

Abstract
INTRODUCTION
Internal intestinal hernia has been defined as a bulging of the intestines through a normal or an abnormal peritoneal or mesenteric opening.1 Internal hernias are a rare cause of small-bowel obstruction, with a reported incidence of 0.2–0.9%.2
PRESENTATION OF CASE
In this report, the patient presented with multiple episodes of intestinal obstruction. High index of suspicion aided the appropriate management of this case. An abdominal CT revealed signs of small bowel obstruction. With negative signs and symptoms indicating adhesions, malignancy or inflammatory causes, mesenteric defect was suspected. When the patient underwent laparotomy, multiple mesenteric defects were found.
DISCUSSION
In the adult population, acquired mesenteric defects are more common than congenital defects. They can be caused by bowel surgery or abdominal trauma.11 Patients with a history of blunt abdominal trauma may present with late complication caused by a missed diagnosis of an associated injury, such as bowel mesenteric injuries.
In this case, the author describes a patient who developed multiple attacks of small bowel obstruction. He had no previous history of similar symptoms but did give a history of recent abdominal trauma managed conservatively. An abdominal CT was performed, and it showed signs of a mesenteric defect. In such a case, early operative intervention is essential to decrease morbidity and increase survival. 16
CONCLUSION
The diagnosis of post traumatic mesenteric injuries can be missed in conservatively managed trauma cases. For this reason, the decision of non-operative approach should be made following the exclusion of associated injuries.
Keywords: Mesenteric defect, Internal hernia, Intestinal obstruction
1. Introduction
Internal intestinal hernia has been defined as bulging of the intestines through a normal or an abnormal peritoneal or mesenteric opening.1
Internal hernias are a rare cause of small-bowel obstruction, with a reported incidence of 0.2–0.9%.2
Based on the site of the opening, they are divided into many types. Paraduodenal hernias account for about 30–53% of all intestinal herniations.1 Based on the etiology, internal hernias can be congenital or acquired, and herniation may be persistent or intermittent. These hernias are considered dangerous and may be even lethal because of the risk of strangulation.3 In this case report, the author presents a 26-year-old male who developed intestinal obstruction caused by internal hernia due to acquired multiple mesenteric defects.
2. Case report
A fit 26-year-old male, following a motor vehicle accident (MVA) in which he had sustained a splenic injury 7 months earlier, presented with a history of abdominal pain and constipation for a 6-month duration.
He was admitted to King Abdulaziz University Hospital as a trauma case. Upon investigations, he was found to have splenic contusions, which were conservatively treated.
Two weeks following his discharge, he started to complain about multiple episodes of epigastric and left upper quadrant pain. The pain was gradual in onset, on and off, progressive, colicky in nature, and moderate in severity. It was associated with constipation. He had no history of weight loss, decrease in appetite, hernia, previous abdominal surgeries, hematemesis, melena or fever.
Two months ago, the pain became more severe and was associated with nausea and vomiting. He vomited twice and the content was non bilious. During that period, an upper GI endoscopy was performed, and he was diagnosed with gastritis. He was treated and his symptoms improved for 2 weeks, however he started to have the same pain again. The last episode was 5 days prior to his presentation.
Upon physical examination, the patient was conscious, alert, and oriented. He looked in pain. His vital signs were as follows: temperature 36.9 °C, heart rate 126, blood pressure 106/59, respiratory rate 20, and O2Sat 93%. Abdominal examination showed a distended abdomen. No surgical scars were noted, and hernial orifices were intact. On palpation, the abdomen was soft and lax with tenderness at the epigastric area, but no abdominal guarding. On auscultation, bowel sounds were positive. Per rectal Examination was unremarkable.
An abdominal X-ray in the erect position was done, which showed multiple small air fluid levels (Fig. 1). Transverse colon was dilated and distended by gas. Maximum diameter was about 8 cm (Fig. 2). CT scan of the abdomen revealed significant dilatation of the distal jejunum and proximal ileal loop forming a closed loop obstruction. A transition zone was seen in the left mid abdomen, where there was significant surrounding mesenteric fat stranding, and ischemia could not be excluded (Fig. 3).
Fig. 1.

An erect abdominal radiograph which revealed multiple air fluid levels.
Fig. 2.

An abdominal radiograph which showed a dilated small bowel loop.
Fig. 3.

A pre-operative CT scan of the abdomen (coronal view), significant dilatation of the distal jejunum and proximal ileal loop forming a closed loop obstruction.
The patient was prepared for an exploratory laparotomy. The intraoperative findings were multiple pre-mesenteric defects with dilated jejunal loop proximally and distally collapsed (Figs. 4 and 5). Inflammatory small bowel segment was found.
Fig. 4.
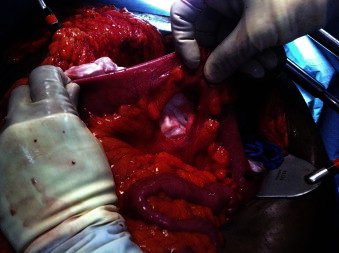
The intraoperative finding, demonstrating a mesenteric defect.
Fig. 5.

The intraoperative findings, showing dilated jejunal loop.
The mesenteric defects were repaired, in addition to resection of small bowel segment and primary anastomosis. On the 9th day following surgery, he was discharged without any complications.
3. Discussion
The advances in the management of blunt abdominal trauma have made non-operative management the standard approach for stable patients. Therefore, patients with history of blunt abdominal trauma may present with late complication caused by a missed diagnosis of an associated injury such as bowel mesenteric injuries.
About 13.5% of all patients, going to laparotomy due to blunt abdominal trauma, were found to have mesenteric injuries.4,5
Patients who have intra-abdominal free fluid on CT scan without solid organ injury were found to have mesenteric injuries or bowel injury.6
Internal hernias are considered a rare type of hernias accounting for 0.2–0.9%.2,7. Trans-mesenteric hernias are one type of internal hernias, and they can be congenital or acquired.8,9 Congenital mesenteric defects are common in the pediatric age group, and they commonly present with intestinal atresia.10
In the adult population, acquired mesenteric defects are more common than congenital defects. They can be caused by bowel surgery or abdominal trauma.11
Patients with mesenteric defect either can be asymptomatic or can present with signs and symptoms of mechanical bowel obstruction.12,13
In this case, the author describes a patient who developed multiple attacks of small bowel obstruction. He had never had a similar history before and had a positive history of recent conservatively managed abdominal trauma. In a patient with mesenteric defect, an abdominal CT might show signs of bowel wall thickening, small bowel obstruction and narrowed intestinal lumen.4 All of these CT signs were found to be positive in the described case.
In patients with no previous history of surgery, other causes of mechanical obstruction should be ruled out, such as internal hernias, foreign bodies and ischemic strictures.11 Although laparotomy is considered in the treatment of such cases, laparoscopy can aid in both diagnosis and treatment.14 Early operative intervention is essential to decrease morbidity and increase survival.16
4. Conclusion
Intestinal obstruction caused by a paramesenteric internal hernia is considered rare. The diagnosis of post traumatic mesenteric injuries can be missed in conservatively managed trauma cases. For that reason, the decision of non-operative approach should follow the exclusion of associated injuries. CT scan is considered an important tool for the assessment of this population.15
Conflict of interest statement
There was no conflict of interest.
Funding
No funding was provided for this case report.
Ethical approval
Written informed consent was obtained from the patient. The patient was informed that his case will be written for publication as a case report with the accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Dr. Felemban B. is the treating surgeon of this case. He contributed in revising and editing of the case report. Aref H. contributed in writing of the manuscript of this case report.
Acknowledgment
I would like to express my sincere appreciation to Dr. Magdy Abdulmoneum, Dr. Ahmed Zahrani and to Dr. Noor Basendowah, for their valuable and constructive suggestions during the development of this case report.
References
- 1.Virich G., Davies W. A massive left paraduodenal fossa hernia as an unusual cause of small bowel obstruction. Annals of the Royal College of Surgeons of England. 2010;92(4):7–9. doi: 10.1308/147870810X12659688851997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Meyers M.A. Paraduodenal hernias: radiologic and arteriographic diagnosis. Radiology. 1970;95:29–37. doi: 10.1148/95.1.29. [DOI] [PubMed] [Google Scholar]
- 3.Blachar A., Federle M.P., Dodson F. Internal hernia: clinical and imaging findings in 17 patients with emphasis on CT criteria. Radiology. 2001;218(January):168–174. doi: 10.1148/radiology.218.1.r01ja5368. [DOI] [PubMed] [Google Scholar]
- 4.De Backer A.I., De Schepper A.M., Vaneerdeweg W., Pelckmans P. Intestinal stenosis from mesenteric injury after blunt abdominal trauma. European Radiology. 1999;9:1429–1431. doi: 10.1007/s003300050863. [DOI] [PubMed] [Google Scholar]
- 5.Cox E.F. Blunt abdominal trauma. Annals of Surgery. 1984;199:467–474. doi: 10.1097/00000658-198404000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Venkatesh K.R., McQuay N., Jr. Outcomes of management of in stable children with intra-abdominal free fluid without solid organ injury after blunt abdominal trauma. Journal of Trauma. 2007;62(1(January)):216–220. doi: 10.1097/01.ta.0000222585.76302.17. [DOI] [PubMed] [Google Scholar]
- 7.Passas V., Karavias D., Grilias D., Birbas A. Computed tomography of left paraduodenal hernia. Journal of Computer Assisted Tomography. 1986;10:542–543. [PubMed] [Google Scholar]
- 8.Blachar A., Federle M.P., Dodson S.F. Internal hernia: clinical and imaging findings in 17 patients with emphasis on CT criteria. Radiology. 2001;218:68–74. doi: 10.1148/radiology.218.1.r01ja5368. [DOI] [PubMed] [Google Scholar]
- 9.Kulacoglu H., Tumer H., Aktimur R., Kusdemir A. Internal herniation with fatal outcome: herniation through an unusual aperture between epiploic appendices and greater omentum. Acta Chirurgica Belgica. 2006;106:109–111. doi: 10.1080/00015458.2006.11679849. [DOI] [PubMed] [Google Scholar]
- 10.Murphy D.A. Intestinal hernias in infancy and childhood. Surgery. 1964;55:311–316. [PubMed] [Google Scholar]
- 11.ur Rehman Z., Khan S. Large congenital mesenteric defect presenting in an adult. Saudi Journal of Gastroenterology: Official Journal of the Saudi Gastroenterology Association. 2010;16(3):223–225. doi: 10.4103/1319-3767.65193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Byard R.W., Wick R. Congenital mesenteric defects and unexpected death – a rare finding at autopsy. Pediatric and Developmental Pathology. 2008;11:245–248. doi: 10.2350/07-12-0392.1. [DOI] [PubMed] [Google Scholar]
- 13.Nawaf Shatnawi J., Kamal Bani-Hani E. Unusual causes of mechanical small bowel obstruction. Saudi Medical Journal. 2005;26(10):1546–1550. [PubMed] [Google Scholar]
- 14.Akbulut S. Unusual cause of intestinal obstruction: left paraduodenal hernia. Case Reports in Medicine. 2012;2012:529246. doi: 10.1155/2012/529246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ali Mahmood, Nadia Mahmood, Dana Busch Asynchronous small bowel obstruction: a complication of blunt abdominal trauma. Radiology Case Reports, North America. 2007;2:81. doi: 10.2484/rcr.v2i2.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Xeropotamos N.S., Nousias V.E., Ioannou H.V., Kappas A.M. Mesenteric injury after blunt abdominal trauma. European Journal of Surgery. 2001;167(2):106–109. doi: 10.1080/110241501750070547. [DOI] [PubMed] [Google Scholar]