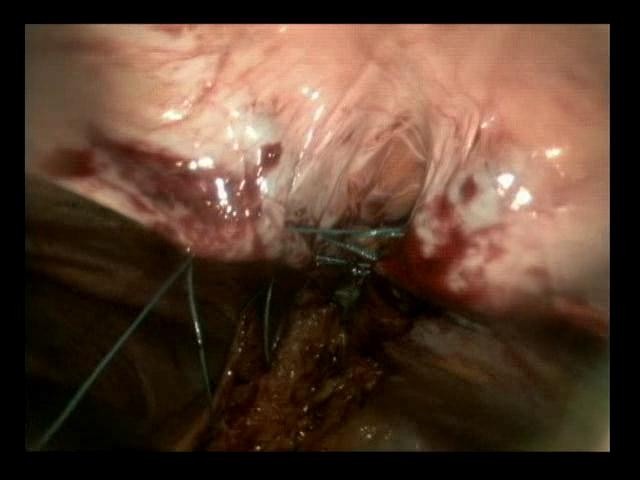
Insertion of horizontal mattress sutures
Fig 2.

Sutures along length of diastasis
Fig 3.

Completed plication
Post-operatively, the patient made good but slow progress and was discharged on day 5. Primary reasons for delay included difficulties in controlling pain and waiting for resolution of an ileus.
Eight weeks following discharge, the patient was reviewed in outpatient clinic and reported an improvement in both appearance and symptoms. There was no evidence of herniation on examination.
DISCUSSION
Operative repair for diastasis recti is controversial (3,4). Consequently, there are few studies assessing the effectiveness of surgical intervention. Reports on laparoscopic repair, however, are rarer still and it is usually the patients themselves who request treatment.
This case demonstrates how symptomatic and concerned patients may benefit from this simple approach to provide a good cosmetic and functional result. The avoidance of a mesh reduces the risk of infection, adhesions and chronic pain as well as operative and anaesthesia time. We hypothesise the outcome will be similar to the published data on cases where mesh was also inserted. However, long-term follow up and the development of a case series is necessary to ensure potential complications are identified and results validated.
REFERENCES
- 1.Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther 1988; 68: 1082–1086 [DOI] [PubMed] [Google Scholar]
- 2.Palanivelu C, Rangarajan M, Jategaonkar PA, Amar V, Gokul KS, Srikanth B. Laparoscopic repair of diastasis recti using the ‘Venetian blinds’ technique of plication with prosthetic reinforcement: a retrospective study. Hernia. 2009. Jun; 13(3): 287–92 [DOI] [PubMed] [Google Scholar]
- 3.Nahas FX, Augusto SM, Ghelfond C. Should diastasis recti be corrected? Aesthetic Plast Surg. 1997. Jul-Aug; 21(4): 285–9 [DOI] [PubMed] [Google Scholar]
- 4.Lockwood T. Rectus muscle diastasis in males: primary indication for endoscopically assisted abdominoplasty. Plast Reconstr Surg 1998; 101: 1685–1691 [DOI] [PubMed] [Google Scholar]