

Abstract
Background:
Compressive neuropathy of median nerve is relatively common but development of an hourglass like constriction is a rare phenomenon. The purpose of this study is to show morphologic changes of median nerve in advances carpal tunnel syndrome.
Methods:
Eighty patients with thenar atrophy, anesthesia and paresthesia of first, second and third finger and severe changes of EMG-NCV were chosen for surgery. All the cases were operated by classic approach.
Results:
At ten cases, nerve was constricted in point and in six patients’ area constriction was seen. Internal and external neurolysis was performed in all the cases. In two of them because of the wide and severe constriction, resection and end-to-end repair was performed. All the patients have been examined periodically. Mean follow-up was 12 month (8-40). According to grading, pain degree (from 8-9 pre operation to 3-4 post operation) and two point discrimination (from the mean of 14 mm (13-20 mm) to 8 mm (6-10 mm)) decreased. Grip power was increased from the mean of 10 kg to 21 kg. In 15 cases return of sensation, and in 13 cases improvement of opposition power was seen.
Conclusion:
We recommend epineurolysis for mild to moderate constriction and also end-to-end repair may be needed if extensive and severe constriction was found. It means that if we manage mild to moderate constriction sooner, it can prevent the need for further surgical procedure because of sever constriction.
Keywords: Carpal tunnel syndrome, hourglass constriction, median nerve
INTRODUCTION
Compression neuropathy of nerves is relatively common, but among the various etiologies of compressive lesions, the development of an hourglass-like constriction of the nerve that is unrelated to any recognizably compressive structure is a very rare phenomenon.[1] This problem has been reported previously for the radial nerve, posterior inter-osseous and anterior inter-osseous nerve. Nerve compressions often are caused by mechanical or dynamic compression of a nerve segment and they occur more frequently in the upper limb than in the lower limb,[1,2] the nerve compression is localized to regions where the nerve passes through the anatomically narrow tunnels. The nerve may be damaged by localized pressure or inflammation caused by surrounding tissue. Carpal tunnel syndrome most commonly caused by tenosynovitis of flexor, thickening of transverse carpal ligament. Among the various causes of compressive lesion, the development of an hourglass-like constriction of the nerve is a rare phenomenon. A review of the literature showed that this problem has been reported previously for the main trunk of the radial nerve,[2,3] and its branches posterior interosseous nerve[4,5] and for the anterior interosseous nerve (branch of median nerve).[6–8] Although, compression neuropathy of median nerve (CTS) is common but hourglass-like constriction is not common. At this study, we present severe cases of CTS that operated and hourglass-like constriction was seen.
METHODS
This case series study was conducted at Al-Zahra university hospital (Isfahan University of Medical Sciences) in between 1997 to 2005. Among 210 patients whom referred to hand clinic, 80 patients were evaluated for thenar atrophy, paresthesia of first, second and third finger, (advanced CTS).
Mean age of these patients was 58 years (46-85). Fifty two cases were female and 28 were males. Each patient was checked separately by clinical and Para clinical methods. In the prepared questionnaire was asked about pain severity ranged from 1-10, paresthesia pre and post operation and total satisfaction after surgery.
The physician examined two point discrimination and grip power, electro diagnostic study which revealed denervation signs in all the patients. Twenty two had diabetes, 17 heart disease, 5 rheumatoid arthritis, 8 old colles, all the patients were operated by classic approach.
Hourglass-like constriction at one point in ten cases, and area hourglass constriction in 6 cases were seen [Figure 1]. In all the cases, epineurotomy was performed. Distal of nerve was stimulated by nerve stimulator in all of them.
Figure 1.
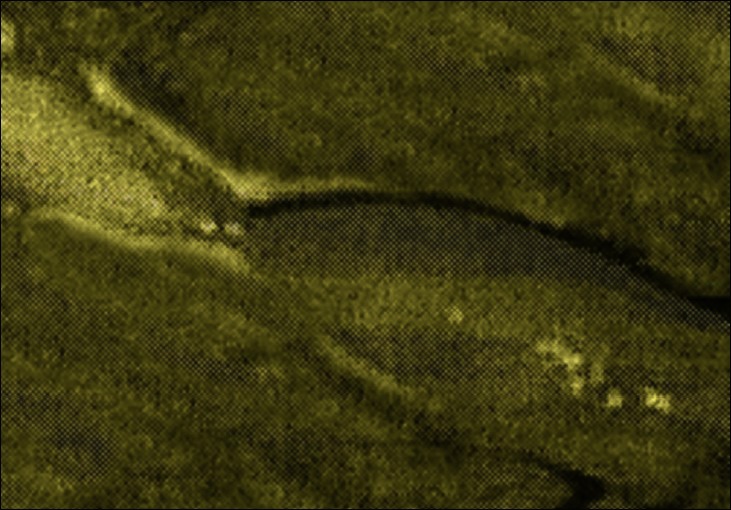
Hourglass like constriction
In two cases because of severe constriction and weak response to nerve stimulation, resection of lesion and end-to-end suture was performed [Figure 2]. After completing the operation short splint at 10 wrist extension was taken for 2 weeks.
Figure 2.
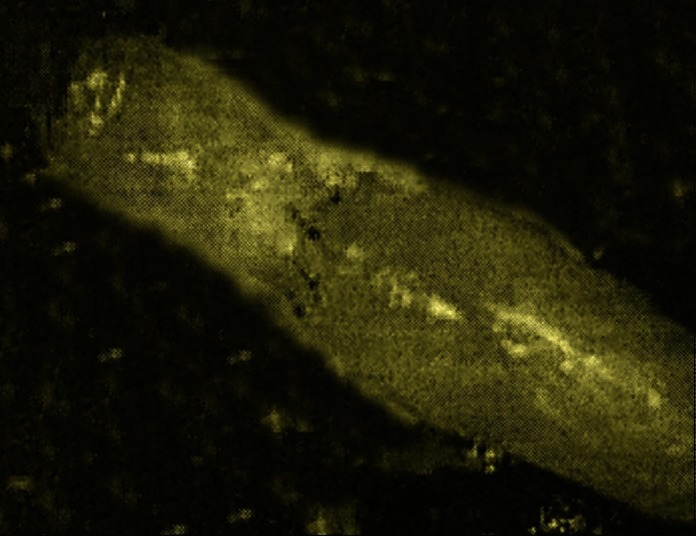
End-to-end repair
RESULTS
All patients have been examined periodically on 2nd, 4th, 8th and 12th weeks followed by 2 month intervals. Mean follow-up was 12 month (8-40).
According to the grading, pain severity decreased from 8-9 pre operation to 3-4 post operation (according to VAS questionnaire) (P < 0.05, in paired t-test). Tow point discrimination also decreased from the mean of 14 mm (13-20 mm) to 8 mm (6-10 mm), mean grip power increase was from 10 kg to 21 kg (P < 0.05, in paired t-test).
In 15 cases return of sensation and in 13 cases improvement of opposition was seen.
DISCUSSION
Compression neuropathy is a major cause of neural dysfunction. It is more frequent in the upper limb than lower limp, because of more mobility in upper limb compared with lower limb. Acute trauma and repetitive micro trauma can cause compression neuropathy.
Among the various causes of compressive lesions, the development of an hourglass constriction is rare. Wilhelm reported the first case in 1970.[9] He reported torsion of the deep branch of radial nerve without any visible source of external compression.
A consecutive lesion without external compression in radial nerve[2,3] posterior interosseous nerve,[4,5] anterior interosseous nerve,[6–8] and axillary nerve have been reported.[10–12]
For axillary nerve, the usual mechanisms of injury were reported as traction after fracture or dislocation or direct blow of shoulder,[12] the other cause of hourglass constriction was relegated to vascular network that changes nerve caliber. Hashizume et al., reported focal constriction secondary to vacuities in the perineurium in the posterior interosseous nerve paralysis.[13] The vascular cause might lead to intrafascicular edema. Chronic hypo perfusion is considered a possible cause of isolated nerve constriction and intra neural scarring. At this study, no above cause is found and it seems that chronic hypo perfusion due to chronic compression is the major cause of hourglass intra neural scarring? So prevention of intrafascicular edema and consequently hypo perfusion can prevent or at least decrease constriction of isolated nerve.
CONCLUSION
Although, hourglass constriction is uncommon but may be seen in severe chronic compressive neuropathy of median nerve that we recommend epineurolysis for mild to moderate constriction and end-to-end repair may be needed if extensive and severe constriction was found. It means that if we manage mild to moderate constriction sooner, it can prevent the need for further surgical procedure because of sever constriction.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Spinner M, Spinner RJ. Management of nerve compression lesions of the upper extremity. In: Omer GE, Spinner M, Van Beek AL, editors. Management of peripheral nerve problems. 2nd ed. Philadelphia: Saunders; 1998. pp. 527–8. [Google Scholar]
- 2.Yamamoto S, Nagano A, Mikami Y, Tajiri Y. Multiple constrictions of the radial nerve without external compression. J Hand Surg Am. 2000;25:134–7. doi: 10.1053/jhsu.2000.jhsu025a0134. [DOI] [PubMed] [Google Scholar]
- 3.Fernandez E, Di Rienzo A, Marchese E, Massimi L, Lauretti L, Pallini R. Radial nerve palsy caused by spontaneously occurring nerve torsion. Case report. J Neurosurg. 2001;94:627–9. doi: 10.3171/jns.2001.94.4.0627. [DOI] [PubMed] [Google Scholar]
- 4.Kotani H, Miki T, Senzoku F, Nakagawa Y, Ueo T. Posterior interosseous nerve paralysis with multiple constrictions. J Hand Surg Am. 1995;20:15–7. doi: 10.1016/S0363-5023(05)80049-8. [DOI] [PubMed] [Google Scholar]
- 5.Yongwei P, Guanglei T, Jianing W, Shuhuan W, Qingtai L, Wen T. Nontraumatic paralysis of the radial nerve with multiple constrictions. J Hand Surg Am. 2003;28:199–205. doi: 10.1053/jhsu.2003.50007. [DOI] [PubMed] [Google Scholar]
- 6.Nagano A, Shibata K, Tokimura H, Yamamoto S, Tajiri Y. Spontaneous anterior interosseous nerve palsy with hourglass-like fascicular constriction within the main trunk of the median nerve. J Hand Surg Am. 1996;21:266–70. doi: 10.1016/S0363-5023(96)80114-6. [DOI] [PubMed] [Google Scholar]
- 7.Yamamoto S, Nagano A, Mikami Y, Tajiri Y, Kawano K, Ltaka K. Fascicular constriction in the anterior interosseous nerve and other motor branches of the median nerve. Muscle Nerve. 1999;22:547–8. doi: 10.1002/(sici)1097-4598(199904)22:4<547::aid-mus26>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- 8.Yasunaga H, Shiroishi T, Ohta K, Matsunaga H, Ota Y. Fascicular torsion in the median nerve within the distal third of the upper arm: Three cases of nontraumatic anterior interosseous nerve palsy. J Hand Surg Am. 2003;28:206–11. doi: 10.1053/jhsu.2003.50021. [DOI] [PubMed] [Google Scholar]
- 9.Wilhelm A. Radial nerve compression. Handchirurgie. 1976;8:113–6. [PubMed] [Google Scholar]
- 10.Perlmutter GS. Axillary nerve injury. Clin Orthop Relat Res. 1999;368:28–36. [PubMed] [Google Scholar]
- 11.Visser CP, Coene LN, Brand R, Tavy DL. The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery. A prospective clinical and EMG study. J Bone Joint Surg Br. 1999;81:679–85. doi: 10.1302/0301-620x.81b4.9005. [DOI] [PubMed] [Google Scholar]
- 12.Oberlin C, Shafi M, Diverres JP, Silberman O, Adle H, Belkheyar Z. Hourglass-like constriction of the axillary nerve: Report of two patients. J Hand Surg Am. 2006;31:1100–4. doi: 10.1016/j.jhsa.2006.03.007. [DOI] [PubMed] [Google Scholar]
- 13.Hashizume H, Inoue H, Nagashima K, Hamaya K. Posterior interosseous nerve paralysis related to focal radial nerve constriction secondary to vasculitis. J Hand Surg Br. 1993;18:757–60. doi: 10.1016/0266-7681(93)90239-c. [DOI] [PubMed] [Google Scholar]