

Abstract
Giant coronary artery aneurysms are variously defined as more than 20 to 50 mm in size. They are rare, with a prevalence of 0.02% in a large surgical population. We present the case of a 68-year-old woman who reported an increased awareness of her chest. Multiple imaging techniques revealed a 7-cm coronary aneurysm. The aneurysm arose from a septal branch of the left anterior descending coronary artery and drained into the main pulmonary artery. Surgical excision with revascularization was successful.
We recommend definitive surgical intervention as a good long-term treatment for giant coronary artery aneurysms, after preoperative imaging has yielded the safest course of resection.
Key words: Coronary aneurysm/diagnosis/etiology/physiopathology/surgery, coronary vessels/surgery, treatment outcome
Giant coronary artery aneurysms are an extremely rare anatomic occurrence. Because of this, there is no established treatment. The apparent consensus is that surgical resection is the best long-term solution. Despite multiple imaging methods that can be used, defining the aneurysm's exact vasculature can be challenging. We report the case of a woman in whom we identified a giant coronary artery aneurysm, and we describe our treatment of that entity.
Case Report
In October 2011, a 68-year-old woman with a history of controlled hypertension visited her primary care physician, reporting increased awareness of her chest but no associated chest pain, pressure, or shortness of breath. An electrocardiogram showed an anterior-wall change that was different from baseline results. A stress echocardiogram showed a 4.5 × 4.9-cm extracardiac mass.
Computed tomographic angiography of the chest and heart showed a large, partially thrombosed vascular structure superior to the mid left ventricle and abutting the left side of the main pulmonary artery (PA) (Fig. 1). The mass was 7.2 × 5.6 cm axially × 5.7 cm craniocaudally. Its inflow was suspected to be from a septal branch of the left anterior descending coronary artery (LAD), with an outflow vessel draining into the main PA.
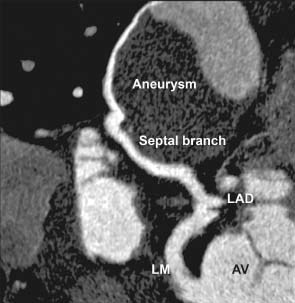
Fig. 1 Computed tomographic angiogram of the heart shows the giant aneurysm.
AV = aortic valve; LAD = left anterior descending coronary artery; LM = left main coronary artery
The patient was admitted to our cardiology service for further evaluation. She reported no clinical symptoms. Results of a physical examination were unremarkable except for a grade 2/6 holosystolic murmur that was best heard over the left sternal border. Coronary angiography revealed a large vascular aneurysm, supplied by a single large-caliber septal branch that arose from the proximal LAD and drained into the main PA (Fig. 2). On the basis of the pathologic results (Fig. 3), the aneurysm most likely originated in the LAD. Increased outflow from a congenital fistula into the PA resulted in the dilation of that vessel.
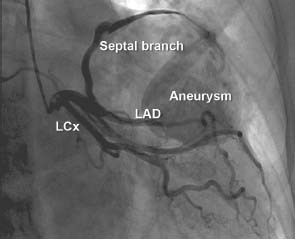
Fig. 2 Coronary angiogram shows a large vascular aneurysm supplied by a large-caliber septal branch arising from the proximal left anterior descending coronary artery and draining into the main pulmonary artery.
LAD = left anterior descending coronary artery; LCx = left circumflex coronary artery
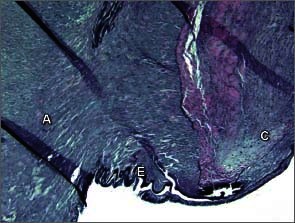
Fig. 3 Photomicrograph shows the junction of the feeding artery (C) and aneurysmal wall (A) separated by a residual internal elastic layer (E) (elastic stain, orig. ×100).
The patient declined coil embolization in favor of open surgery that might yield a more definitive result. Surgical intervention was through a median sternotomy. A 7-cm mass was identified in the lateral wall of the left ventricle (Figs. 4 and 5). After cardiopulmonary bypass was established, the mass was dissected from the heart. The feeding vessel, which was very friable and tortuous back to its origin at the proximal LAD, was ligated at its origin. Our concern about compromise of the LAD prompted us to harvest the saphenous vein and construct a graft to the distal LAD. We also transected the outflow at the level of the PA.
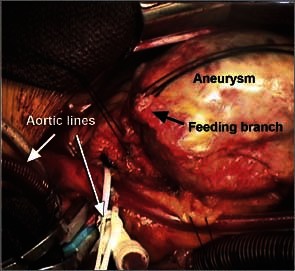
Fig. 4 Intraoperative photograph shows the ligated aneurysm.

Fig. 5 Photograph shows the resected aneurysm.
The patient recovered uneventfully and was discharged from the hospital on postoperative day 5. The final pathologic report confirmed a 7 × 6 × 5-cm coronary artery aneurysm.
Discussion
Coronary artery aneurysms in adults are usually associated with atherosclerosis; however, they have also been described in the settings of prior Kawasaki disease, trauma (including stent implantation and angioplasty), infection, congenital malformation, connective-tissue disorders, and autoimmune disease.1 The prevalence of coronary artery aneurysms is 1.2% to 4.9% in populations undergoing angiography2 and 1.4% in autopsy studies.1 Giant coronary artery aneurysms, variably defined as having diameters exceeding 20 to 50 mm, are much rarer than smaller aneurysms, despite having causes in common. In a surgical population of 30,268 patients, Li and colleagues3 found only 6 cases of giant coronary artery aneurysm (prevalence, 0.02%).
Because of the rarity of giant coronary artery aneurysms, no standard treatment protocol has been established. Coil embolization is a safe, low-risk option; however, surgical management is the preferred and most often reported strategy, particularly in symptomatic patients. The usual surgical approach is sternotomy and cardiopulmonary bypass followed by coronary artery bypass grafting (if necessary) and resection of the aneurysmal sac. The sac can be resected en bloc after proximal and distal ligation, or dissected before partial or full resection. In cases involving large aneurysmal size or complex anatomy, alternative approaches have included proximal and distal ligation of the aneurysmal vessel without resection,4 dissection of the sac followed by ligation,5 percutaneous intervention with stent placement,6 and atrial resection.7
We recommend definitive surgical intervention as a good long-term treatment for giant coronary artery aneurysms, after preoperative imaging has yielded the safest course of resection.
Footnotes
Address for reprints: John F. Lazar, MD, Department of Cardiac Surgery, University of Rochester School of Medicine and Dentistry, 601 Elmwood Ave., Box Surg, Rochester, NY 14642
E-mail: john_lazar@urmc.rochester.edu
References
- 1.Wright WP, Alpert MA, Mukerji V, Santolin CJ. Coronary artery aneurysms–a case study and literature review. Angiology 1991;42(8):672–9. [DOI] [PubMed]
- 2.Nichols L, Lagana S, Parwani A. Coronary artery aneurysm: a review and hypothesis regarding etiology. Arch Pathol Lab Med 2008;132(5):823–8. [DOI] [PubMed]
- 3.Li D, Wu Q, Sun L, Song Y, Wang W, Pan S, et al. Surgical treatment of giant coronary artery aneurysm. J Thorac Cardiovasc Surg 2005;130(3):817–21. [DOI] [PubMed]
- 4.Blank R, Haager PK, Maeder M, Genoni M, Rickli H. Giant right coronary artery aneurysm. Ann Thorac Surg 2007;84 (5);1740–2. [DOI] [PubMed]
- 5.Agarwal R, Jeevanandam V, Jolly N. Surgical treatment of a giant coronary artery aneurysm: a modified approach. Ann Thorac Surg 2007;84(4):1392–4. [DOI] [PubMed]
- 6.Dhakam S, Rahman N. Myocardial infarction in a youngster due to giant coronary aneurysm. Catheter Cardiovasc Interv 2011;77(4):528–9. [DOI] [PubMed]
- 7.Yoshida K, Kitahara H, Kondo R, Kurai M, Hyougotani A, Amano J. Giant intraatrial septal aneurysm originating from a branch of the left coronary artery. Jpn J Thorac Cardiovasc Surg 2006;54(10):432–6. [DOI] [PubMed]