

Abstract
Acute appendicitis, as well as intestinal obstruction, is a common surgical emergencies. Both the conditions can present as an acute abdomen, however the diagnosis of acute appendicitis can be overlooked when it presents as a small bowel obstruction. Difficulties in correctly identifying the cause of pain can be hazardous to the patient and care needs to be taken in obtaining a prompt and accurate diagnosis enabling the most appropriate management. Appendiceal duplication although rare and difficult to diagnose preoperatively, should be checked while operating for appendicular pathology in order to avoid serious clinical and medicolegal implications.
We hereby report a case of appendiceal duplication presenting as small bowel obstruction with one appendix having acute appendicitis and the other one perforated in the middle third.
INTRODUCTION
The appendix is an out-pouching from the caecum, and is often called the abdominal tonsil due to the presence of lymphoid follicles. The appendix is usually present singlely with the base located at the convergence of taeniae along inferior aspect of the ceacum while its tip lies at various locations. Appendiceal anomalies although rare include agenesis, duplication, triplication and anomalously located solitary appendix. About 8% of western population have inflammation of appendix during their lifetime, this makes acute appendicitis the most common general surgical emergency.
Acute appendicitis can present in a various manners, one rare form being small bowel obstruction. We are reporting a unique case of acute appendicitis having appendiceal duplication, presenting as small bowel obstruction.
CASE PRESENTATION
A 40 year old male was admitted to our emergency department as a case of pain in the abdomen for 6 days. The nature of the pain was colicky, diffuse and was associated with constipation. This was followed by abdominal distension, anorexia and nausea. A detailed history was sought. Patient had no history of prior abdominal surgery, loss of weight, bleeding with stools or intake of any medication. Past medical and surgical histories were unremarkable. On examination, he was found to have a blood pressure of 120/80, pulse rate of 106 beats/min, and had a temperature of 1010 F. Abdominal examination revealed abdominal distension, lower abdominal guarding more so in the right iliac fossa with rebound tenderness and increased bowel sounds. Abdominal roentograms in supine and standing positions showed multiple small bowel air fluid levels. His abdominal ultrasonography scans revealed multiple dilated loops of small bowel with free fluid in pelvis and paracaecally. A preliminary diagnosis of small bowel obstruction with possibility of intestinal gangrene was made.
Because of the uncertinity of the diagnosis an exploratory laparotomy was performed through a right paramedian incision under emergency settings. Surprisingly two ceacal appendices were noted, the tip of one was pre-ileal having gross inflammation with its base on the anterior most tenia coli and the tip across the terminal most part of cecum with multiple adhesions kinking the bowel. The tip of the other appendix was retrocaecal having a perforation in the middle third with its base at the confluence of the tenia. The distance between the two bases was approximately four centimeters (Fig.1 and Fig. 2). About 200ml of foul smelling frank pus was present in the paracaecal recess and pelvis. Small intestine loops were grossly dilated.
Figure 1.
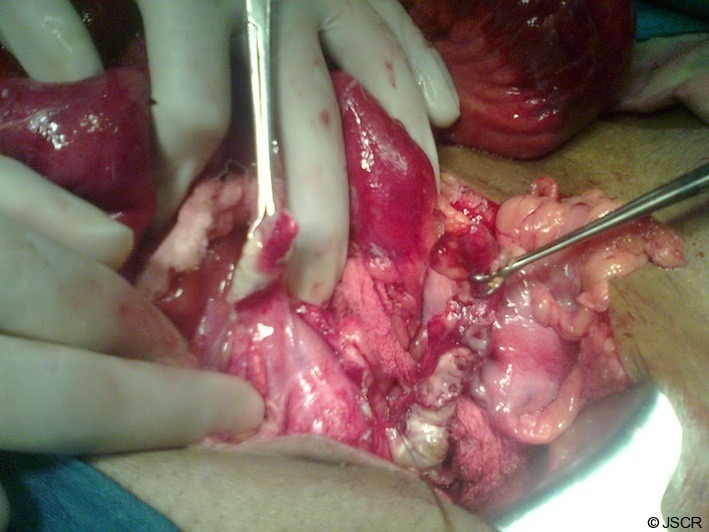
Intra-operative picture of two inflamed appendices
Figure 2.
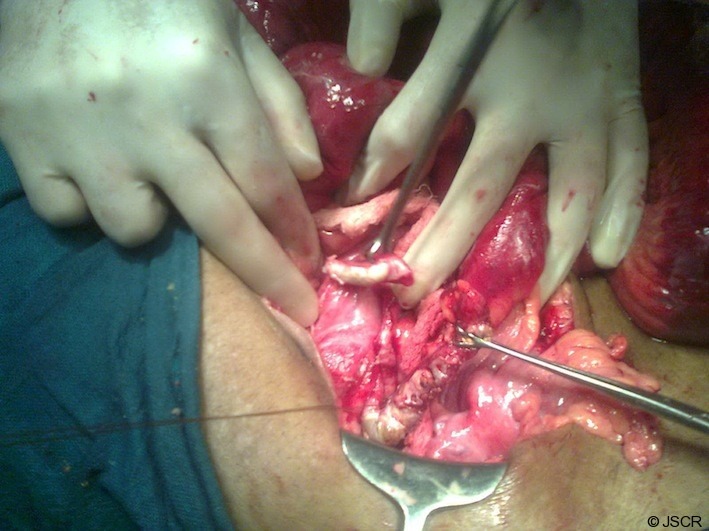
Intra-operative picture of two inflamed appendices
The adhesiolysis and appendectomies were duly done and generous isotonic saline washes were performed. The distended bowel was decompressed by milking the contents in the large bowel. A tube drain was kept in the pelvis. The patients post operative period was uneventful and he was discharged after 4 days of hospital stay. The histopathology analysis revealed acute appendicitis for the pre-ileal appendix and gangrene of the retroceacal appendix. The patient is on a regular follow-up and is doing well.
DISCUSSION
Appendiceal anomalies have been reported on numerous occasions. These include agenesis, duplication, triplication, anomalously located solitary appendix and the more recently described horseshoe appendix(1). They are thought to result due to the persistence of normally transient embryologic second caecal appendix. Collins could find only 2 such cases in 50000 appendices(2). To date less than 100 cases of appendiceal duplication in which two appendices are present have been reported(3). A single case of appendiceal triplication has been reported till now along with a 0.004% incidence of appendiceal duplication(4), thereby concluding that appendiceal anomalies are rare. Cave in 1936 devised the first system classifying appendiceal duplication(5). Later on it was further modified by Wallbridge in 1963(6). Biermann in 1993(7) proposed the following classification
| Type A | A single ceacum with various degrees of partial duplication. |
| Type B1 | The 2 appendices are symmetrically placed on either side of the ileocecal valve. |
| Type B2 | One appendix arises from the ceacum at the usual site and a second appendix branches from the ceacum along the lines of the taenia at various distances from the first. |
| Type C | A double ceacum each with an appendix on each ceacum. |
Type B and C can have associated genitourinary and gastrointestinal anomalies.(8)
Acute appendicitis is also known to be a rare cause of mechanical small bowel obstruction(9), usually resulting from adhesions due to periappendicular inflammation and is different from ileus seen in patients having perforated appendicitis presenting with generalized or localized peritonitis. Inspite of previous reports, such a presentation of acute appendicitis is not recognized widely, which may cause delays in diagnosis and management. Thereby resulting in an increased chance of post operative and long term complications.
Harris et al (10) in a series of 10 cases of appendicitis with gangrene, necrosis or perforation reported that the most common cause of the mechanical bowel obstruction was an appendix that lay across the terminal ileum with adhesive bands holding it down. He concluded that very often the differentiation between adynamic ileus and true mechanical obstruction is difficult to elicit clinically.
REFERENCES
- 1.Mesko T. Horseshoe anomaly of the appendix: A previously undescribed entity. Surgery 1989,563–66 [PubMed] [Google Scholar]
- 2.Collins D. A study of 50,000 specimens of the human veriform appendix. Surgical Gynecological Obstetrics 1955;101:437–46 [PubMed] [Google Scholar]
- 3.Bluett M, Halter S, Salhany K. Duplication of the appendix mimicking adenocarcinoma of the colon. Archives of Surgery 1987;122:817–20 [DOI] [PubMed] [Google Scholar]
- 4.Kjossev KT, Losanoff JE. Duplicated vermiform appendix. British Journal of Surgery 1996;83:1259. [PubMed] [Google Scholar]
- 5.Cave AJE. Appendix vermiformis duplex. Journal of Anatomy 1936;70:283–92 [PMC free article] [PubMed] [Google Scholar]
- 6.Wallbridge PH. Double appendix. British Journal of Surgery 1963;50:346–47 [DOI] [PubMed] [Google Scholar]
- 7.Biermann R. Appendix duplex. Eine Pathologische Raritat 1993;64:1059–61 [PubMed] [Google Scholar]
- 8.Mitchell IC, Nicholls JC. Duplication of the vermiform appendix. Report of a case: Review of the classification and medicolegal aspects. Medicine, Science, Law 1990;30(2):124–26 [DOI] [PubMed] [Google Scholar]
- 9.Gupta S, Vaidya M: Mechanical small bowel obstruction cased by acute appendicitis. The American Surgeon 1969, 35(9):670–674 [PubMed] [Google Scholar]
- 10.Harris S, Rudolf L: Mechanical small bowel obstruction due to acute appendicitis. Annals of Surgery 1966, 164(1):157–161 [DOI] [PMC free article] [PubMed] [Google Scholar]