

Abstract
Acute lateral patellar dislocation is relatively common in younger age group and most likely caused by indirect trauma. About 10% of acute patella dislocations are the result of a direct blow to the medial side. We report a case of irreducible lateral patellar dislocation which is of exceptional interest in that lateral patellar dislocation (extra-articular) occurred in comparatively older age group with arthritic knee, there was no direct trauma involved and it was associated with some rotation along long axis, impaction of patella on lateral femoral condyle and was locked underneath osteophytic ridge of lateral femoral condyle, which needed open reduction. This is a very rare injury, first of its kind being reported in Australia.
INTRODUCTION
Orthopaedic professionals usually never have the fortune to perform the good office of reduction of patella (1–3). Most of patella dislocations are spontaneously reduced and others are reduced easily in emergency department (3,4). Irreducible patellar dislocations are rare injuries, but those that do occur are mainly directed intra-articular (7). We report an exceptionally interesting case of an extra-articular irreducible lateral patella dislocation.
CASE REPORT
A 50-year-old gentleman was brought into Emergency with an inability to walk after a fall while walking down hill. Past history did not reveal any predisposing factors for patella dislocation. Examination revealed obvious laterally dislocated patella with tenting of the anterolateral skin. (Figure 1)
Fig. 1.

Lateral dislocation of patella with rotation and obvious tenting of skin
His knee was locked in full extension (unlike some flexion associated with lateral patellar dislocation) (6,8). The patella was rotated about the long axis with the smooth articular surface facing posterolaterally. It was locked under the outer edge of the lateral femoral condyle. Imaging studies confirmed the clinical findings and also revealed a minor impaction fracture of lateral femoral condyle with arthritic changes in the knee joint (Figure 2).
Fig. 2.

Imaging studies showing lateral dislocation of patella with rotation about long axis, patella locked onto lateral femoral condyle; and insignificant impaction fracture of lateral femoral condyle
We attempted closed reduction under sedation and relaxation. We tried to unlock the patella and push it medially while keeping the knee in full extension and the hip in flexion (to relax the quadriceps). We also attempted to flex the knee fully to reduce the patella from the unnatural position, as mentioned in literature (8,9). All attempts were futile and the patella was immovable. The patient was taken to theatre, keeping in mind the possible need for open reduction. Under general anaesthetic and muscle relaxation, closed reduction was attempted without success. After appropriate preparation of skin and draping, a bone hook and tinaculum were used to apply traction and attempts were made to slide the patella over the prominent lateral femoral condyle, which was of no avail (3). We performed an open reduction through a medial para-patellar approach. There was a large longitudinal tear in the medial retinaculum (Figure 3) with avulsion of attachments from medial border of patella.
Fig. 3.

Intra-operative photograph (before reduction) – tear of medial retinaculum with avulsion of medial attachments of patella
The patella was rotated about 70-80 degrees with the articular surface facing outwards. The medial border of the patella was hooked on the outer surface of the lateral femoral condyle under the prominent osteophytic ridge. The patella was pulled laterally and a wide periosteum elevator was inserted as a skid between the medial border of the patella and the lateral femoral condyle to unlock the patella from under the osteophytic ridge of the lateral femoral condyle. It was slipped over the lateral femoral condyle with a periosteum elevator. As soon as patella cleared lateral femoral condyle, it flipped back into normal position. We found a small insignificant impaction fracture on the lateral femoral condyle with a prominent osteophytic ridge (like a shelf), which was probably a contributing factor for the patella being locked and irreducible (in addition to rotation along long axis). Medial structures were repaired. The knee was placed in a Richard's splint in extension for two weeks while allowing him to touch weight bearing. Post-operative radiographs revealed normal patello-femoral articulation. At two weeks, gradual ROM (Range of motion) was started in ROM brace with quadriceps strengthening exercises. He achieved pain-free full active ROM by six weeks without any residual instability of patella.
DISCUSSION
Since the first description by Cooper in 1844 (8), there have been only a few similar cases reported in orthopaedic literature. From the literature, it is apparent that this type of patella dislocation would result from a blow directly on the medial side while the quadriceps is taut (4). This makes the patella ride against the prominent lateral femoral condyle (which acts as a safeguard to prevent lateral displacement of the patella) creating torque resulting in rotation of the patella around the longitudinal axis. If this force continues to act, it will push the patella beyond the margin of the lateral femoral condyle over which its medial edge will be locked (Figure 4). A CT scan is valuable in cases of doubt (2,6).
Fig. 4.
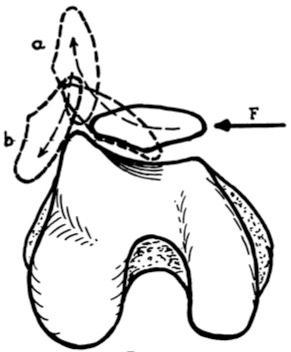
Sketch showing the path patella must take for lateral dislocation with rotation about long axis. (F): direction of dislocating force, (a): position of patella resulting from it sliding up on lateral femoral condyle, (b): final position of patella, where it gets locked, after medial edge clears lateral condyle
It is very natural to assume that any attachments on medial border of patella have to rupture before this kind of dislocation (3). It may be possible, though unlikely, to achieve closed reduction of this type of injury, which may increase the risk of iatrogenic osteochondral lesions (6). We prefer and recommend performing open reduction to have an opportunity to repair medial torn structures. We believe that this will reduce the tendency of lateral dislocation and restore limb (quadriceps) strength to optimum. It also allows inspection of the joint and removal of possible loose cartilage bodies.
References
- 1.Elibrahimi A, Habi S. Lateral patellar dislocation with vertical axis rotation of 90°. American Journal of Emergency Medicine. 2007; 25: 733.e1–733.e2 [DOI] [PubMed] [Google Scholar]
- 2.Michels F, Pouliart N, Oosterlinck D. Locked patellar dislocation – a case report. Journal of Medical Case Reports. 2008; 2: 371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Inman VT, Smart BW. Irreducible lateral dislocation of the patella with rotation: a case report. J Bone Joint Surg Am. 1941;23: 695–700 [Google Scholar]
- 4.Corso J, Thal R, Forman D. Locked patellar dislocation with vertical axis rotation - a case report. Clin Orthop Relat Res. 1992; 279:190–193 [PubMed] [Google Scholar]
- 5.Hackl W, Benedetto KP, Fink C, Sailer R, Rieger M. Locked lateral patellar dislocation: a rare case of irreducible patellar dislocation requiring open reduction. Knee Surg Sports Traumatol Arthrosc. 1999;7:352–355 [DOI] [PubMed] [Google Scholar]
- 6.Feibel RJ, Niloofar D, Cwinn AA. Irreducible lateral patellar dislocation: The importance of impaction fracture recognition. The Journal of Emergency Medicine. 2007; 33: 11–15 [DOI] [PubMed] [Google Scholar]
- 7.Phaltankar PM, Bridl SH. Locked lateral patellar dislocation with impaction fracture of patella. Ann R Coll Surg Engl. 2002; 84: 125–126 [PMC free article] [PubMed] [Google Scholar]
- 8.Cooper A. A treatise on dislocations and fractures of joints. p. 178 Philadelphia: Lea and Blanchard; 1844 [Google Scholar]
- 9.Sanborn EK. Lateral luxation of the patella, of difficult reduction. Boston Med. and Surg. J. 1856; LIV: 175 [Google Scholar]