

Abstract
Study Objectives:
Considerable research indicates that sleep disturbances and insomnia are more common and severe among individuals following a traumatic brain injury (TBI). It remains unclear, however, how the experience of multiple TBIs affect sleep disturbances and insomnia. The current study investigated the incidence and severity of insomnia and sleep complaints among active-duty military personnel who have sustained multiple TBIs.
Design and Setting:
Upon intake at a military TBI clinic located in Iraq, 150 male military patients completed standardized self-report measures and clinical interviews.
Measurements and Results:
Patients were categorized into three groups according to history of TBI: zero TBIs (n = 18), single TBI (n = 54), multiple TBIs (n = 78). Rates of clinical insomnia significantly increased across TBI groups (P < 0.001):- 5.6% for no TBIs, 20.4% for single TBI, and 50.0% for multiple TBIs. Insomnia severity significantly increased across TBI groups even when controlling for depression, posttraumatic stress disorder, and concussion symptom severity (B = 1.134, standard error = 0.577, P = 0.049).
Conclusions:
Multiple TBIs are associated with increased risk for and severity of sleep disturbance among male military personnel.
Citation:
Bryan CJ. Repetitive traumatic brain injury (or concussion) increases severity of sleep disturbance among deployed military personnel. SLEEP 2013;36(6):941-946.
Keywords: Insomnia, military, multiple TBI, sleep, TBI, traumatic brain injury
INTRODUCTION
A traumatic brain injury (TBI) occurs when brain function disruption occurs secondary to an external force, as indicated by alteration or loss of consciousness, posttraumatic amnesia, neurologic deficits (e.g., dizziness, concentration problems), and/or intracranial lesion, with severity (i.e., mild, moderate, severe) determined by the presence and/or duration of each.1 Considered a signature injury of the Iraq and Afghanistan conflicts, TBI is an issue of particular concern among military personnel due to increased risk of exposure to concussive injuries secondary to explosions and other military-related accidents (e.g., motor vehicle accidents, falls), with recent estimates suggesting that anywhere from 8-20% of military personnel who have deployed to Iraq and Afghanistan may have sustained a TBI.2
TBI is associated with increased risk for a host of health problems and consequences such as depression, anxiety, irritability, cognitive deficits, and functional impairment among clinical, nonclinical, and military samples.3,4 Sleep disruption is another common consequence of TBI3,4 that might result from trauma-induced physical changes within the brain and/or exacerbation of comorbid conditions such as depression or anxiety. In general, approximately half of individuals with TBI suffer from some sort of sleep disturbance following a TBI, including sleep maintenance, onset insomnia, and early morning awakenings,4–6 and one fourth had a diagnosed sleep disorder.4,7
Interestingly, mild TBI appears to be more strongly correlated with increased likelihood of sleep disturbance than more severe TBIs.5,7,8 The exact reasons for this pattern are not yet known, although it has been proposed that differences in the nature of injury (i.e., more diffuse injuries in milder TBIs) or recovery patterns may contribute differentially to insomnia complaints; alternatively, sleep problems might be reported less frequently among individuals with more severe TBI because sleep issues may be perceived as relatively less serious or problematic than other neuropsychologic or cognitive sequelae of TBI.8 Because most combat-related TBIs are rated as mild,9 it is possible that rising insomnia rates among military personnel during the past decade10 might be due in part to the increased incidence of mild TBI, although increased rates of comorbid psychiatric and physical conditions including posttraumatic stress disorder (PTSD), depression, and chronic pain might also play a role.
Although the association of TBI with sleep disturbance is well established, to date there are limited data regarding the potential effect of repetitive or multiple TBIs on sleep disturbance.11 Multiple TBIs are of particular concern to military populations given the likelihood of service members sustaining multiple injuries during the course of combat deployments. Hoge and colleagues,3 for instance, reported that 86.9% of soldiers reported being in the vicinity of two or more explosions during a combat deployment. Although the cognitive and psychologic sequelae of blast-induced TBI are not yet fully understood, a recent study found that TBI was diagnosed in 65.2% of military personnel referred for a TBI evaluation following exposure to a blast or explosion, and service members reported an average of two previous head injuries.12 In light of evidence that sleep disturbance is an important risk factor for a host of health-related outcomes including depression, anxiety disorders, cardiovascular disease, immune suppression, and even suicide in both general population and military samples,13,14 understanding the possible link between multiple TBIs and sleep disturbance is critical.
The primary aim of the current study was to investigate the incidence and severity of insomnia symptoms by lifetime TBIs in a clinical sample of deployed military personnel. We hypothesized that service members who had sustained multiple TBIs would have increased likelihood and severity of sleep disturbance and clinical insomnia, even when controlling for other common psychologic and concussion-related symptoms. We further sought to explore which type of sleep disturbances best differentiated TBI subgroups.
METHODS
Participants
Participants included 157 military personnel and four civilian contractors (n = 161) referred to an outpatient TBI clinic located at a combat support hospital in Iraq. Because of the extreme imbalance in sex distribution (93.2% male, n = 150), we included only male patients for the current study. Participants were predominantly Caucasian (70.7%), in the Army (79.3%), and had been in the military approximately 6.57 y (standard deviation [SD] = 5.47, range: 0.75 to 29.0 y). Rank distribution was primarily junior enlisted (E1-E4: 55.3%) and noncommissioned officer (E5-E6: 31.1%). Participants had deployed zero to six times previously (mean = 0.79, SD = 1.06), and ranged in age from 19 to 56 y (mean = 27.45, SD = 7.08).
Procedures
Data were collected in an outpatient TBI clinic located in central Iraq. Patients were referred to the TBI clinic for evaluation and treatment of possible head injuries. Upon arrival at the clinic, patients underwent a standardized intake evaluation that included computerized neurocognitive testing, psychologic and physical health questionnaires, a clinical interview conducted by a clinical psychologist, and a physical examination by a physician, information that was used to plan and coordinate subsequent treatment. As a part of their clinical interviews, patients were asked to report the number of previous head injuries that were sustained during their deployment and the number that were sustained prior to their deployment (whether occurring prior to or during military service). Only previous head injuries that met criteria for a diagnosis of TBI were recorded. Clinical data were stored in a clinic database and then deidentified prior to analysis. Study approval was obtained from the Brooke Army Medical Center Institutional Review Board, the U.S. Army Medical Research and Material Command's Office of Research Protection, and the Multi-National Force-Iraq Institutional Official.
TBI Diagnosis
TBI diagnoses were made by a licensed clinical psychologist and defined as a traumatically induced structural injury and/or physiologic disruption of brain function as a result of an external force that is indicated by new onset or worsening of at least one of the following clinical signs immediately following the event: (1) any period of loss of or decreased level of consciousness; (2) any loss of memory for events immediately before or after the injury; (3) any alteration in mental state at the time of the injury; (4) neurologic deficits that may or may not be transient; and (5) intracranial lesion.15
Materials
Insomnia Severity Index
The Insomnia Severity Index (ISI)16,17 is a seven-item self-report scale that assesses subjective symptoms of insomnia. Each item is scored on a 0 to 4 scale, with the total score calculated by summing the scores of each item, resulting in a range of 0 to 28. Higher scores indicate more severe levels of insomnia. Among patients with TBI, self-reported ISI scores have been validated by objective and physiologic measures of sleep.6 In the current sample, 58 patients (36.0%) reported minimal insomnia (scores 0-7), 48 patients (29.8%) reported subthreshold insomnia (scores 8-14), 43 patients (26.7%) reported moderate clinical insomnia (scores 15-21), and 12 patients (7.5%) reported severe clinical insomnia (scores 22-28). See Table 1 for additional descriptive statistics. The internal consistency and convergent validity of the ISI are very good.
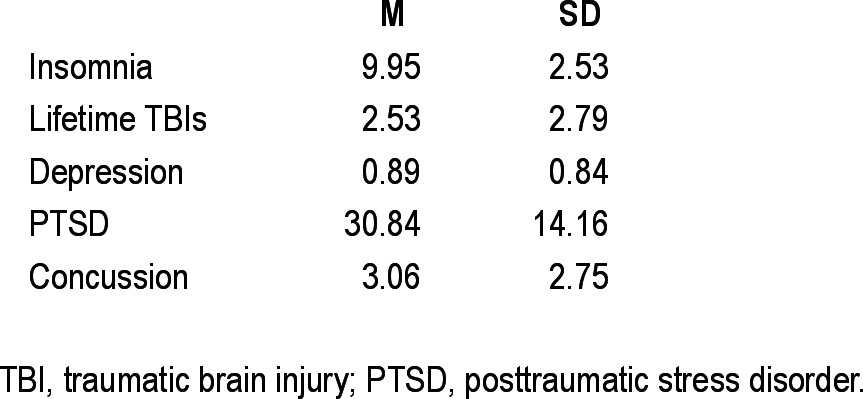
Table 1.
Means and standard deviations of all variables (n = 150)
Depression Subscale of the Behavioral Health Measure
The Depression subscale of the Behavioral Health Measure (BHM)18 is a six-item self-report scale that assesses symptoms of depression. Each item is scored on a 0 to 4 scale, with the total score calculated as the mean score of the six items, resulting in a scale score range of 0 to 4. Higher scores indicate greater health (i.e., less depression), although for ease of interpretation in the current study, the depression scores were reverse-keyed such that higher scores indicated more severe depression. In the current sample, 103 patients (65.6%) had scores in the normal or minimal range (0-1.16), 14 patients (8.7%) scored in the “at risk” range (1.17-1.38), and 44 patients (27.3%) scored in the clinical range (1.39-4.00). See Table 1 for additional descriptive statistics. The internal consistency and convergent validity of the Depression subscale are very good.19
Posttraumatic Stress Disorder Checklist
The Posttraumatic Stress Disorder Checklist (PCL)20,21 is a 17-item self-report scale that assesses symptoms of PTSD. Each item is scored on a 1 to 5 scale, with the total score calculated as the sum of each item, resulting in a range of 17 to 85. Higher scores indicate more severe PTSD symptoms, with a cutoff score of 50 established as optimal for a diagnosis of PTSD in clinical samples. In the current study, 21 participants (13.0%) scored above this recommended cutoff score. See Table 1 for additional descriptive statistics. The internal consistency and validity of the PCL are very good.
Military Acute Concussion Evaluation
The history portion of the Military Acute Concussion Evaluation (MACE)22 is a clinician-administered interview that assesses 10 concussion symptoms (headache, dizziness, memory problems, balance problems, nausea/vomiting, difficulty concentrating, irritability, visual disturbances, ringing in the ears, and other) currently being experienced by the respondent. Each symptom is dichotomously scored as either present or absent. Total number of symptoms is summed to provide an overall metric of concussion symptom severity, with higher scores indicating more severe concussion symptomatology. In the current study, participants reported a range of 0 (n = 36, 22.4%) to 10 (n = 3, 1.9%) concussion symptoms. See Table 1 for additional descriptive statistics.
Statistical Analyses
Analyses were conducted to investigate the associations among lifetime TBIs and insomnia while controlling for other clinical symptoms. Participants were classified into three groups according to number of lifetime TBIs: zero, one, or multiple (i.e., two or more). Generalized linear regression with robust estimation was then used to determine the association of lifetime TBIs with insomnia severity above and beyond the effects of depression, PTSD, and concussion symptom severity. Pairwise comparisons of mean scores according to TBI group were then conducted to compare insomnia severity scores according to TBI group.
RESULTS
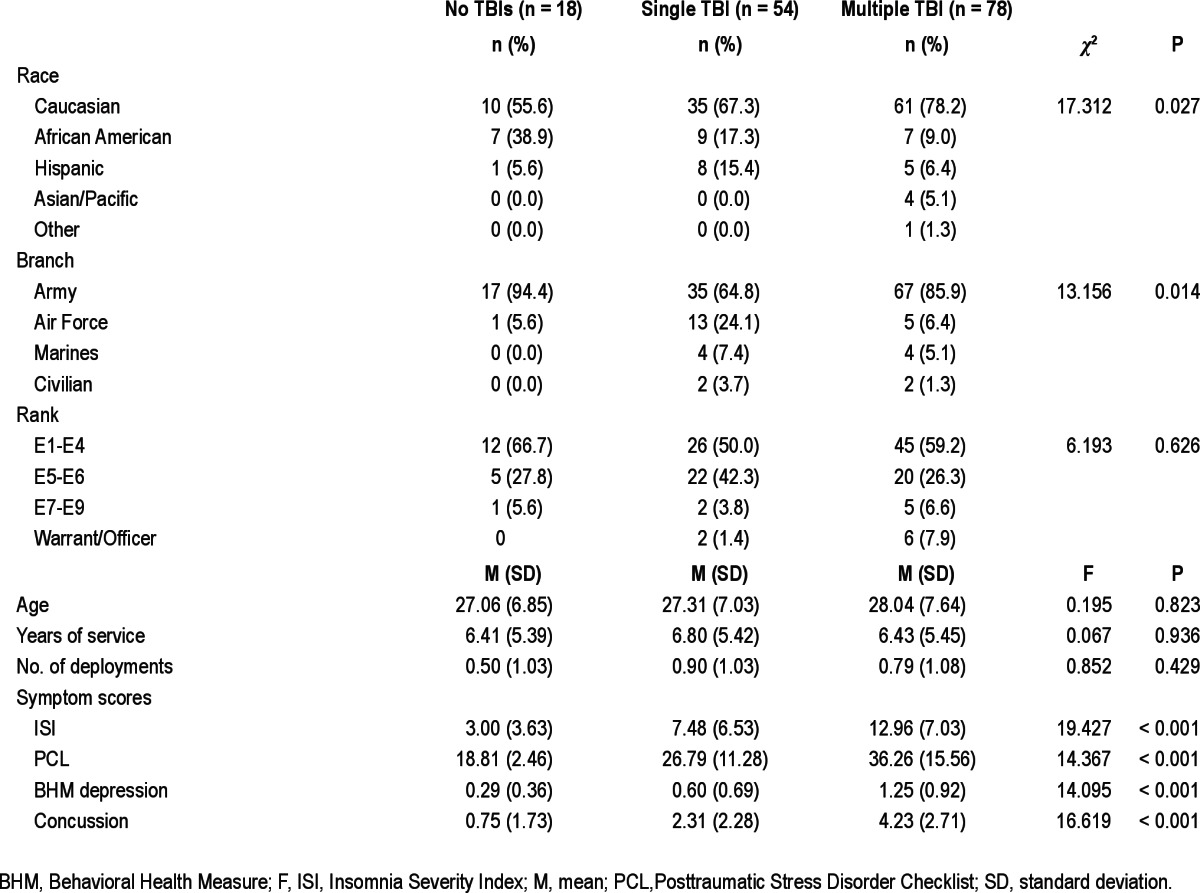
Means, SD, and intercorrelations of predictor variables are reported in Tables 1 and 2. Total number of lifetime TBIs was significantly correlated with more severe insomnia (r = 0.26, P = 0.001), depression (r = 0.32, P < 0.001), PTSD (r = 0.34, P < 0.001), and concussion (r = 0.39, P < 0.001) symptom severity. As would be expected, symptom scores were highly intercorrelated with one another (r > 0.60, P < 0.001). The total number of lifetime TBIs ranged from 0 to 19 (mean = 2.53, SD = 2.83, median = 2.00). Eighteen patients (12.0%) had never experienced a TBI during their lifetime, 54 (36.0%) had experienced one lifetime TBI, and 78 (52.0%) had experienced two or more lifetime TBIs. Sample descriptors by TBI group are displayed in Table 3. As can be seen, there were minimal differences between groups on most demographic variables, although the single TBI group had a greater proportion of Air Force personnel and the zero TBI group had a greater proportion of African American personnel. Because these between-group differences did not affect outcomes, however, reported results are for analyses without race included as a covariate.
Table 2.
Intercorrelations of all variables (n = 150)

Table 3.
Group differences in demographic and clinical variables
Does the Incidence of Clinical Insomnia and Specific Sleep Disturbance Increase in Frequency with Number of TBIs?
To determine if the incidence of clinical insomnia increased with greater number of lifetime TBIs, we dichotomized ISI scores according to a predetermined ISI score of 14, which has been recommended as the optimal cutoff for a diagnosis of clinical insomnia, and then conducted chi-square analyses by TBI group. Results indicated that the likelihood of clinical insomnia significantly increased by TBI group (χ2 (2) = 19.859, P < 0.001, Φ = 0.364): 5.6% of those with no TBIs, 20.4% of those with a single TBI, and 50.0% of those with multiple TBIs.
To determine differences in the severity of onset insomnia, maintenance insomnia, and early morning awakening by TBI group, we used the first three items of the ISI, which asked patients to rate the past week severity of insomnia problem(s) in the following areas on a scale of 0 (none) to 4 (very severe): difficulty falling asleep (i.e., onset insomnia), difficulty staying asleep (i.e., maintenance insomnia), and waking up too early (i.e., early morning awakening). We dichotomized responses using a predetermined cutoff of score of 2 (moderate) or higher to indicate a positive report of each complaint. As displayed in Table 4, the frequency of patients reporting each type of sleep disruption increased in frequency with number of TBIs: onset insomnia (no TBI: 16.7%, single TBI = 48.1%, multiple TBI = 66.7%; χ2 (2) = 15.449, P < 0.001, Φ = 0.330), maintenance insomnia (no TBI: 22.2%, single TBI: 36.5%, multiple TBIs: 68.6%; χ2 (2) = 18.957, P < 0.001, Φ = 0.368), and early morning awakening (no TBI: 16.7%, single TBI = 36.5%, multiple TBIs: 58.6%; χ2 (2) = 12.552, P = 0.002, Φ = 0.299). Results indicated that, in general, approximately two to three times as many patients with a single TBI than zero TBIs reported moderate to severe levels of each type of sleep disturbance, and approximately 1.5 times as many patients with multiple TBIs than with a single TBI reported moderate to severe levels of each type of sleep disturbance.
Table 4.
Proportion of patients reporting moderate or higher severity of onset insomnia, maintenance insomnia, and early morning awakening by TBI group

Does the Severity of Insomnia Symptoms Increase with Number of TBIs?
Next, to determine if TBI group accounted for increased severity of insomnia above and beyond the effects of cooccurring psychologic and concussion symptoms, regression analyses were conducted in two steps. In the first step, TBI group was entered as a sole predictor of insomnia severity, resulting in a statistically significant relationship (B = 4.913, standard error [SE] = 0.669, P < 0.001) indicating that insomnia severity increased across TBI group severity: no TBIs (mean = 4.06, SD = 4.67), single TBI (mean = 7.83, SD = 6.70), and multiple TBIs (mean = 12.62, SD = 7.02; see Figure 1). Pairwise comparisons revealed that patients with multiple TBIs had significantly more severe insomnia than patients with zero TBIs (P < 0.001) or a single TBI (P < 0.001), and patients with a single TBI had significantly more severe insomnia than those with zero TBIs (P = 0.039). In the second step, PTSD, depression, and concussion symptoms were entered into the regression equation as covariates. Results indicated that TBI group remained a significant predictor of insomnia severity (B = 1.134, SE = 0.577, P = 0.049) above and beyond the effects of depression (B = 3.675, SE = 0.741. P < 0.001), PTSD (B = 0.100, SE = 0.050, P = 0.044), and concussion (B = 0.513, SE = 0.199, P = 0.010) symptom severity. Pairwise comparisons revealed that patients with multiple TBIs had significantly more severe insomnia than patients with no TBIs (P = 0.045), but not patients with a single TBI (P = 0.249). Patients with a single TBI also did not significantly differ from those with zero TBIs (P = 0.206). Depression, PTSD, and concussion symptom severity therefore explained some of the differences in insomnia severity between TBI groups.
Figure 1.
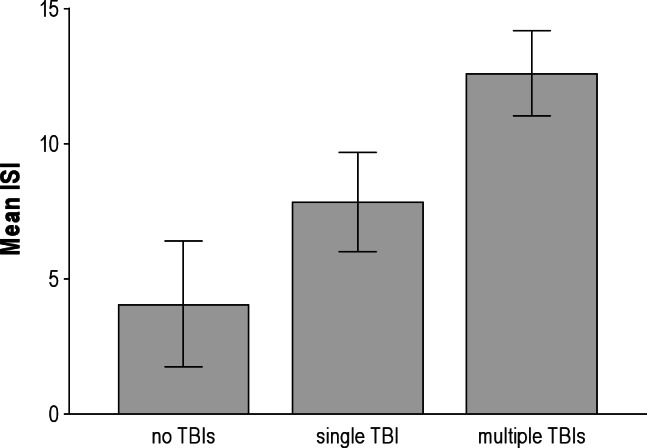
Mean insomnia scores (with 95% confidence intervals), by traumatic brain injury (TBI) group. Group differences in ISI scores are as follows: 0 < 1 < 2. ISI, Insomnia Severity Index.
DISCUSSION
Results of the current study were consistent with expectations that multiple TBIs are associated with increased incidence of clinical insomnia and severity of sleep disturbance. As compared with patients with no history of TBI (5.6%), approximately four times as many patients with a single TBI (22.4%) and 10 times as many patients with multiple TBIs (47.6%) exceeded the threshold for clinical insomnia. The rates of insomnia among our zero TBI and single TBI groups are consistent with prior studies on prevalence rates of insomnia, which are estimated to range from 6-10% of the general population23,24 and 25-29% of patients with TBI,4 although no studies estimating the prevalence of insomnia among patients with multiple TBIs were identified.
Consistent with previous research,4 all three types of sleep disturbances investigated—i.e., onset insomnia, maintenance insomnia, and early morning awakening—also increased in frequency and severity across TBI groups. Prior research has indicated that sleep maintenance is a more commonly reported sleep complaint than onset insomnia and early morning awakening among individuals with TBI,5,24 although these studies did not control for total number of lifetime TBIs. In the current study, onset insomnia was reported with somewhat greater frequency than maintenance insomnia and early morning awakening among service members with a single TBI, but all three types of sleep disturbance occurred with relatively equal frequency among patients with multiple TBIs. We additionally found that onset insomnia best differentiated patients with any number of TBIs (i.e., one or multiple TBIs) from those with no TBIs, but maintenance insomnia best differentiated multiple TBI patients from single TBI patients. Results suggest that different types of sleep complaints might be differentially related to number of TBIs. Specifically, onset insomnia might be most vulnerable to disruption following a first TBI, and maintenance insomnia might intensify following an additional TBI. Further studies are needed to replicate these findings and to better understand how different types of sleep disturbance might be differentially related to history of TBIs.
Results of our regression analyses indicated that number of lifetime TBIs is a significant predictor of overall insomnia severity, and remained a robust predictor even when controlling for depression, PTSD, and concussion symptom severity, suggesting that number of TBIs is an important risk factor for sleep disturbance among military personnel. Given that sleep disruption is associated with slowed recovery and continued functional impairment following TBI,26 and could potentially exacerbate psychiatric problems, memory, mood, behavior, and social functioning,27 these results suggest that recovery might be delayed or attenuated among military personnel who have sustained multiple TBIs relative to those who have sustained a first TBI. From a clinical perspective, this suggests that targeting sleep disturbance might be an important early intervention for patients who have sustained a second (or subsequent) TBI. Preliminary evidence suggests that sleep outcomes improve with cognitive-behavioral treatment for insomnia among patients with TBI,6,7,28 although the effect of these sleep-related outcomes on more global TBI recovery has not been thoroughly tested. Future studies might investigate early sleep interventions as a potential active ingredient for rapid and full recovery from TBI.
Several limitations to the current study warrant discussion. First, our study was limited to a clinical sample of military personnel deployed to Iraq at the time of their index injury or exposure. Generalizability to the broader military must therefore be made with caution, because we are unable to draw any conclusions about how multiple TBIs affect the sleep of military personnel who do not present for treatment. Related to this limitation is our cross-sectional design, which limits our ability to determine directionality of the relationship among sleep complaints and TBI. It is possible, for instance, that military personnel with insomnia are more vulnerable to neurologic disruptions following head injury. Longitudinal studies will be required to better tease apart the temporal relationship between TBI and sleep disturbance. Our use of self-report methodology might also introduce response bias that might affect conclusions. Although previous studies have found a high correlation among self-report and objective methods for assessing sleep disruption, recall bias specific to describing and recounting past instances of TBI could be a limitation. Despite these limitations, the current study provides useful information about sub-populations of patients who have experienced a TBI, and the importance of considering multiple TBIs as a unique risk factor for sleep disturbance.
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest.
REFERENCES
- 1.Department of Veterans Affairs and Department of Defense. Clinical practice guideline: management of concussion/mild traumatic brain injury. Washington, DC: Department of Veterans Affairs and Department of Defense; 2009. [Google Scholar]
- 2.Tanielian T, Jaycox LH. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, CA: RAND Corporation; 2008. [Google Scholar]
- 3.Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in US soldiers returning from Iraq. N Engl J Med. 2008;358:453–63. doi: 10.1056/NEJMoa072972. [DOI] [PubMed] [Google Scholar]
- 4.Mathias JL, Alvaro PK. Prevalence of sleep disturbances, disorders, and problems following traumatic brain injury: a meta-analysis. Sleep Med. 2012;13:898–905. doi: 10.1016/j.sleep.2012.04.006. [DOI] [PubMed] [Google Scholar]
- 5.Beetar JT, Guilmette TJ, Sparadeo FR. Sleep and pain complaints in symptomatic traumatic brain injury and neurologic problems. Arch Phys Med Rehabil. 1996;77:1298–302. doi: 10.1016/s0003-9993(96)90196-3. [DOI] [PubMed] [Google Scholar]
- 6.Ouellet MC, Morin CM. Subjective and objective measures of insomnia in the context of traumatic brain injury: a preliminary study. Sleep Med. 2006;7:486–97. doi: 10.1016/j.sleep.2006.03.017. [DOI] [PubMed] [Google Scholar]
- 7.Ouellet MC, Beaulieu-Bonneau S, Morin CM. Insomnia in patients with traumatic brain injury: frequency, characteristics, and risk factors. J Head Trauma Rehabil. 2006;21:199–212. doi: 10.1097/00001199-200605000-00001. [DOI] [PubMed] [Google Scholar]
- 8.Orff HJ, Avalon L, Drummond SP. Traumatic brain injury and sleep disturbance: a review of current research. J Head Trauma Rehabil. 2009;24:155–65. doi: 10.1097/HTR.0b013e3181a0b281. [DOI] [PubMed] [Google Scholar]
- 9.MacGregor AJ, Shaffer RA, Dougherty AL, et al. Prevalence and psychological correlates of traumatic brain injury in Operation Iraqi Freedom. J Head Trauma Rehabil. 2010;25:1–8. doi: 10.1097/HTR.0b013e3181c2993d. [DOI] [PubMed] [Google Scholar]
- 10.Medical Surveillance Monthly Report. Insomnia, active component, US armed forces, January 2000–December 2009. Med Surv Monthly Rep. 2010;17:12–5. [Google Scholar]
- 11.Warden D. Military TBI during the Iraq and Afghanistan wars. J Head Trauma Rehabil. 2006;21:398–402. doi: 10.1097/00001199-200609000-00004. [DOI] [PubMed] [Google Scholar]
- 12.Luethcke CA, Bryan CJ, Morrow CE, Isler WC. Comparison of concussive symptoms, cognitive performance, and psychological symptoms between acute blast- versus nonblast-induced mild traumatic brain injury. J Int Neuropsychol Soc. 2011;17:36–45. doi: 10.1017/S1355617710001207. [DOI] [PubMed] [Google Scholar]
- 13.Taylor DJ, McRae CM, Gehrman P, et al. Insomnia. In: Hersen M, Rosqvist J, editors. Handbook of psychological assessment, case conceptualization, and treatment, vol. 1: adults. Hoboken, NJ: John Wiley & Sons; 2007. pp. 674–700. [Google Scholar]
- 14.Luxton DD, Greenburg D, Ryan J, Niven A, Wheeler G, Mysliwiec V. Prevalence and impact of short sleep duration in redeployed OIF soldiers. Sleep. 2011;34:1189–95. doi: 10.5665/SLEEP.1236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.DOD/VA Traumatic Brain Injury Task Force. Report to the Surgeon General: Traumatic Brain Injury Task Force. Department of Defense and Department of Veterans Affairs; 2008. [Google Scholar]
- 16.Bastien CH, Vallieres A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297–307. doi: 10.1016/s1389-9457(00)00065-4. [DOI] [PubMed] [Google Scholar]
- 17.Morin CM. Insomnia: psychological assessment and management. New York, NY: Guilford Press; 1993. [Google Scholar]
- 18.CelestHealth Solutions. Clinical report manual: college counseling version. Newburgh, IN: CelestHealth Solutions; 2008. [Google Scholar]
- 19.Blount TH, Bryan CJ, Kanzler KE, et al. Psychometric properties of the BHM-20 in military samples. Poster presented at the annual meeting of the Association for Behavioral and Cognitive Therapy; October 2010; San Francisco, CA. [Google Scholar]
- 20.Blanchard EB, Jones-Alexander J, Buckley TC, Forneris CA. Psychometric properties of the PTSD checklist (PCL) Behav Res Ther. 1996;34:669–73. doi: 10.1016/0005-7967(96)00033-2. [DOI] [PubMed] [Google Scholar]
- 21.Weathers FW, Litz BT, Herman DS, et al. The PTSD checklist: reliability, validity, and diagnostic utility. Paper presented at the annual meeting of the International Society for Traumatic Stress Studies; October 1993; San Antonio, TX. [Google Scholar]
- 22.Defense and Veterans Brain Injury Center. Military acute concussion evaluation (MACE) Washington, DC: Defense and Veterans Brain Injury Center; 2007. [Google Scholar]
- 23.National Institutes of Health. National Institutes of Health state of the science conference statement on manifestations and management of chronic insomnia in adults, June 13-15, 2005. Sleep. 2005;28:1049–57. doi: 10.1093/sleep/28.9.1049. [DOI] [PubMed] [Google Scholar]
- 24.Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Med Rev. 2002;6:97–111. doi: 10.1053/smrv.2002.0186. [DOI] [PubMed] [Google Scholar]
- 25.Perlis ML, Artiola L, Giles DE. Sleep complaints in chronic postconcussion syndrome. Percept Mot Skills. 1997;84:595–9. doi: 10.2466/pms.1997.84.2.595. [DOI] [PubMed] [Google Scholar]
- 26.Worthington AD, Melia Y. Rehabilitation is compromised by arousal and sleep disorders: results of a survey of rehabilitation centres. Brain Inj. 2006;20:327–32. doi: 10.1080/02699050500488249. [DOI] [PubMed] [Google Scholar]
- 27.Zeitzer JM, Frieman L, O'Hara R. Insomnia in the context of traumatic brain injury. J Rehabil Res Dev. 2009;46:827–36. doi: 10.1682/jrrd.2008.08.0099. [DOI] [PubMed] [Google Scholar]
- 28.Castriotta RJ, Atanasov S, Wilde MC, Masel BE, Lai JM, Kuna ST. Treatment of sleep disorders after traumatic brain injury. J Clin Sleep Med. 2009;15:137–44. [PMC free article] [PubMed] [Google Scholar]