

Abstract
Recent studies indicate that multiple bone morphogenetic protein (BMP) family ligands and receptors are involved in the development of pulmonary arterial hypertension, yet the underlying mechanisms are incompletely understood. Although BMP2 and BMP4 share high homology in amino acid sequence, they appear to exert divergent effects on chronic hypoxic pulmonary hypertension (CHPH). While BMP4 promotes vascular remodeling, BMP2 prevents CHPH. We previously demonstrated that BMP4 upregulates the expression of canonical transient receptor potential channel (TRPC) proteins and, thereby, enhances store-operated Ca2+ entry (SOCE) and elevates intracellular Ca2+ concentration ([Ca2+]i) in pulmonary arterial smooth muscle cells (PASMCs). In this study, we investigated the effects of BMP2 on these variables in rat distal PASMCs. We found that treatment with BMP2 (50 ng/ml, 60 h) inhibited TRPC1, TRPC4, and TRPC6 mRNA and protein expression. Moreover, BMP2 treatment led to reduced SOCE and decreased basal [Ca2+]i in PASMCs. These alterations were associated with decreased PASMC proliferation and migration. Conversely, knockdown of BMP2 with specific small interference RNA resulted in increased cellular levels of TRPC1, TRPC4, and TRPC6 mRNA and protein, enhanced SOCE, elevated basal [Ca2+]i, and increased proliferation and migration of PASMCs. Together, these results indicate that BMP2 participates in regulating Ca2+ signaling in PASMCs by inhibiting TRPC1, TRPC4, and TRPC6 expression, thus leading to reduced SOCE and basal [Ca2+]i and inhibition of cell proliferation and migration.
Keywords: BMP2, transient receptor potential canonical, calcium signaling, pulmonary arterial smooth muscle cells
pulmonary arterial (PA) hypertension (PAH) is a rare disease with poor prognosis. It is defined by sustained elevation of PA pressure, which eventually causes right ventricular failure and death. The pathogenesis of PAH is characterized by persistent vasoconstriction and structural remodeling of the pulmonary vasculature; however, the mechanisms underlying these changes are incompletely understood.
Among numerous molecules that have been discovered to explain the pathobiology of PAH, accumulating evidence indicates that a change in intracellular Ca2+ concentration ([Ca2+]i) is a key signal in the regulation of contraction, proliferation, and migration of PA smooth muscle cells (PASMCs) (6, 7, 16, 17, 27). Store-operated Ca2+ channels (SOCCs) mediated Ca2+ entry, the so-called store-operated Ca2+ entry (SOCE) is an important approach in maintenance of [Ca2+]i homeostasis in various cell types, including PASMCs (31, 35, 38, 45). We and others recently found that enhanced SOCE is responsible for the hypoxia-induced increase in [Ca2+]i in PASMCs (21, 24, 42, 44). SOCCs are believed to be composed of canonical transient receptor potential (TRPC) channel proteins (9, 32). Previously, we found that TRPC1, TRPC4, and TRPC6 are the predominant TRPCs expressed in distal PAs and PASMCs (25, 42, 53). Moreover, it appears that TRPC1 and TRPC6 are specifically upregulated by hypoxia and contribute to the hypoxia-induced increases in SOCE and basal [Ca2+]i in PASMCs (46).
Loss-of-function mutation of bone morphogenetic protein (BMP) type II receptor was found in a majority of patients with idiopathic PAH (26), suggesting that the signaling of BMP plays an important role in PAH. BMP type II receptor belongs to the transforming growth factor-β superfamily of receptors and transduces signal upon binding to BMP ligands, i.e., BMP2 and BMP4 (27, 29). Recently, considerable efforts have been made to elucidate the role and mechanisms of aberrant BMP signaling in PAH. BMP2 and BMP4 were reported to be upregulated in the lung under hypoxia. Although the two proteins share high homology in amino acid sequence, they appear to play opposite roles in the development of chronic hypoxic pulmonary hypertension (CHPH) (13). While mice with partial deficiency of BMP4 were protected from pulmonary vascular remodeling and development of CHPH, Bmp2+/− mice were prone to develop a severe form of this disease (1, 13). It is unknown what led to these differences. We recently found that BMP4 upregulated TRPC1, TRPC4, and TRPC6 expression and functionally increased SOCE and basal [Ca2+]i in PASMCs (23). In this study, we investigated the effects of BMP2 on these parameters, as well as proliferation and migration of rat distal PASMCs.
MATERIALS AND METHODS
Cell isolation and culture.
Animal protocols were approved by the Animal Care and Use Committee of the Johns Hopkins Medical Institutions. Male Wistar rats (300–500 g body wt) were anesthetized with pentobarbital sodium (65 mg/kg ip), as previously described (36, 37, 42), and the distal intrapulmonary arteries (>4th generation) were dissected from lungs in HBSS (130 mM NaCl, 5 mM KCl, 1 mM MgCl2, 10 mM HEPES, and glucose, with pH adjusted to 7.2 with 5 mM NaOH). Ca2+ was added to a concentration of 1.5 mM. The thin layer of adventitia was carefully stripped off with forceps, and the lumina were gently swiped using a cotton swab to remove endothelium. Distal PASMCs were obtained from the isolated PA enzymatically, plated onto 25-mm coverslips in six-well dishes, and cultured for 3–6 days in smooth muscle growth medium (SMGM-2, Clonetics, Walkersville, MD) with 5% serum in a humidified atmosphere of 5% CO2-95% air at 37°C. Cellular purity was >98% when assessed by morphological appearance under phase-contrast microscopy and by immunofluorescence staining for α-actin under confocal microscopy, as previously described (42).
BMP2 treatment.
Distal PASMCs at 50–70% confluence were growth-arrested in smooth muscle basal medium (SMBM; Clonetics) containing 0.3% FBS for 24 h and then treated with 5–200 ng/ml recombinant human BMP2 (R & D Systems, Minneapolis, MN) for 24, 48, or 60 h. These treated cells were subjected to Ca2+ assays or gene expression measurements.
Small interference RNA transfection.
Small interference RNA (siRNA) siGENOME SMARTpool targeting to BMP2 mRNA (National Center for Biotechnology Information GenBank accession number NM_017178) and the nontargeting (NT) control siRNA pool (NT siRNA) were purchased from Dharmacon (Lafayette, CO). Rat distal PASMCs grown in SMGM-2 were transfected with 20 nM siRNA for 6 h in serum-free SMBM using GeneSilencer (Genlantis, San Diego, CA) according to the manufacturer's instructions, cultured for 18 h in SMBM containing 5% FBS, subjected to migration and proliferation assays, or cultured for 42 h in SMBM containing 0.3% FBS, and then subjected to gene expression, [Ca2+]i, and Ca2+ influx measurements.
RNA extraction and real-time quantitative PCR.
As previously described (23), total RNA in distal PASMCs was extracted using an RNeasy kit (Qiagen, Valencia, CA). Reverse transcription was performed using an iScript cDNA synthesis kit (Bio-Rad, Hercules, CA). Real-time PCR was performed using an iCycler IQ system (Bio-Rad). Primer sequences specific for rat TRPC1, TRPC4, TRPC6, BMP2, BMP4, and cyclophilin B are listed in Table 1 (23). Relative concentration of each transcript was calculated using the Pfaffl method. TRPC and BMP mRNA copies were normalized to cyclophilin B and expressed as percent change from control values.
Table 1.
Real-time quantitative PCR primers for rat TRPC1, TRPC4, TRPC6, BMP2, BMP4, and cyclophilin B
| Gene | Accession No. | Primer Sequence | Product Size, bp | Location in Sequence |
|---|---|---|---|---|
| TRPC1 | NM_053558 | Left: 5′-AGCCTCTTGACAAACGAGGA-3′ Right: 5′-ACCTGACATCTGTCCGAACC-3′ | 146 | 797–942 |
| TRPC4 | NM_080396 | Left: 5′-GACACGGAGTTCCAGAGAGC-3′ Right: 5′-GTTGGGCTGAGCAACAAACT-3′ | 142 | 777–918 |
| TRPC6 | NM_053559 | Left: 5′-TACTGGTGTGCTCCTTGCAG-3′ Right: 5′-GAGCTTGGTGCCTTCAAATC-3′ | 141 | 1267–1407 |
| BMP2 | NM_017178 | Left: 5′-AAGCGTCAAGCCAAACACAAAC-3′ Right: 5′-GCCACGATCCAGTCATTCCAC-3′ | 107 | 896–1002 |
| BMP4 | NM_012827 | Left: 5′-CAGAGCCAACACTGTGAGGA-3′ Right: 5′-GGGATGCTGCTGAGGTTAAA-3′ | 108 | 477–584 |
| Cyclophilin B | NM_022536 | Left: 5′-GGACGAGTGACCTTTGGACT-3′ Right: 5′-TGACACGATGGAACTTGCTG-3′ | 118 | 170–287 |
TRPC, canonical transient receptor potential; BMP, bone morphogenetic protein.
Western blot analysis.
Distal PASMCs were washed with PBS, and protein was extracted with ice-cold lysis buffer (T-PER buffer, Pierce, Rockford, IL) supplemented with proteinase inhibitors. The amount of cell lysate protein was determined using bicinchoninic acid protein assay (Pierce). Proteins were separated on 8% SDS-PAGE (Bio-Rad), transferred onto polyvinylidene difluoride membranes (Bio-Rad), and probed with affinity-purified rabbit polyclonal antibodies specific for TRPC proteins (Alomone Laboratories, Jerusalem, Israel) or mouse monoclonal antibodies to β-actin (Sigma, St. Louis, MO). The secondary antibodies were horseradish peroxidase-conjugated anti-rabbit or anti-mouse IgG (Kirkegaard and Perry Laboratories, Gaithersburg, MD). Protein bands were detected by enhanced chemiluminescence (GE Healthcare, Piscataway, NJ).
Measurement of [Ca2+]i.
As we described previously (42), coverslips with PASMCs were loaded with 7.5 μM fura 2-AM (Invitrogen, Grand Island, NY) and incubated for 60 min at 37°C under 5% CO2-95% air, and each was mounted in a closed polycarbonate chamber clamped in a heated aluminum platform (model PH-2, Warner Instruments, Hamden, CT) on the stage of an inverted microscope (TSE 100 Ellipse, Nikon, Melville, NY). Cells were perfused at 1 ml/min with Krebs-Ringer bicarbonate solution (KRBS), which consisted of (in mM) 118 NaCl, 4.7 KCl, 2.5 CaCl2, 0.57 MgSO2, 1.18 KH2PO4, 25 NaHCO3, and 10 glucose, was equilibrated in heated reservoirs with 5% CO2 and 16% O2, and was led to the chamber through stainless steel tubing. An in-line heat exchanger and dual-channel heater controller (models SF-28 and TC-344B, Warner Instruments) were used to maintain chamber temperature at 37°C. After 10 min of perfusion to eliminate extracellular dye, [Ca2+]i was determined by fura 2 fluorescence emitted at 510 nm after excitation at 340 and 380 nm (F340 and F380) at 12- to 30-s intervals with a xenon arc lamp, interference filters, an electronic shutter, a ×20 fluorescence objective, and a cooled charge-coupled device imaging camera. Data were collected and analyzed with InCyte software (Intracellular Imaging, Cincinnati, OH). Ca2+ levels are presented as an average from 20–30 cells.
Measurement of SOCE.
PASMCs were perfused for ≥10 min with Ca2+-free KRBS containing 1 mM EGTA to chelate residual Ca2+, 5 μM nifedipine (Sigma-Aldrich, St. Louis, MO) to prevent Ca2+ entry through L-type voltage-dependent Ca2+ channels, and 10 μM cyclopiazonic acid (CPA; Sigma-Aldrich) to deplete sarcoplasmic reticulum Ca2+ stores. SOCE was assessed in two ways, as described previously (25, 42). 1) [Ca2+]i was measured before and after restoration of extracellular [Ca2+] to 2.5 mM, and SOCE was evaluated from the peak increase in [Ca2+]i caused by restoration of extracellular Ca2+ in the continued presence of nifedipine and CPA. 2) Fura 2 fluorescence excited at 360 nm at 30-s intervals was monitored before and after addition of MnCl2 (200 μM) to the cell perfusate, and SOCE was evaluated from the rate at which fura 2 fluorescence was quenched by Mn2+, which entered the cell as a Ca2+ surrogate and reduced fura 2 fluorescence upon binding to the dye.
Assessment of PASMC migration.
Migration of PASMCs was assessed using Transwell polycarbonate inserts (8-μm membrane pore size; Corning, Lowell, MA). PASMCs were treated with BMP2 (50 ng/ml) for 60 h, trypsinized, and added to the membrane (8 × 104 cells/insert). After incubation for 24 h, cells were fixed using 95% freezing-cold ethanol for 10 min, stained with Brilliant Blue R staining solution (Sigma) for 5 min, and washed with PBS. The stained cells were imaged under an inverted microscope at five fixed positions of the Transwell membrane (top right, top left, bottom right, bottom left, and central field) and counted to represent the total cells. Then the cells on the upper surface of the membrane inserts were gently wiped off with cotton swabs. Images for cell migration on the lower surface of membrane were obtained at the five positions used for total cell imaging. Cell migration was calculated as the ratio of migrated cells to total cells on each membrane.
Cell proliferation assay.
Proliferation of PASMCs was determined by the Cell Proliferation Biotrak ELISA Kit (GE Healthcare) according to the manufacturer's protocol. Briefly, PASMCs were seeded onto 96-well plates in 0.3% FBS-SMBM at a density of 5 × 103 cells/well, cultured with or without BMP2 (50 ng/ml) for 72 h, and labeled with bromodeoxyuridine for 24 h. Then the cells were successively fixed, blocked, probed with anti-bromodeoxyuridine, and developed with tetramethylbenzidine substrate, and the reaction was stopped with sulfuric acid. The optical density of each well was determined using a microplate reader (Bio-Rad) at 450 nm.
Drugs and materials.
Unless otherwise specified, all reagents were obtained from Sigma-Aldrich. The stock solutions of recombinant human BMP2 at 50 μg/ml were made in 4 mM HCl containing 0.1% BSA. Stock solutions of 30 mM CPA and 5 mM nifedipine were made in DMSO, and 200 mM MnCl2 was dissolved in deionized water. Fura 2-AM was prepared before the experiment as a 2.5 mM stock solution in DMSO containing 20% Pluronic F-127 (Invitrogen).
Statistical analyses.
Values are means ± SE. Statistical analyses were performed using unpaired and paired Student's t-tests or ANOVA. Differences were considered significant when P < 0.05.
RESULTS
BMP2 inhibited TRPC expression in distal PASMCs.
Treatment with BMP2 at 5, 10, 50, 100, or 200 ng/ml for 60 h dose-dependently reduced the mRNA expression of TRPC1, TRPC4, and TRPC6 in distal PASMCs compared with control cells (Fig. 1A). These reductions reached significance at 50 ng/ml BMP2. Raising the dosage of BMP2 to 100 and 200 ng/ml did not further inhibit the levels of the three TRPC transcripts; therefore, the optimal dosage of BMP2 for maximal inhibition was considered to be 50 ng/ml. Treatment with 50 ng/ml BMP2 decreased mRNA expression of TRPC1, TRPC4, and TRPC6 by 32.2%, 36.9%, and 36.5%, respectively (Fig. 1A).
Fig. 1.

A: expression of canonical transient receptor potential (TRPC) mRNA relative to cyclophilin B in distal pulmonary arterial smooth muscle cells (PASMCs) treated with bone morphogenetic protein (BMP) 2 (5, 10, 50, 100, or 200 ng/ml) or vehicle (control; 4 mM HCl with 0.1% BSA) for 60 h as determined by real-time quantitative PCR. Values are means ± SE (n = 4 in each group). *P < 0.05 vs. control. B: expression of TRPC mRNA relative to cyclophilin B in distal PASMCs treated with 50 ng/ml BMP2 or vehicle (control) for 24, 48, or 60 h as determined by real-time quantitative PCR. Values are means ± SE (n = 3 in each group). *P < 0.05 vs. control.
Time-course study at 24, 48, and 60 h indicated that the most drastic decreases of TRPC mRNA expression by 50 ng/ml BMP2 treatment were at 60 h (Fig. 1B). Western blotting confirmed that BMP2 treatment (50 ng/ml, 60 h) also decreased the protein expression of TRPC1, TRPC4, and TRPC6 by 32.3%, 37.0%, and 30.5%, respectively, in distal PASMCs (Fig. 2).
Fig. 2.

Top: representative Western blots for TRPC1, TRPC4, and TRPC6 in distal PASMCs treated with 50 ng/ml BMP2 or vehicle for 60 h. Bottom: mean protein expression for TRPC1, TRPC4, and TRPC6 relative to β-actin. Values are means ± SE (n = 4 in each group). *P < 0.05 vs. control.
BMP2 reduced SOCE in distal PASMCs.
SOCE was assessed in two ways: Ca2+ restoration and Mn2+ quenching. In the Ca2+ restoration assessment, CPA given in the absence of extracellular Ca2+ and in the presence of nifedipine caused an initial transient increase in [Ca2+]i, indicating no difference in Ca2+ release between control PASMCs and cells treated with BMP2 (50 ng/ml for 60 h). Subsequent restoration of extracellular Ca2+ induced a second increase in [Ca2+]i, which quickly achieved a peak change in [Ca2+]i of 264.1 ± 21.2 nM (n = 3) in BMP2-treated PASMCs; this peak change in [Ca2+]i was smaller, indicating a smaller SOCE in BMP2-treated cells than in vehicle-treated control cells (Δ[Ca2+]i = 371.3 ± 28.1 nM, n = 3, P < 0.05; Fig. 3A). Mn2+ quenching, which is measured as the rate at which Mn2+ quenches fura 2 fluorescence, is thought to be a more specific index of Ca2+ influx. SOCE assessed by Mn2+ quenching and expressed as the percent decrease from fluorescence at 10 min to fluorescence at time 0 was also smaller in BMP2-treated distal PASMCs than in vehicle-treated control cells (33.3 ± 2.2% vs. 43.4 ± 1.9%, n = 3, P < 0.05; Fig. 3B).
Fig. 3.

A: response of intracellular Ca2+ concentration ([Ca2+]i) to restoration of extracellular Ca2+ to 2.5 mM after perfusion with Ca2+-free Krebs-Ringer bicarbonate solution (KRBS, 0 Ca2+) containing cyclopiazonic acid (CPA, 10 μM), nifedipine (Nif, 5 μM), and EGTA (1 mM) in rat distal PASMCs treated with BMP2 (n = 3 experiments in 86 cells) or vehicle (n = 3 experiments in 88 cells) for 60 h. Right: maximum increase in [Ca2+]i after restoration of extracellular Ca2+ was smaller in BMP2-treated PASMCs than in control cells. Values are means ± SE. *P < 0.05. B: time course of quenching of fura 2-AM fluorescence at 360 nm by 200 μM Mn2+ after perfusion with Ca2+-free KRBS (0 Ca2+) containing nifedipine (5 μM) and CPA (10 μM) in distal PASMCs treated with 50 ng/ml BMP2 (n = 3 experiments in 84 cells) or vehicle control for 60 h normalized to fluorescence at time 0 (F/F0). Right: Mn2+ quenching, expressed as percent decrease in fluorescence at 10 min from time 0, was greater in control cells than in BMP2-treated distal PASMCs. Values are means ± SE. *P < 0.05. C: changes in basal [Ca2+]i in distal PASMCs treated with 50 ng/ml BMP2 for 60 h. Values are means ± SE (n = 4 experiments in 120 cells). *P < 0.05 vs. control.
BMP2 decreased basal [Ca2+]i in distal PASMCs.
Basal [Ca2+]i was decreased from 76.43 ± 8.19 nM (n = 4) in control cells exposed to vehicle to 54.09 ± 2.22 nM (n = 4) in distal PASMCs treated with 50 ng/ml BMP2 for 60 h (P < 0.05; Fig. 3C).
BMP2 inhibited migration and proliferation of PASMCs.
Treatment with BMP2 (50 ng/ml for 60 h) caused inhibition of proliferation and migration of PASMCs. Proliferation was decreased 18.7% compared with control (P < 0.05; Fig. 4A), whereas migration was decreased 21.6% (P < 0.05; Fig. 4B) in BMP2-treated cells.
Fig. 4.

A: changes in proliferation of distal PASMCs treated with 50 ng/ml BMP2 for 60 h. Values are means ± SE (n = 4). *P < 0.05 vs. control. B: changes in migration of distal PASMCs treated with 50 ng/ml BMP2 for 60 h. Values are means ± SE (n = 4). *P < 0.05 vs. control.
Knockdown of BMP2 enhanced TRPC expression, SOCE, and basal [Ca2+]i and increased proliferation and migration of distal PASMCs.
To verify the above-mentioned effects of BMP2 in PASMCs, we further used siRNA targeted to BMP2 (BMP2 siRNA) to knock down BMP2 expression in the culture. As seen in Fig. 5A, exposure of PASMCs to BMP2 siRNA resulted in a 89.1% decrease of BMP2 mRNA compared with that in NT siRNA-treated control cells. Under this condition, the amount of BMP2 protein in the conditioned medium of PASMC culture was decreased 85.9% (Fig. 5B). The specificity of BMP2 siRNA was verified by determining the mRNA (Fig. 5A) and protein (Fig. 5B) levels of BMP4 in PASMC culture, which were not altered by BMP2 siRNA treatment. Next, we examined the effects of decreased BMP2 on TRPC expression and the subsequent functional influences on SOCE and basal [Ca2+]i in rat distal PASMCs. Knockdown of BMP2 caused significant increases of mRNA (Fig. 5C) and protein (Fig. 5D) expression of TRPC1, TRPC4, and TRPC6 compared with NT siRNA-exposed cells. Consequently, restoration of extracellular Ca2+ led to a peak change in [Ca2+]i of 527.2.1 ± 68.1 nM (n = 3) in PASMCs treated with BMP2 siRNA; this peak change in [Ca2+]i was greater than that measured in NT siRNA-treated cells (Δ[Ca2+]i = 385.5 ± 31.3 nM, n = 3, P < 0.05; Fig. 6A). SOCE assessed by Mn2+ quenching was increased ∼14.8% by BMP2 siRNA treatment (P < 0.05 vs. NT siRNA treatment; Fig. 6B). Basal [Ca2+]i was increased from 68.53 ± 6.28 nM in control cells exposed to NT siRNA to 85.78 ± 5.95 nM in PASMCs treated with BMP2 siRNA (P < 0.05; Fig. 6C). Moreover, as indicated in Fig. 7, knockdown of BMP2 caused increases in proliferation and migration of PASMCs (Fig. 7) compared with cells treated with NT siRNA.
Fig. 5.
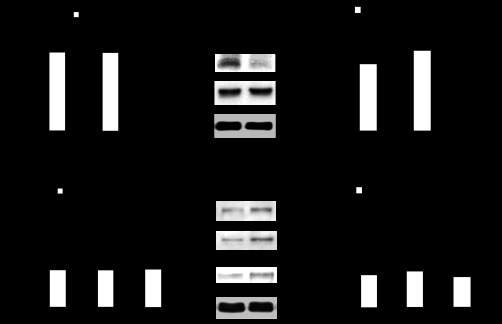
A: BMP2 and BMP4 mRNA relative to cyclophilin B as determined by real-time quantitative PCR in PASMCs treated with BMP2 small interference (si) RNA or nontargeting (NT) control siRNA. Values are means ± SE (n = 3 for each group). *P < 0.05 vs. NT siRNA. B: representative Western blots of secreted BMP2 and BMP4 protein in conditioned media from PASMC cultures treated with BMP2 siRNA or NT control siRNA (left) and mean protein levels of secreted BMP2 and BMP4 relative to β-actin in cells from each PASMC culture (right). Values are means ± SE (n = 3 for each group). *P < 0.05 vs. NT siRNA. C: TRPC1, TRPC4, and TRPC6 mRNA relative to cyclophilin B as determined by real-time quantitative PCR in PASMCs treated with BMP2 siRNA or NT control siRNA. Values are means ± SE (n = 3 for each group). *P < 0.05 vs. NT siRNA. D: representative Western blots of TRPC1, TRPC4, and TRPC6 protein in PASMCs treated with BMP2 siRNA or NT control siRNA (left) and mean protein expression for TRPC1, TRPC4, and TRPC6 relative to β-actin (right). Values are means ± SE (n = 3 for each group). *P < 0.05 vs. NT siRNA.
Fig. 6.

A: [Ca2+]i responses to restoration of extracellular [Ca2+] to 2.5 mM after perfusion with Ca2+-free KRBS (0 Ca2+) containing CPA (10 μM), nifedipine (5 μM), and EGTA (1 mM) in rat distal PASMCs treated with BMP2 siRNA (n = 3 experiments in 83 cells) or NT siRNA (n = 3 experiments in 85 cells) (left). Right: maximum increase in [Ca2+]i after restoration of extracellular [Ca2+] was enhanced in BMP2 siRNA-treated PASMCs compared NT siRNA-treated cells. Values are means ± SE. *P < 0.01. B: time course of quenching of fura 2-AM fluorescence at 360 nm by 200 μM Mn2+ after perfusion with Ca2+-free KRBS (0 Ca2+) containing nifedipine (5 μM) and CPA (10 μM) in rat distal PASMCs treated with BMP2 siRNA (n = 3 experiments in 86 cells) or NT siRNA (n = 3 experiments in 82 cells) normalized to fluorescence at time 0 (left). Right: Mn2+ quenching, expressed as percent increase in fluorescence from time 0, was reduced in BMP2 siRNA-treated PASMCs compared with NT siRNA-treated cells. Values are means ± SE. *P < 0.05. C: changes in basal [Ca2+]i in distal PASMCs treated with BMP2 siRNA (n = 3 from 88 cells). Values are means ± SE. *P < 0.05 vs. NT siRNA (n = 3 from 87 cells).
Fig. 7.

A: cell proliferation was increased in BMP2 siRNA-treated PASMCs compared with NT siRNA-treated cells. Values are means ± SE (n = 4). *P < 0.05 vs. NT siRNA. B: cell migration was increased in BMP2 siRNA-treated PASMCs compared with NT siRNA-treated cells. Values are means ± SE (n = 4). *P < 0.05 vs. NT siRNA.
Expression of BMP2 and BMP4 in distal PA and PASMCs.
To examine the differences of BMP2 and BMP4 expression levels in distal PAs and PASMCs, we used real-time PCR to measure BMP2 and BMP4 mRNA. As seen in Fig. 8, BMP2 mRNA is much less abundant than BMP4 mRNA in distal PAs (P < 0.05; Fig. 8A) and PASMCs (P < 0.05; Fig. 8B).
Fig. 8.

Expression of BMP2 and BMP4 mRNA normalized to cyclophilin B in distal pulmonary artery (PA; A) and PASMCs (B) as determined by real-time quantitative PCR. Values are means ± SE (n = 4). *P < 0.05.
DISCUSSION
The present study provides evidence indicating that BMP2 regulates Ca2+ signaling in PASMCs. BMP2 treatment 1) inhibited TRPC1, TRPC4, and TRPC6 expression in PASMCs, 2) reduced SOCE and basal [Ca2+]i in PASMCs, and 3) inhibited proliferation and migration of PASMCs. In addition, knockdown of BMP2 by siRNA enhanced mRNA and protein expression of TRPC1, TRPC4, and TRPC6, which were associated with increased SOCE, basal [Ca2+]i, and proliferation and migration of PASMCs.
Of the seven members of the TRPC family that have been identified (28), TRPC1, TRPC4, and TRPC6 are the predominant members expressed in PASMCs (25). It is conceivable that TRPC1 and TRPC4 primarily form SOCCs, which provide a pathway for SOCE, thus participating in regulation of [Ca2+]i in various cell types, including PASMCs (3, 34). Knockdown of TRPC1 by its specific siRNA suppressed SOCE in rat PASMCs (21, 24). Antisense oligonucleotides targeted to TRPC1 reduced TRPC1 gene expression and reduced SOCE in human PASMCs (39). Anti-TRPC1 antibody treatment attenuated SOCC activity, resulting in decreased SOCE and SOCC-mediated contraction of rat caudal artery (4, 5, 47). Conversely, overexpression of human TRPC1 enhanced the contractile responses of rat PA rings to CPA (20). In the vasculature, TRPC4 is thought to be mainly expressed by endothelial cells; however, it is also found to contribute to ATP-induced cell mitogenesis in PASMCs by forming SOCCs and increasing SOCE (52). TRPC6 is usually considered to form receptor-operated Ca2+ channels (ROCCs), because it could be activated by diacylglycerol (DAG) and other signaling messengers involved in the G protein pathway. Knockdown of TRPC6 by its siRNA decreased DAG-induced cation influx in rat PASMCs (21). Inhibition of DAG kinase by its inhibitor R-59949 caused sarcolemmal accumulation of DAG in PASMCs isolated from wild-type and Trpc6−/− mice; however, this increased [Ca2+]i in cells from wild-type, but not Trpc6−/−, mice (46). It is also believed that TRPC6 can assemble into SOCCs according to the following evidence. 1) Upregulated TRPC6 was associated with increased SOCE in proliferative PASMCs, whereas inhibition of TRPC6 expression with antisense oligonucleotides or bosentan reduced SOCE induced by passive store depletion and attenuated mitogen-mediated PASMC proliferation (19, 49, 50). 2) Knockdown of TRPC6 by siRNA decreased SOCE, as well as the proliferation rate of human hepatoma cells (10). 3) We previously demonstrated that TRPC6 could form functional SOCC in rat distal PASMCs, because knockdown of TRPC6 expression by siRNA reduced the hypoxia-induced increases in SOCE (24). It is likely that TRPC6, as one of the subunits in the homo- or heterotetrameric TRP pore complex, participates in formation of SOCCs and ROCCs; the preference for TRPC6 to form SOCCs or ROCCs may be dependent on the cellular host environment, as well as the cell phenotype, and may be determined by the interactions with auxiliary proteins such as adaptors, scaffolds, and regulators (33).
If TRPC1, TRPC4, and TRPC6 or any one of these TRPCs are present in SOCCs in PASMCs, the decreased expression level of these Ca2+ channel proteins could lead to fewer SOCCs and reduced SOCE in distal PASMCs treated with BMP2. To verify this presumption, we determined whether treatment with BMP2 altered SOCE in distal PASMCs. Using Ca2+ restoration and Mn2+ quenching techniques, we found that SOCE was lower in BMP2-treated than control cells, indicating a functional influence of BMP2 on Ca2+ signaling in PASMCs.
In addition to SOCE, changes in TRPC expression are often associated with an altered basal level of cellular [Ca2+]i as a result of reduced SOCE (8, 42, 43, 52). PASMCs exposed to growth factors (i.e., serum, platelet-derived growth factor, or BMP4) or stimuli (i.e., ATP or chronic hypoxia) exhibit increased basal [Ca2+]i in conjunction with increased expression of TRPC1, TRPC4, or TRPC6 (14, 21, 23, 44, 50, 52). Some drugs, such as bosentan, sildenafil, and tanshinone IIA sulfonate, show therapeutic efficacy for PAH, in which downregulation of TRPC1, TRPC4, or TRPC6 expression may be involved (19, 24, 41). Additionally, our previous studies found that increased [Ca2+]i caused by hypoxia in PASMCs was blocked by the SOCC antagonists (43) and that knockdown of TRPC1 or TRPC6 attenuated the hypoxia-induced increases in SOCE and basal [Ca2+]i, suggesting a cause-and-effect link between increases in TRPC1 and TRPC6 expression and the hypoxia-induced increases in SOCE and basal [Ca2+]i (24). In this study, we further demonstrated that BMP2 decreased basal [Ca2+]i in distal PASMCs. According to the above-mentioned findings from the literature and our data, it is reasonable to speculate that the basal [Ca2+]i is regulated by TRPC-mediated SOCE and that the decreased basal [Ca2+]i in BMP2-treated PASMCs was caused by the decreased expression of TRPC1, TRPC4, and TRPC6.
The increased proliferation and migration of PASMCs have been considered to be critical pathobiological changes in pulmonary vascular remodeling and PAH development. Accumulating evidence indicates that [Ca2+]i is a central factor in regulating pulmonary vascular hypertrophy by stimulating PASMC proliferation and migration (6, 12, 15, 34). Changes in TRPC expression level and SOCE activity correlated with altered proliferation of PASMCs as a result of altered [Ca2+]i (2, 14, 18, 39). Downregulated expression of TRPC1 decreased amplitudes of SOCE and attenuated proliferation of PASMCs (39). In contrast, enhanced expression of TRPC1 and increased SOCE were found in proliferating PASMCs (14). The TRPC blocker SKF-96365 or repression of TRPC1 expression by siRNAs or by a short hairpin RNA reduced the speed of cell migration (22). These findings indicate that TRPCs are directly linked to cell proliferation and migration. Consequently, we found that BMP2 inhibited the proliferation and migration of distal PASMCs. This result is consistent with a previous report showing inhibition of BMP2 upon proliferation of normal human PASMCs (51). Finally, the inhibitory effects of BMP2 treatment were confirmed by knockdown of endogenous BMP2 expression by specific siRNA, which resulted in increased cell proliferation and migration, in association with increased expression of TRPC1, TRPC4, and TRPC6 and enhanced SOCE and basal [Ca2+]i in distal PASMCs.
Aside from the action on TRPC expression, BMP2 may also regulate Ca2+ signaling by increasing voltage-gated K+ channel protein (i.e., KV1.5) expression in PASMCs, resulting in a decrease in L-type voltage-dependent Ca2+ currents and an increase in cell apoptosis (48, 51). Together, the inhibitory effects of BMP2 on basal [Ca2+]i and PASMC proliferation and migration suggest a potential therapeutic application of this protein in PAH treatment. However, BMP2 also showed divergent effects on PASMCs from normal individuals and patients with pulmonary hypertension. While a panel of genes relating to cell growth and contraction were downregulated by BMP2 in normal PASMCs, these same genes were upregulated in cells from patients with idiopathic PAH (11). Moreover, BMP2-induced apoptosis in normal PASMCs was reduced in cells from patients with secondary pulmonary hypertension (48, 51). Therefore, it seems that the differential effects of BMP2 on gene expression in PASMCs from normal individuals and patients with pulmonary hypertension may account for the transition of BMP2 from an antiproliferative to a proliferative factor in pulmonary hypertension. Consequently, caution should be exercised when suggesting use of BMP2 as a therapeutic strategy for PAH.
The amino acid sequence of the secreted mature protein of human BMP2 (UniProtKB/Swiss-Prot accession no. P12343) is highly similar to that of BMP4 (P12644), with 87.8% homology. Interestingly, these two proteins show divergent effects on CHPH development. In chronic hypoxia, increased BMP4 expression enhanced proliferation and migration of pulmonary vascular smooth muscle cells, and partial deficiency of BMP4 in BMP4 heterozygous-mutant mice protected the mice from vascular remodeling and pulmonary vascular systolic pressure increment (13). Unlike BMP4-heterozygous mutant mice, mice that were heterozygous-null for BMP2 (Bmp2+/−) developed more severe CHPH than their wild-type littermates (1). Our findings of the divergent effects of BMP2 and BMP4 on modulating TRPC expression and the level of basal [Ca2+]i in distal PASMCs may contribute to the mechanisms underlying these opposing responses of BMP2- and BMP4-null mice in CHPH development. In addition, the following aspects are also likely involved: the differential binding capacity of PASMCs to BMP2 and BMP4, the different location of BMP2 and BMP4 in the lung, opposing effects of BMP2 and BMP4 exerting in pulmonary hypertension, and lower levels of expression of BMP2 than BMP4 in distal PAs and PASMCs in normoxia. 1) While BMP4 was found to bind to high- and low-affinity sites on human PASMCs, BMP2 was found to bind only to low-affinity sites (40). Consequently, a higher dosage of BMP2 than BMP4 was needed to induce the downstream activation of Smad1/5 phosphorylation (40). 2) During hypoxia, the increased expression of BMP2 in mouse lung was mainly detected in the peripheral pulmonary vasculature; although BMP4 was widely expressed in endothelial cells, vascular smooth muscle cells, and epithelial compartments of the lung, the upregulation by hypoxia was only detected in bronchial and alveolar epithelium (1, 13). 3) BMP2, but not BMP4 according to the existing finding, protects against hypoxic reduction of endothelial nitric oxide synthase expression in the pulmonary vasculature (1). 4) During normoxia, expression levels of BMP2 in distal PAs and PASMCs are much lower than expression levels of BMP4, as indicated by mRNA quantification in our results. Contrary to the above-mentioned differential effects, BMP2 and BMP4 have been found to mediate similar inhibitory effects on PASMC proliferation, suggesting a complicated link between Ca2+ and the antiproliferative effects of BMP proteins, and the cell responses are likely context-specific (30). The relative expression level of BMP2 and BMP4 under chronic hypoxia and their role in regulating the hypoxia-induced increase in basal [Ca2+]i in distal PASMCs are subjects for future study.
In summary, our study demonstrates that BMP2 inhibited TRPC1, TRPC4, and TRPC6 expression in PASMCs, thereby participating in functional downregulation of SOCE and [Ca2+]i in PASMCs, leading to inhibition of cell proliferation and migration. These results suggest that BMP2 may influence PAH development by modulating TRPC expression and Ca2+ signaling in PASMCs.
GRANTS
This work was supported by National Heart, Lung, and Blood Institute Grant R01 HL-093020; National Natural Science Foundation of China Grants 81070043, 81071917, 81173112, 81170052, and 81220108001; Chinese Central Government Key Research Projects of the 973 Grant 2009CB522107; Changjiang Scholars and Innovative Research Team in University Grant IRT0961; Guangdong Department of Science and Technology of China Grants 2009B050700041 and 2010B03160030; Guangdong Province Universities and Colleges Pearl River Scholar Funded Scheme (2008) China; Guangdong Department of Education Research Grant cxzd1025; a Guangdong Natural Science Foundation Team Grant (2010); and a Guangzhou Department of Education Yangcheng Scholarship (Grant 10A058S, 12A001S).
DISCLOSURES
No conflicts of interest, financial or otherwise, are declared by the authors.
AUTHOR CONTRIBUTIONS
Y.Z., K.Y., L.X., N.L., Q.J., and X.D. performed the experiments; Y.Z., L.X., L.T., Q.J., X.D., M.-S.C., and J.W. analyzed the data; Y.Z., W.L., and J.W. interpreted the results of the experiments; Y.Z., W.L., and J.W. prepared the figures; W.L., M.-S.C., and J.W. are responsible for conception and design of the research; W.L. and J.W. drafted the manuscript; W.L., L.T., and J.W. edited and revised the manuscript; W.L. and J.W. approved the final version of the manuscript.
ACKNOWLEDGMENTS
We thank Drs. J. T. Sylvester and L. Shimoda for constructive discussion.
REFERENCES
- 1. Anderson L, Lowery JW, Frank DB, Novitskaya T, Jones M, Mortlock DP, Chandler RL, de Caestecker MP. Bmp2 and Bmp4 exert opposing effects in hypoxic pulmonary hypertension. Am J Physiol Regul Integr Comp Physiol 298: R833–R842, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ariano P, Dalmazzo S, Owsianik G, Nilius B, Lovisolo D. TRPC channels are involved in calcium-dependent migration and proliferation in immortalized GnRH neurons. Cell Calcium 49: 387–394, 2011 [DOI] [PubMed] [Google Scholar]
- 3. Beech DJ. Emerging functions of 10 types of TRP cationic channel in vascular smooth muscle. Clin Exp Pharmacol Physiol 32: 597–603, 2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bergdahl A, Gomez MF, Dreja K, Xu SZ, Adner M, Beech DJ, Broman J, Hellstrand P, Sward K. Cholesterol depletion impairs vascular reactivity to endothelin-1 by reducing store-operated Ca2+ entry dependent on TRPC1. Circ Res 93: 839–847, 2003 [DOI] [PubMed] [Google Scholar]
- 5. Bergdahl A, Gomez MF, Wihlborg AK, Erlinge D, Eyjolfson A, Xu SZ, Beech DJ, Dreja K, Hellstrand P. Plasticity of TRPC expression in arterial smooth muscle: correlation with store-operated Ca2+ entry. Am J Physiol Cell Physiol 288: C872–C880, 2005 [DOI] [PubMed] [Google Scholar]
- 6. Berridge MJ. Calcium signalling and cell proliferation. Bioessays 17: 491–500, 1995 [DOI] [PubMed] [Google Scholar]
- 7. Berridge MJ, Bootman MD, Roderick HL. Calcium signalling: dynamics, homeostasis and remodelling. Nat Rev Mol Cell Biol 4: 517–529, 2003 [DOI] [PubMed] [Google Scholar]
- 8. Cioffi DL, Wu S, Stevens T. On the endothelial cell I(SOC). Cell Calcium 33: 323–336, 2003 [DOI] [PubMed] [Google Scholar]
- 9. Dietrich A, Mederos YSM, Gollasch M, Gross V, Storch U, Dubrovska G, Obst M, Yildirim E, Salanova B, Kalwa H, Essin K, Pinkenburg O, Luft FC, Gudermann T, Birnbaumer L. Increased vascular smooth muscle contractility in TRPC6−/− mice. Mol Cell Biol 25: 6980–6989, 2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. El Boustany C, Bidaux G, Enfissi A, Delcourt P, Prevarskaya N, Capiod T. Capacitative calcium entry and transient receptor potential canonical 6 expression control human hepatoma cell proliferation. Hepatology 47: 2068–2077, 2008 [DOI] [PubMed] [Google Scholar]
- 11. Fantozzi I, Huang W, Zhang J, Zhang S, Platoshyn O, Remillard CV, Thistlethwaite PA, Yuan JX. Divergent effects of BMP-2 on gene expression in pulmonary artery smooth muscle cells from normal subjects and patients with idiopathic pulmonary arterial hypertension. Exp Lung Res 31: 783–806, 2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Firth AL, Yau J, White A, Chiles PG, Marsh JJ, Morris TA, Yuan JX. Chronic exposure to fibrin and fibrinogen differentially regulates intracellular Ca2+ in human pulmonary arterial smooth muscle and endothelial cells. Am J Physiol Lung Cell Mol Physiol 296: L979–L986, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Frank DB, Abtahi A, Yamaguchi DJ, Manning S, Shyr Y, Pozzi A, Baldwin HS, Johnson JE, de Caestecker MP. Bone morphogenetic protein 4 promotes pulmonary vascular remodeling in hypoxic pulmonary hypertension. Circ Res 97: 496–504, 2005 [DOI] [PubMed] [Google Scholar]
- 14. Golovina VA, Platoshyn O, Bailey CL, Wang J, Limsuwan A, Sweeney M, Rubin LJ, Yuan JX. Upregulated TRP and enhanced capacitative Ca2+ entry in human pulmonary artery myocytes during proliferation. Am J Physiol Heart Circ Physiol 280: H746–H755, 2001 [DOI] [PubMed] [Google Scholar]
- 15. Guo RW, Yang LX, Li MQ, Pan XH, Liu B, Deng YL. Stim1- and Orai1-mediated store-operated calcium entry is critical for angiotensin II-induced vascular smooth muscle cell proliferation. Cardiovasc Res 93: 360–370, 2012 [DOI] [PubMed] [Google Scholar]
- 16. Harper JF, Harmon A. Plants, symbiosis and parasites: a calcium signalling connection. Nat Rev Mol Cell Biol 6: 555–566, 2005 [DOI] [PubMed] [Google Scholar]
- 17. Hyvelin JM, Guibert C, Marthan R, Savineau JP. Cellular mechanisms and role of endothelin-1-induced calcium oscillations in pulmonary arterial myocytes. Am J Physiol Lung Cell Mol Physiol 275: L269–L282, 1998 [DOI] [PubMed] [Google Scholar]
- 18. Karaki H, Ozaki H, Hori M, Mitsui-Saito M, Amano K, Harada K, Miyamoto S, Nakazawa H, Won KJ, Sato K. Calcium movements, distribution, and functions in smooth muscle. Pharmacol Rev 49: 157–230, 1997 [PubMed] [Google Scholar]
- 19. Kunichika N, Landsberg JW, Yu Y, Kunichika H, Thistlethwaite PA, Rubin LJ, Yuan JX. Bosentan inhibits transient receptor potential channel expression in pulmonary vascular myocytes. Am J Respir Crit Care Med 170: 1101–1107, 2004 [DOI] [PubMed] [Google Scholar]
- 20. Kunichika N, Yu Y, Remillard CV, Platoshyn O, Zhang S, Yuan JX. Overexpression of TRPC1 enhances pulmonary vasoconstriction induced by capacitative Ca2+ entry. Am J Physiol Lung Cell Mol Physiol 287: L962–L969, 2004 [DOI] [PubMed] [Google Scholar]
- 21. Lin MJ, Leung GP, Zhang WM, Yang XR, Yip KP, Tse CM, Sham JS. Chronic hypoxia-induced upregulation of store-operated and receptor-operated Ca2+ channels in pulmonary arterial smooth muscle cells: a novel mechanism of hypoxic pulmonary hypertension. Circ Res 95: 496–505, 2004 [DOI] [PubMed] [Google Scholar]
- 22. Louis M, Zanou N, Van Schoor M, Gailly P. TRPC1 regulates skeletal myoblast migration and differentiation. J Cell Sci 121: 3951–3959, 2008 [DOI] [PubMed] [Google Scholar]
- 23. Lu W, Ran P, Zhang D, Lai N, Zhong N, Wang J. Bone morphogenetic protein 4 enhances canonical transient receptor potential expression, store-operated Ca2+ entry, and basal [Ca2+]i in rat distal pulmonary arterial smooth muscle cells. Am J Physiol Cell Physiol 299: C1370–C1378, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Lu W, Ran P, Zhang D, Peng G, Li B, Zhong N, Wang J. Sildenafil inhibits chronically hypoxic upregulation of canonical transient receptor potential expression in rat pulmonary arterial smooth muscle. Am J Physiol Cell Physiol 298: C114–C123, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Lu W, Wang J, Shimoda LA, Sylvester JT. Differences in STIM1 and TRPC expression in proximal and distal pulmonary arterial smooth muscle are associated with differences in Ca2+ responses to hypoxia. Am J Physiol Lung Cell Mol Physiol 295: L104–L113, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Machado RD, Pauciulo MW, Thomson JR, Lane KB, Morgan NV, Wheeler L, Phillips JA, 3rd, Newman J, Williams D, Galie N, Manes A, McNeil K, Yacoub M, Mikhail G, Rogers P, Corris P, Humbert M, Donnai D, Martensson G, Tranebjaerg L, Loyd JE, Trembath RC, Nichols WC. BMPR2 haploinsufficiency as the inherited molecular mechanism for primary pulmonary hypertension. Am J Hum Genet 68: 92–102, 2001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. McDaniel SS, Platoshyn O, Wang J, Yu Y, Sweeney M, Krick S, Rubin LJ, Yuan JX. Capacitative Ca2+ entry in agonist-induced pulmonary vasoconstriction. Am J Physiol Lung Cell Mol Physiol 280: L870–L880, 2001 [DOI] [PubMed] [Google Scholar]
- 28. Minke B, Cook B. TRP channel proteins and signal transduction. Physiol Rev 82: 429–472, 2002 [DOI] [PubMed] [Google Scholar]
- 29. Miriyala S, Gongora Nieto MC, Mingone C, Smith D, Dikalov S, Harrison DG, Jo H. Bone morphogenic protein-4 induces hypertension in mice: role of noggin, vascular NADPH oxidases, and impaired vasorelaxation. Circulation 113: 2818–2825, 2006 [DOI] [PubMed] [Google Scholar]
- 30. Morrell NW, Yang X, Upton PD, Jourdan KB, Morgan N, Sheares KK, Trembath RC. Altered growth responses of pulmonary artery smooth muscle cells from patients with primary pulmonary hypertension to transforming growth factor-β1 and bone morphogenetic proteins. Circulation 104: 790–795, 2001 [DOI] [PubMed] [Google Scholar]
- 31. Ng LC, Gurney AM. Store-operated channels mediate Ca2+ influx and contraction in rat pulmonary artery. Circ Res 89: 923–929, 2001 [DOI] [PubMed] [Google Scholar]
- 32. Parekh AB, Putney JW., Jr Store-operated calcium channels. Physiol Rev 85: 757–810, 2005 [DOI] [PubMed] [Google Scholar]
- 33. Poteser M, Groschner K. Studying subunit interaction and complex assembly of TRP channels. In: TRP Channels, edited by Xu MX. Boca Raton, FL: CRC, 2011, chapt. 4 [PubMed] [Google Scholar]
- 34. Remillard CV, Yuan JX. TRP channels, CCE, and the pulmonary vascular smooth muscle. Microcirculation 13: 671–692, 2006 [DOI] [PubMed] [Google Scholar]
- 35. Robertson TP, Hague D, Aaronson PI, Ward JP. Voltage-independent calcium entry in hypoxic pulmonary vasoconstriction of intrapulmonary arteries of the rat. J Physiol 525: 669–680, 2000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Shimoda LA, Sylvester JT, Sham JS. Inhibition of voltage-gated K+ current in rat intrapulmonary arterial myocytes by endothelin-1. Am J Physiol Lung Cell Mol Physiol 274: L842–L853, 1998 [DOI] [PubMed] [Google Scholar]
- 37. Smirnov SV, Robertson TP, Ward JP, Aaronson PI. Chronic hypoxia is associated with reduced delayed rectifier K+ current in rat pulmonary artery muscle cells. Am J Physiol Heart Circ Physiol 266: H365–H370, 1994 [DOI] [PubMed] [Google Scholar]
- 38. Snetkov VA, Aaronson PI, Ward JP, Knock GA, Robertson TP. Capacitative calcium entry as a pulmonary specific vasoconstrictor mechanism in small muscular arteries of the rat. Br J Pharmacol 140: 97–106, 2003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Sweeney M, Yu Y, Platoshyn O, Zhang S, McDaniel SS, Yuan JX. Inhibition of endogenous TRP1 decreases capacitative Ca2+ entry and attenuates pulmonary artery smooth muscle cell proliferation. Am J Physiol Lung Cell Mol Physiol 283: L144–L155, 2002 [DOI] [PubMed] [Google Scholar]
- 40. Upton PD, Long L, Trembath RC, Morrell NW. Functional characterization of bone morphogenetic protein binding sites and Smad1/5 activation in human vascular cells. Mol Pharmacol 73: 539–552, 2008 [DOI] [PubMed] [Google Scholar]
- 41. Wang J, Jiang Q, Wan L, Yang K, Zhang Y, Chen Y, Wang E, Lai N, Zhao L, Jiang H, Sun Y, Zhong N, Ran P, Lu W. Sodium tanshinone IIA sulfonate inhibits canonical transient receptor potential expression in pulmonary arterial smooth muscle from pulmonary hypertensive rats. Am J Respir Cell Mol Biol 48: 125–134, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Wang J, Shimoda LA, Sylvester JT. Capacitative calcium entry and TRPC channel proteins are expressed in rat distal pulmonary arterial smooth muscle. Am J Physiol Lung Cell Mol Physiol 286: L848–L858, 2004 [DOI] [PubMed] [Google Scholar]
- 43. Wang J, Shimoda LA, Weigand L, Wang W, Sun D, Sylvester JT. Acute hypoxia increases intracellular [Ca2+] in pulmonary arterial smooth muscle by enhancing capacitative Ca2+ entry. Am J Physiol Lung Cell Mol Physiol 288: L1059–L1069, 2005 [DOI] [PubMed] [Google Scholar]
- 44. Wang J, Weigand L, Lu W, Sylvester JT, Semenza GL, Shimoda LA. Hypoxia inducible factor 1 mediates hypoxia-induced TRPC expression and elevated intracellular Ca2+ in pulmonary arterial smooth muscle cells. Circ Res 98: 1528–1537, 2006 [DOI] [PubMed] [Google Scholar]
- 45. Weigand L, Foxson J, Wang J, Shimoda LA, Sylvester JT. Inhibition of hypoxic pulmonary vasoconstriction by antagonists of store-operated Ca2+ and nonselective cation channels. Am J Physiol Lung Cell Mol Physiol 289: L5–L13, 2005 [DOI] [PubMed] [Google Scholar]
- 46. Weissmann N, Dietrich A, Fuchs B, Kalwa H, Ay M, Dumitrascu R, Olschewski A, Storch U, Mederos y Schnitzler M, Ghofrani HA, Schermuly RT, Pinkenburg O, Seeger W, Grimminger F, Gudermann T. Classical transient receptor potential channel 6 (TRPC6) is essential for hypoxic pulmonary vasoconstriction and alveolar gas exchange. Proc Natl Acad Sci USA 103: 19093–19098, 2006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Xu SZ, Beech DJ. TrpC1 is a membrane-spanning subunit of store-operated Ca2+ channels in native vascular smooth muscle cells. Circ Res 88: 84–87, 2001 [DOI] [PubMed] [Google Scholar]
- 48. Young KA, Ivester C, West J, Carr M, Rodman DM. BMP signaling controls PASMC KV channel expression in vitro and in vivo. Am J Physiol Lung Cell Mol Physiol 290: L841–L848, 2006 [DOI] [PubMed] [Google Scholar]
- 49. Yu Y, Fantozzi I, Remillard CV, Landsberg JW, Kunichika N, Platoshyn O, Tigno DD, Thistlethwaite PA, Rubin LJ, Yuan JX. Enhanced expression of transient receptor potential channels in idiopathic pulmonary arterial hypertension. Proc Natl Acad Sci USA 101: 13861–13866, 2004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Yu Y, Sweeney M, Zhang S, Platoshyn O, Landsberg J, Rothman A, Yuan JX. PDGF stimulates pulmonary vascular smooth muscle cell proliferation by upregulating TRPC6 expression. Am J Physiol Cell Physiol 284: C316–C330, 2003 [DOI] [PubMed] [Google Scholar]
- 51. Zhang S, Fantozzi I, Tigno DD, Yi ES, Platoshyn O, Thistlethwaite PA, Kriett JM, Yung G, Rubin LJ, Yuan JX. Bone morphogenetic proteins induce apoptosis in human pulmonary vascular smooth muscle cells. Am J Physiol Lung Cell Mol Physiol 285: L740–L754, 2003 [DOI] [PubMed] [Google Scholar]
- 52. Zhang S, Remillard CV, Fantozzi I, Yuan JX. ATP-induced mitogenesis is mediated by cyclic AMP response element-binding protein-enhanced TRPC4 expression and activity in human pulmonary artery smooth muscle cells. Am J Physiol Cell Physiol 287: C1192–C1201, 2004 [DOI] [PubMed] [Google Scholar]
- 53. Zhu X, Chu PB, Peyton M, Birnbaumer L. Molecular cloning of a widely expressed human homologue for the Drosophila trp gene. FEBS Lett 373: 193–198, 1995 [DOI] [PubMed] [Google Scholar]