

A 34-year-old man presented with a one-month history of progressive shortness of breath, fever, night sweats, and fatigue. His medical history was remarkable for hepatitis B and a small perimembranous ventricular septal defect (VSD). Blood cultures were positive for α-hemolytic streptococcus, and transthoracic and transesophageal echocardiography confirmed vegetations on all 4 cardiac valves, a VSD, and a small pericardial effusion (Fig. 1).
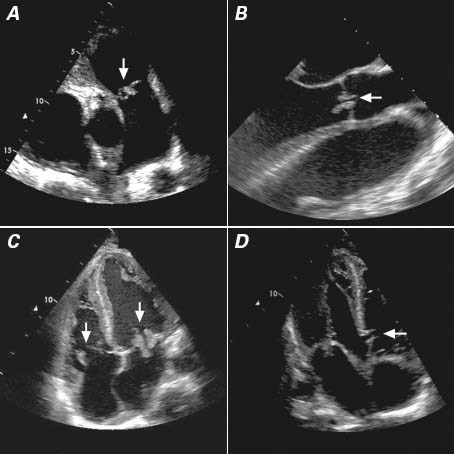
Fig. 1 Transthoracic (A, C, D) and transesophageal (B) echocardiographic images show vegetations (arrows) on the A) pulmonary valve, B) aortic valve, and C) tricuspid (left) and mitral (right) valves, together with D) a perimembranous ventricular septal defect (arrow).
Antibiotic coverage was started with benzyl penicillin, gentamicin, and clindamycin, but the patient showed no clinical improvement after 7 days and was referred for surgical intervention. The aortic, mitral, and tricuspid valves were replaced by prosthetic tissue valves, the pulmonary valve was repaired, and the VSD was closed.
Postoperative echocardiography confirmed well-seated and functioning aortic, mitral, and tricuspid valves, moderate pulmonary regurgitation, and no residual VSD. The patient made a good initial recovery and was extubated on postoperative day 5. Later, he developed intractable sepsis and resultant multiorgan failure. He did not recover and died on postoperative day 19.
Comment
Experience with quadruple-valve infective endocarditis is very limited due to its rare occurrence and the lethal nature of the disease.1–3 Although repair or replacement of all cardiac valves is technically feasible, refractory sepsis can become a major obstacle to recovery. In our patient, we inferred that the infective endocarditis disease process started in the left side of the heart and migrated to the right side via the VSD. The decision for continuing medical therapy or initiating surgical intervention should be made on a case-by-case basis, because successful surgical intervention does not guarantee resolution of the sepsis.
Footnotes
Address for reprints: Morteza Tavakkoli Hosseini, MD, Department of Cardiothoracic Surgery and Transplantation, Harefield Hospital, Hill End Rd., Harefield, UK UB9 6JH
E-mail: morteza.tavakkoli@gmail.com
References
- 1.Yao F, Han L, Xu ZY, Zou LJ, Huang SD, Wang ZN, et al. Surgical treatment of multivalvular endocarditis: twenty-one-year single center experience. J Thorac Cardiovasc Surg 2009; 137(6):1475–80. [DOI] [PubMed]
- 2.Krake PR, Zaman F, Tandon N. Native quadruple-valve endocarditis caused by Enterococcus faecalis. Tex Heart Inst J 2004;31(1):90–2. [PMC free article] [PubMed]
- 3.Seeburger J, Groesdonk H, Borger MA, Merk D, Ender J, Falk V, et al. Quadruple valve replacement for acute endocarditis. J Thorac Cardiovasc Surg 2009;137(6):1564–5. [DOI] [PubMed]