

Abstract
Bacille Calmette-Guérin (BCG) is an effective treatment for patients with superficial bladder cancer and bladder carcinoma in situ (CIS). It may cause side effects usually due to local and systemic inflammatory effects. We report a case of a male patient with non-invasive urothelial carcinoma of urinary bladder (Stage T1) who developed caseating granulomas on his glans penis as a complication of intravesical BCG immunotherapy. Though there are other reported cases of BCG dissemination noted in the literature, penile granuloma is rare. The first reported case was published in 1992 and since then only eleven cases are reported. It appears that both direct infectious processes and hypersensitivity reactions contribute to the clinical manifestations of a systemic BCG infection. Our case possibly represents a local infection of M bovis involving the glans penis.
Keywords: BCG immunotherapy, penile trauma, penile tuberculosis, urothelial carcinoma
INTRODUCTION
Bacille Calmette-Guérin (BCG), a live attenuated strain of Mycobacterium bovis, is an effective treatment for patients with superficial bladder cancer and bladder carcinoma insitu (CIS). It may cause side effects usually due to local and systemic inflammatory effects of the attenuated tubercle bacillus. Systemic infections with M. bovis have been known to occur, however, in the prostate, blood, liver, kidneys, and lungs of patients undergoing treatment with intravesical BCG.[1] We report the case of a male patient with noninvasive urothelial carcinoma of urinary bladder who developed caseating granulomas on his glans penis as a complication of intravesical BCG immunotherapy.
CASE REPORT
A 62-year-old male patient presented with intermittent hematuria and urgency of urine. Cystoscopic examination revealed a multicentric papillary tumor in the urinary bladder. The patient underwent transurethral resection of bladder tumour (TURBT) followed by immediate instillation of Doxorubicin. Subsequent histopathology showed the features of noninvasive papillary urothelial carcinoma, Grade 1, Stage T1. According to the treatment protocol, this case was considered for intravesical BCG therapy (Strain : D0 anish-1331) at a dose of 120 mg weekly for six weeks. BCG immunotherapy started after 10th post operative day and continued for 6 weeks thereafter. A follow-up cystoscopy was carried out after completion of therapy and found no recurrences of the tumor at that point of time. Approximately two weeks after completion of BCG therapy patient started suffering of mild dysuria. Tender, papular and ulcerated eruptions with mild discharge were noted on the glans penis. The patient was not circumcised. Local examination revealed mildly tender inguinal lymphadenopathy on the right side. Oral Azithromycin at a dose of 500 mg BD was prescribed along with topical antimicrobial agent empirically. But the patient did not respond well. Routine investigation including Chest X-ray, complete blood count (CBC), urine routine and culture and venereal disease research laboratory (VDRL) tests were advised. CBC was within normal range for the age except erythrocyte sedimentation rate, which was strikingly increased to 102 mm at first hour. VDRL test for Syphilis and ELISA for human immunodeficiency virus type 1 and 2 were non reactive. Routine urine examination and culture did not reveal anything. An incisional biopsy performed and tissue was sent to the department of pathology. Histopathological examination showed caseating granuloma under the penile mucosa with ulceration at places. [Figures 1 and 2] Ziehl-Neelsen stain and Periodic acid-Schiff stain did not reveal any organism. Culture for tuberculosis was not done. Anti-tubercular therapy started with two drug regimen comprising 300 mg of isoniazid and 450 mg of rifampicin once daily. Lesions began to heal by the tenth day of therapy. The therapy was continued for six months and lesions were completely healed. The patient was advised to attend OPD for regular follow-up and check cystoscopy.
Figure 1.
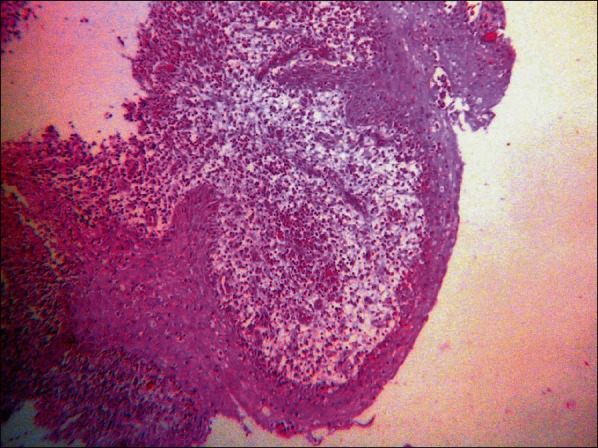
Photomicrograph showing caseating granuloma under the penile squamous mucosa. (H and E Stain, ×100)
Figure 2.
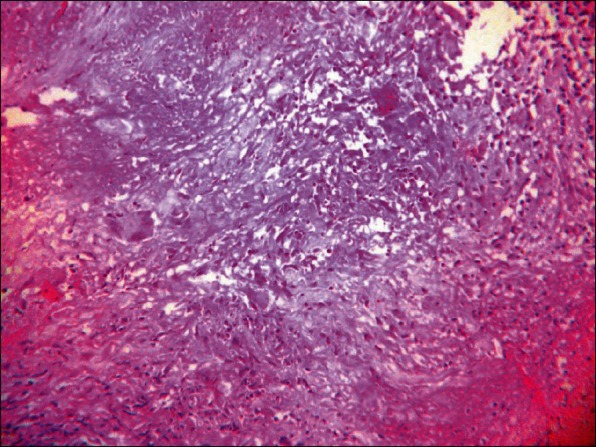
Photomicrograph showing caseating granuloma with langhans' giant cells. (H and E Stain, ×400)
DISCUSSION
BCG intravesical immunotherapy is indicated in the management of residual superficial bladder cancer and urothelial carcinoma-in-situ (CIS) and for prophylaxis of multiple and/or early recurrent bladder tumours. In multiple T1G2 tumors, Ta-T1G3 tumors with or without CIS, and CIS alone, the advantages of intravesical BCG are more pronounced than in intermediate-risk patients, who are at a lower risk of progression.[2] We treated our case with BCG because of the multicentric nature of the lesion. BCG should not be instilled immediately after surgery because of the high rate of systemic complications. Even when there are no contraindications to BCG, side effects are common. The most common side effects are abacterial cystitis and dysuria (80%), hematuria (40%), and low-grade fever. Granulomatous prostatitis is noted in about 1% of patients apart from granulomas that may occur in lung, liver, and bones.[3] However, penile granuloma is very rare. Few cases are enlisted in the literature. The first reported case was published in 1992 and since then only eleven cases are reported.[4]
Christopher G. French et al. reported a case of caseating granuloma on glans penis in a 67-year-old male patient of T1 multiple bladder cancer, which was treated successfully with isoniazid and rifampicin.[5]
Yusuke H, Yoshinori H and colleagues report a rare case of granulomatous balanoposthitis after intravesical BCG instillation therapy in a 58-year-old man, which they treated with single antituberculous agent isoniazid (300 mg/day).[6]
Kureshi F et al. in 2006 reported cutaneous complications of intravesical therapy in two patients with transitional cell carcinoma of the bladder. Both of them were elderly individual and presented with penile granuloma following intravesical BCG therapy. However one patient had to undergo penectomy because of gangrenous complication of the penis.[7] However Sharma et al. used four drug regimen for the treatment of penile tuberculosis in their case.[4]
It may so happen that penile involvement occurs because of the inadvertent trauma caused by the process of catheterization during BCG inoculation or spillage of the BCG containing solution after instillation as postulated by other workers.[4,5] In our case, papules were on the surface of the glans. This suggests that BCG might come in direct contact with the involved area either by inadvertent spillage or from voided urine.
It appears that both direct infectious processes and hypersensitivity reactions contribute to the clinical manifestations of a systemic BCG infection. A granulomatous reaction may occur with either a hypersensitivity mechanism or an infectious process and is not pathognomonic for disseminated infection. Finding of a positive culture of mycobacteria from a distant site is an important indication of disseminated infection.[8]
CONCLUSION
Apart from granulomas occurring in other locations following BCG immunotherapy, penile granulomas are rare one. It may be due to local trauma or hypersensitivity reaction due BCG. Careful instillation of intravesical BCG immunotherapy after specified post operative period can successfully prevent recurrences in urothelial carcinoma as well as its complications.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Lamm DL, van der Meijden PM, Morales A. Incidence and treatment of complications of bacillus Calmette-Guérin intravesical therapy in superficial bladder cancer. J Urol. 1992;147:596–600. doi: 10.1016/s0022-5347(17)37316-0. [DOI] [PubMed] [Google Scholar]
- 2.Babjuk M, Oosterlinck W, Sylvester R, Kaasinen E, Böhle A, Palou-Redorta J. European Association of Urology (EAU). EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder. Eur Urol. 2008;54:303–14. doi: 10.1016/j.eururo.2008.04.051. [DOI] [PubMed] [Google Scholar]
- 3.Rischmann P, Desgrandchamps F, Malavaud B, Chopin DK. BCG intravesical instillations: Recommendations for side-effects management. Eur Urol. 2000;37(Suppl 1):33–6. doi: 10.1159/000052381. [DOI] [PubMed] [Google Scholar]
- 4.Sharma VK, Sethy PK, Dogra PN, Singh U, Das P. Primary tuberculosis of glans penis after intravesical Bacillus Calmette Guerin immunotherapy. Indian J Dermatol Venereol Leprol. 2011;77:47–50. doi: 10.4103/0378-6323.74979. [DOI] [PubMed] [Google Scholar]
- 5.French CG, Hickey L, Bell DG. Caseating Granulomas on the Glans Penis as a Complication of Bacille Calmette-Guérin Intravesical Therapy. Rev Urol. 2001;3:36–9. [PMC free article] [PubMed] [Google Scholar]
- 6.Yusuke H, Yoshinori H, Kenichi M, Akio H. Granulomatous balanoposthitis after intravesical Bacillus-Calmette-Guerin instillation therapy. Int J Urol. 2006;13:1361–3. doi: 10.1111/j.1442-2042.2006.01553.x. [DOI] [PubMed] [Google Scholar]
- 7.Kureshi F, Kalaaji AN, Halvorson L, Pittelkow MR, Davis MD. Cutaneous complications of intravesical treatments for bladder cancer: Granulomatous inflammation of the penis following BCG therapy and penile gangrene following mitomycin therapy. J Am Acad Dermatol. 2006;55:328–31. doi: 10.1016/j.jaad.2005.07.041. [DOI] [PubMed] [Google Scholar]
- 8.Abu-Nader R, Terrell CL. Mycobacterium bovis Vertebral Osteomyelitis as a Complication of Intravesical BCG Use. Mayo Clin Proc. 2002;77:393–7. doi: 10.4065/77.4.393. [DOI] [PubMed] [Google Scholar]