

Abstract
Objective
We examined the effect of adding a video feedback intervention component to the assessment feedback session of the Family Check-Up intervention (FCU; Dishion & Stormshak, 2007). We hypothesized that the addition of video feedback procedures during the FCU feedback at child age 2 would have a positive effect on caregivers’ negative relational schemas of their child, which in turn would mediate reductions in observed coercive caregiver-child interactions assessed at age 5.
Method
We observed the caregiver-child interaction videotapes of 79 high-risk families with toddlers exhibiting clinically significant problem behaviors. A quasi-random sample of families were provided with direct feedback on their interactions during the feedback session of the FCU protocol.
Results
Path analysis indicated that reviewing and engaging in feedback about videotaped age-2 assessment predicted reduced caregivers’ negative relational schemas of the child at age 3, which acted as an intervening variable on the reduction of observed parent–child coercive interactions recorded at age 5. Video feedback predicted improved family functioning over and above level of engagement in the FCU in subsequent years, indicating the important incremental contribution of using video feedback procedures in early family-based preventive interventions for problem behaviors.
Conclusions
Supportive video feedback on coercive family dynamics is an important strategy for promoting caregiver motivation to reduce negative attributions toward the child, which fuel coercive interactions. Our study also contributes to the clinical and research literature concerning coercion theory and effective intervention strategies by identifying a potential mechanism of change.
Keywords: assessment feedback, coercion theory, Family Check-Up, relational schema, video feedback
Viewing videotaped family interactions is becoming an increasingly popular component, and even the cornerstone, of family-based interventions for young children. Contemporary models typically include video feedback as part of a multimodal intervention strategy, along with psychoeducation, family therapy, and other forms of parental support (Brisch et al., 1997). Interventionists usually videotape a semistructured family interaction task (e.g., teaching tasks, cleanup task) in the home or laboratory setting. Relatively short segments are then carefully selected and viewed with the caregivers. Interventionists typically draw caregivers’ attention to specific, concrete behaviors during viewing. Specific efforts are made to support parenting strengths and at the same time to provide corrective feedback about maladaptive interactions.
The foci and specific procedures of video feedback vary across intervention models because of their different theoretical foundations. Yet, videotape intervention models can be generally described along two lines: behavior oriented (e.g., Stern, 2004) and psychotherapeutic (e.g., Lieberman, 2004). The distinction between these approaches can be quite difficult to make because many intervention programs combine elements of both (e.g., Beebe, 2003; Egeland, Weinfeld, Bosquet, & Cheng, 2000). The interrelated nature of the behavioral approach, which focuses on interactions, and psychotherapeutic models, which target the caregiver’s mental representations of the child and family relationships, further blurs distinctions about the targets of video feedback interventions across theoretical orientations. Regardless of the approach used, video feedback is hypothesized to help parents step back from emotionally laden interactions with their child and examine what transpires with the aide of the therapist.
The effectiveness of video feedback interventions for caregivers with young children is supported by two meta-analyses. Bakermans-Kranenburg, van IJzendoorn, and Juffer (2003) analyzed the effectiveness of 70 studies aimed at improving child attachment security (n = 1,503) and/or parental sensitivity (n = 7,636). They found that interventions with a video feedback component were more effective across outcomes (Cohen’s d = 0.44) than interventions without video (d = 0.31). Of the included studies, 20% included video feedback methods. They also found larger effects for interventions with a focus on specific parent-child interaction patterns. The child’s age was also associated with larger effects, such that intervening with children between ages 6 months and 54 months was most effective relative to work with younger (e.g., prenatal and infant) and older children. More recently, Fükkink (2008) conducted a meta-analysis of 29 methodologically rigorous studies (n = 1,844 families, child average age of 2.3 years [SD = 2.7]) of video feedback interventions. The majority of the studies that used video feedback methods in the Bakermans-Kranenburg et al. (2003) meta-analysis were included. Fükkink’s results indicated that video feedback interventions with families are effective at changing the ways caregivers think about their child (i.e., parental attitude toward the child; d = 37) and how they behave with their children (d = 47). The Fükkink meta-analysis also found that the interventions resulted in smaller effects on child-level outcomes with parents who belonged to a high-risk group. Perhaps surprisingly, Fükkink and Bakermans-Kranenburg et al. both found support for a “less is more” hypothesis, such that shorter video feedback interventions produced larger effects than did programs of longer duration. These findings indicate the potential effectiveness of using videotaped feedback methods when attempting to promote positive family interactions, particularly those that are brief and include toddlers and younger children.
Coercive Family Dynamics
Coercion is a central mechanism by which family interaction patterns are linked to problem behaviors in children (Patterson, 1982), including young children (Scaramella & Leve, 2004; Shaw & Bell, 1993). A primary tenet of coercion theory is that families engage in recurring interaction patterns during conflict, and the dispute is terminated and “won” through the use of aversive behavior. This process occurs outside of the immediate awareness of the participants, who fall back on overlearned verbal and interpersonal behaviors (Patterson, 1982). Coercive interactions are observed more often in families with children with adjustment and socialization problems (Patterson, 1982; Patterson, Reid, & Dishion, 1992). Interventions that reduce coercive interactions result in reductions in child behavior problems (e.g., Dishion, Patterson, & Kavanaugh, 1992; Forgatch & Patterson, 2010), indicating that coercive interactions are a mechanism by which problem behaviors develop in families and can also be a mechanism of change during treatment.
Toddlerhood is a salient developmental period because developmental changes in children (and requisite adjustments made by parents) result in dramatic increases in multiple forms of disruptive behavior, most notably oppositional and aggressive behavior (e.g., Campbell, Spieker, Burchinal, Poe, & The NICHD Early Child Care Research Network, 2006; Loeber & Dishion, 1983; Shaw, Gilliom, Ingoldsby, & Nagin, 2003). During this period, coercive processes typically can first be seen in the second year when toddlers’ mobility increases, yet cognitive appreciation for the consequences of their behaviors is not yet developed (Patterson, 2002). In that the child has the potential to do harm to him or herself or others, relative to infancy, caregivers increasingly use directives in an attempt to keep the child safe and control disruptive behaviors (Patterson, 1982), which can initiate coercive interactions when children fail to comply. This bidirectional, contingent response process of caregiver directive and child noncompliance, followed by the caregiver’s inadvertent escalation of the problem by withdrawing or responding harshly, which in turn leads to greater noncompliance and problem behaviors, drives the coercion cycle (e.g., Gardner, Ward, Burton, & Wilson, 2003; Shaw & Bell, 1993).
The caregiver’s interpretation that a child is purposely provoking or frustrating attempts to parent exemplifies what can be called a negative relational schema (NRS). These implicit beliefs and feelings are known mediators between family context and coercive interaction patterns (MacKinnon-Lewis, Lamb, Arbuckle, Baradaran, & Volling, 1992; Nix et al., 1999). In relational frame theory, relational schemas can be conceptualized as networks of beliefs, which become related to each other through the function of stimulus equivalence (Sidman & Tailby, 1982). Schemas are important in how individuals read and respond to social interactions, such as an angry response to a child who does not hear a parent’s request. These overlearned patterns of thinking, feeling and behaving underlie automatic, response tendencies that are challenging to address clinically without the insight of the client (Hayes, Strosahl, & Wilson, 1999). Relational schemas can also result from interpersonal histories not involving the child, such as family of origin experiences, which influence how caregivers read parent-child interactions. This process is carefully outlined by attachment theory (e.g., Bowlby, 1982; George & Solomon, 2008). Thus, the tendency to interpret malicious intent in the child may have little to do with actual behavior, but instead reflects the caregiver’s own childhood experiences of harsh parenting and rejection. Research has also demonstrated that relational schemas influence the way in which adolescents (e.g., Smith, Welsh, & Fite, 2010) and adults (e.g., Simpson, Rholes, & Winterheld, 2010) interpret and appraise the behaviors and affective states of themselves and others, as well as other salient relationship events.
Across theoretical perspectives, it is a characteristic of negative schemas that they become unaffected by environmental contingencies, such as shifts in the caregiver-child relationship (e.g., Catania, Matthews, & Shimoff, 1982), and quite difficult to alter. Reframing becomes a particularly important tool for the effective therapist working with caregivers to change parenting practices (Robins & Alexander, 1996). Therapists might, for example, help reframe a caregiver’s beliefs regarding the intentions and motivations of a child’s behaviors; doing so improves the caregiver’s flexibility to be responsive to the child’s needs, discourages adherence to overlearned relational patterns, and assumes behavior change is possible, Although these implicit interpretations of child behavior and intent are often the target of family therapy, there is a lack of research on specific strategies for systematic intervention.
Fortunately the method of assessing relational schemas is a relatively simple procedure. Borrowing from the psychodynamic tradition, Bullock & Dishion (2007) used the five-minute speech sample (Magaña et al., 1986) to assess both positive and negative relational schemas. The underlying assumption of the measurement technique is that rules about relationships are embedded within the verbal network of relations that are derived from myriad social interactions and from the verbal culture of the family and the community (Hayes, Barnes-Holmes, & Roche, 2001). Negative and positive schemas in families of adolescents were found to have predictive validity to adolescent problem behavior (Bullock & Dishion, 2007). These findings were later replicated and extended in an Australian sample (Pasalich, Dadds, Hawes, & Brennan, 2011).
More recently we examined negative and positive caregiving schemas in early childhood. Waller, Gardner, Dishion, Shaw, and Wilson (2012) found that NRSs were related to caregivers’ reports of conflict with their toddler and observed positive and harsh parenting behaviors. Further, NRSs uniquely predicted later problem behaviors in early childhood over and above caregiver reports and observational measures of parenting. There is evidence to suggest that the relationship between NRSs and coercive interactions are relevant at later developmental periods as well: MacKinnon-Lewis et al. (1992) linked mothers’ negative attributions of their 7-to 9-year-old male child to coercive mother–child interactions.
We find that coercive dynamics during early childhood are highly problematic for development. For example, we recently observed that coercive interactions appeared to drive the escalation of noncompliance and caregiver-reported oppositional defiant behaviors between ages 2 and 5 (Smith, Dishion, Shaw, Wilson, et al., under review). Observations also revealed that the stability of coercive interactions was predictive of teacher-reported behavior problems in school at age 7.5 even while controlling for the growth in oppositional defiant symptoms and observed noncompliance. Developmental cascade models leading to serious adolescent and adult outcomes (e.g., violence, substance use, and high-risk sexual behaviors) begin with early negative parent–child interactions, such as coercion (e.g., Dishion, Véronneau, & Myers, 2010; Dodge et al., 2009). Interventions that successfully reduce coercive interactions, specifically, prevent escalations in problem behaviors among high-risk children (for a review, see Forgatch & Patterson, 2010). Further, interventions aimed at improving parenting and family relationships have a high probability of long-term success when they are implemented prior to school age (Dishion & Patterson, 1992).
The Present Study
The present study examined the effects of including video feedback procedures in a brief evidence-based parenting intervention, the Family Check-Up (FCU; Dishion & Stormshak, 2007). The FCU is a second-generation intervention grounded in the Parent Management Training–Oregon Model (PMTO; Forgatch & Patterson, 2010) and designed to be implemented in community settings with the potential for a high public health impact, such as schools. The FCU’s key strategy for improving children’s behavioral health is to improve family management practices (Dishion & Stormshak, 2007). The cornerstone of the FCU is the multirater, multimethod assessment that occurs after an initial session with the parents. The assessment has an ecological focus and includes a series of brief family interaction tasks that are videotaped in the home. Salient domains of family management are assessed using a coding system of the videotaped interactions and collecting parent- and teacher-report questionnaire data and child self-report at later ages. These domains include parental positive behavior support, involvement, and limit setting, and the quality of the caregiver–child relationship. Child and caregiver adjustment and mental health factors are also assessed.
The third meeting with caregivers in the FCU is a feedback session, during which motivation to improve parenting practices is specifically targeted. The results of the ecological assessment drive the number and kind of parenting interventions that are offered to the family in the assessment feedback session. One goal of the FCU feedback session is to collaboratively help caregivers better understand the ecological factors influencing the child’s problem behaviors and enhance the family’s motivation to improve family management strategies and parenting practices. We previously found that strong therapist skill in providing support and corrective assessment feedback was pivotal to engaging and motivating parents to change the way they interact with their child (e.g., Smith, Dishion, Shaw, & Wilson, under review), indicating the importance of adherence to the interventional techniques of this session. The FCU was shown to be an effective intervention for preventing early childhood problem behavior among families participating in the Women, Infants, and Children (WIC) Nutritional Supplement program (e.g., Dishion et al., under review; Dishion et al., 2008; Gardner, Shaw, Dishion, Burton, & Supplee, 2007; Shaw, Dishion, Supplee, Gardner, & Arnds, 2006).
Although meta-analyses suggest that interventions that include video feedback are effective, in very few studies has the intervention protocol been disentangled from video feedback, because all families received the entire treatment package. Our study addressed the question, does the addition of video feedback lead to improved outcomes within an evidence-based intervention? Specifically, we examined two of the primary outcomes hypothesized to be associated with receiving video feedback: observed caregiver–child coercive interactions and caregivers’ mental representations of the child. We hypothesized that video feedback procedures, during which caregivers view their interactions with their 2-year-old child and then are guided toward identifying effective parenting behaviors by the therapist, would improve their relational schema about the child at age 3, which would in turn decrease coercive caregiver–child interactions at age 5. Shaw, Bell, and Gilliom (2000) noted that the caregiving environment in the child’s second year differentiates clinical impairment 6 years later, suggesting that this is a crucial period in which to focus intervention strategies aimed at improving parenting practices and parent–child interactions. The findings of Fükkink (2008) and Bakermans-Kranenburg et al. (2003) also suggest that video feedback interventions are most effective for parents with toddler-age children.
Method
Participants
The present study examined a subsample of 731 mother–child dyads (49% female) recruited from the Women, Infants, and Children Nutrition Program (WIC) in three geographically and culturally diverse U.S. regions near Charlottesville, VA (188 dyads), Eugene, OR (271), and Pittsburgh, PA (272), for a randomized controlled trial of the FCU. WIC families with children between age 2 years 0 months and 2 years 11 months whose screening indicated socioeconomic, family, or child risk factors for future child behavior problems were invited to participate in the study. The sample reflects cultural diversity, including African American, European American, and Latino families. Comprehensive information regarding the recruitment and randomization protocol can be found in Dishion et al. (2008). Families in both the intervention and control conditions were assessed at each wave using the same multimethod assessment battery.
Inclusion in our study was determined by either the primary or alternate caregiver reporting clinical- or borderline-range scores on the Externalizing scale of the Child Behavior Checklist 1.5/5 (Achenbach & Rescorla, 2001) at the age 2 assessment. Seventy-nine families (target child: 47% female, 53% European American, 28% African American, 6% Hispanic/Latino, 11% biracial) from the three sites (VA, 23; OR, 28; PA, 28) met inclusion criteria. The children in the sample had a mean age of 29.9 months (SD = 3.2). Primary caregivers comprised 77 biological mothers, 1 biological father, and 1 foster mother. Of this sample, 64 (81%) of the families elected to receive the FCU again at age 3, and 49 (62%) participated in the FCU at both age 3 and age 4.
Intervention
The FCU intervention protocol is more fully described elsewhere (see Dishion et al., 2008; Dishion & Stormshak, 2007). In brief, the FCU is an assessment-driven intervention model that consists of three sessions, typically beginning with an initial interview with the caregivers, a home visit to complete observational interaction tasks, and a feedback session (Figure 1). In our study, the in-home ecological assessment occurred prior to the initial contact between the caregivers and the therapist to align with the randomization protocol of the research study. In typical clinical practice using the FCU, the assessment follows the initial session. During the 1-hour feedback session, assessment results are discussed collaboratively with the caregivers. Feedback addresses families’ strengths and areas in need of improvement. Consistent with a health maintenance framework, the FCU was offered to families assigned to the intervention condition at child ages 2, 3, 4, and 5.
Figure 1. The RACS state-space grid and the measurement of coercive interactions.
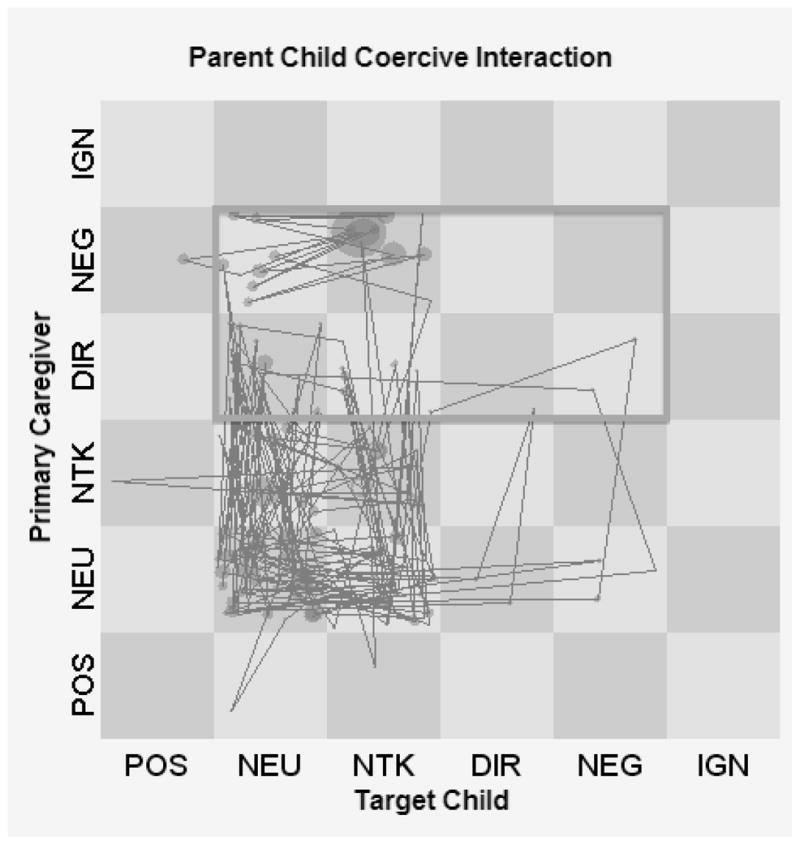
Note. POS = Postive engagement. NEU = Neutral engagement. NTK = No talk. DIR = Directive. NEG = Negative engagement. IGN = Ignore.
Therapists involved in this trial were a combination of PhD- and master’s-level service providers with previous experience carrying out family-based interventions. Modal therapists had a master’s-level degree in social work, education, or psychology. Prior to working with study families, therapists were trained for 2.5–3 months using didactic instruction, role-plays, and videotaped supervision of intervention activity. Therapists were also certified by the lead therapist at each site, who had been previously certified by the intervention developer. Certification procedures were designed to ensure therapist competence in all critical components of the FCU. Subsequent rating of FCU feedback sessions conducted with study families at child age 2 indicated fidelity of implementation scores above the minimum competency cutoff (Smith, Dishion, Shaw, & Wilson, under review). Therapists were of diverse ethnic status, including African American, European American (the majority), Hispanic/Latino, and mixed ethnicity. Weekly cross-site case reviews were convened and fidelity of implementation rating procedures occurred yearly to reduce drift.
Video feedback was used at the discretion of the therapist, although the treatment developer encouraged its use. Thus, assignment to the video feedback condition was not randomized, nor was it under the control of the researchers. Therapists were given the flexibility to select videotaped segments of caregivers and their child involved in the structured interaction tasks that are part of the FCU’s ecological assessment. Working within the model’s strengths-based framework, therapists most often elected to show short video clips of caregivers using effective and desirable parenting skills, which the therapist then worked to reinforce. This procedure is similar to previous articulations of video modeling and “feedforward” procedures described in a review by Dowrick (1999). Video modeling and feedforward techniques emphasize reinforcing the effective behaviors caregivers are already practicing, as opposed to pointing out ineffective parenting behaviors. The therapists who implemented videotape feedback were primarily at the treatment site supervised by the developer.
Assessment Procedure
In each wave of the study, an independent assessment team assessed families in the control and the intervention conditions of the randomized trial from which the sample of the present study was drawn. The assessment team was blind to the assignment of the family and conducted the same assessment procedures for all families. The videotaped interactions occurred most often in the families’ homes. Families received monetary compensation for participating in the assessment at each wave of data collection.
Measures
Video feedback
The FCU feedback sessions conducted at age 2 were rated using the COACH system to assess fidelity of implementation (Dishion, Knutson, Brauer, Gill, & Risso, 2010). During fidelity rating procedures, sessions were coded for having used video feedback (yes/no; (see Smith, Dishion, Shaw, & Wilson, under review). In total, 23 families, all from the Eugene site, were given video feedback.
Cumulative risk
An index of cumulative risk was generated from seven indicators of socioeconomic risk reported at entry into the study (child age 2). These indicators were (a) single parenthood, (b) parent substance use problem, (c) low maternal education, (d) residence in a dangerous neighborhood, (e) residence in a densely populated neighborhood, (f) income below the national poverty line, and (g) parent with felony conviction. Families received a score of 1 for each risk indicator if present or a 0 if the risk indicator was absent. The cumulative risk index score is a total of the seven indicators. The mean cumulative risk score of the sample in this study was 2.14 (SD = 1.33, range: 0–5).
Negative relational schemas
Primary caregivers’ relational schemas about their child were assessed at ages 2 and 3 using the Family Affective Attitude Rating Scale (FAARS; (Bullock & Dishion, 2004; Bullock, Schneiger, & Dishion, 2005). The FAARS is a macrosocial code used with a 5-minute speech sample (FMSS; Magaña et al., 1986) during which caregivers are asked to talk about their child and his or her relationship with the child. Assessors gave the following instructions to caregivers: “I’d like to hear your thoughts and feelings about (child’s name), in your own words and without my interrupting with any questions or comments. When I ask you to begin I’d like you to speak for 5 minutes, telling me what kind of person (child’s name) is and how the two of you get along together. After you begin to speak, I prefer not to answer any questions until after the 5 minutes. Do you have any questions?” Assessors then leave the room to minimize distractions while the caregivers’ response is digitally recorded.
Trained undergraduate and graduate coders rated the FMSSs on the three scales of the FAARS: (1) Negative Attitudes and (2) Positive Attitudes expressed by the primary caregiver about the child, and (3) Family Cohesion. We used only the Negative scale (i.e., NRS). Coders were required to achieve 80% agreement on seven consecutive samples during training. Coding teams met one or two times a week during training. An average of 4 weeks was needed to achieve 80% agreement among the team. After training, coders continued to meet one time per week to prevent coder drift. Ratings of the speech sample were given across several dimensions on the basis of global impressions of the whole speech sample to avoid undue influence by discrete pieces of information, and on the basis of substantive information about current attributions or behaviors.
Items in the NRS scale were rated on a 9-point Likert scale: 1 (no examples evidenced), 2–3 (some indication, but no concrete evidence), 4 (one or more weak examples), 5 (one concrete and unambiguous example, or three or more weak examples), 6–8 (at least one concrete example and one or more weak examples), and 9 (two or more concrete, unambiguous examples). For additional information regarding scoring criteria, see the FAARS manual (Bullock et al., 2005). The NRS scale comprises five codes: (1) the parent is critical of the child’s behavior, (2) the parent is critical of the child’s traits/personality, (3) the parent has a negative relationship with the child, (4) the parent assumes/attributes negative intentions of the child, and (5) the parent reports conflict/anger/hostility toward the child.
The FAARS has been previously validated with the full 731-participant sample from the randomized trial from which the participants in the present study were drawn (Waller et al., 2012), a sample of mothers of preschool-age children (Pasalich et al., 2011), and parents of adolescents (Bullock & Dishion, 2007). Cronbach’s alphas for NRS in the sample used in the present study indicated good internal reliability at both ages (age 2, α = .83; age 3, α = .84), which is consistent with previous FAARS validation studies.
Caregiver coerce
Primary caregivers (predominantly biological mothers) and children who agreed to participate in the study were scheduled for a 2.5-hour home visit to complete videotaped interaction tasks each year. Each assessment began by introducing the child to an assortment of age-appropriate toys and having them play for 15 minutes while the mothers completed questionnaires. A free play period was followed by the primary caregiver and child participating in a cleanup task (5 minutes) at age 2. A delay of gratification task followed (5 minutes) the cleanup task at age 5. At both ages, 3-minute-long teaching tasks (two at age 2 and two at age 5) followed. Afterwards, different inhibition-inducing toys were introduced for 2 minutes each (two toys at age 2, a remote controlled robot and a child-size tunnel, and one at age 5, a pet carrier with an unidentified stuffed animal inside playing a tape recording of cougar sounds). The final task involved a meal preparation and lunch (20 minutes total).
The videotaped interaction tasks involving the child and the primary caregiver were coded using the Relationship Affect Coding System (RACS; Peterson, Winter, Jabson, & Dishion, 2008). The RACS records three continuous streams of behavior: verbal, physical, and affect and captures the duration of events within each. Verbal codes comprise positive, neutral, and negative talk and include verbal behavior change codes, such as positive structuring, neutral, and negative directives. Physical behaviors (e.g., hugging, handing each other objects) are coded as positive, neutral, and negative. Affect codes include anger/disgust, distress, ignoring, validation, and positive affect. The “off” codes of no talk, no physical, and neutral affect are used when verbal, physical behavior, or affect streams are not observed. The RACS coding was done using Noldus Observer (Noldus Information Technology, 2003), which enables continuous coding of an interaction as the behaviors are observed. As such, the exact durations and frequencies of the behaviors of interest are captured.
Summary scores were created to capture salient dimensions of the parent–child interaction. First, the verbal, physical, and affect streams were combined to create six behavior clusters: positive engagement (POS), neutral engagement (NEU), no talk (NTK), directives (DIR), negative engagement (NEG), and ignore (IGN). A state space grid was used to summarize the dynamic exchanges between the caregiver and child. In a state space grid, the child’s behavior is selected as time T and the parent’s reaction as T+1 (Caregiver on y-axis and Child on x-axis in Figure 1). This data structure required forming a set of priority rules from the three parallel streams. For instance, if the caregiver smiled and at the same time was observed to be saying something negative to the child, the negative verbal code trumped the smile, a positive affect code, and the caregiver’s behavior was classified within the negative engagement cluster, which is labeled NEG in Figure 1. The end result allows us to analyze and identify the dyadic interaction patterns that have been graphed on the state space grid (see Tom Hollenstein, 2007). State space grids have previously been adapted for the study of caregiver–child interactions and their relationship with child psychopathology (e.g., Granic, Hollenstein, Dishion, & Patterson, 2003; T. Hollenstein, Granic, Stoolmiller, & Snyder, 2004).
In the state space grid, all parenting behaviors are a response to the child’s behavior. In this study, we were particularly interested in the caregivers’ tendency to react harshly and use coercive strategies when managing the child’s behavior. Thus, the Caregiver Coerce measure was defined as the times when the caregiver was observed to be negatively engaged (NEG) or directive (DIR) and the child was observed to be responding in a neutral (NEU), directive (DIR), or negative (NEG) manner or was not talking (NTK). This region thus comprises 8 cells from the 36 total possible cells of the complete matrix, represented with a dark grey rectangle in Figure 1. We then calculated the total duration of each caregiver–child dyad exchange relevant to this region and divided that time by the overall session time to get a duration proportion score. The average duration proportion of caregiver–child coercive interaction in our sample is .224, .189, and .172 at ages 2, 3, and 5, respectively. Reliability coefficients were in the “good” to “excellent” range, with overall kappa scores of .68, .68, and .72 at ages 2, 3, and 5, respectively. Kappa coefficients were obtained from Noldus Observer. We used the RACS coding from interaction tasks administered at the home assessments across all three ages, that is, the teaching, inhibition, and meal tasks.
Data Analytic Plan
To address the study hypothesis, path modeling was conducted using structural equation modeling with Mplus 6.12 (L. K. Muthén & Muthén, 2012). The full subsample of 79 families was used in all analyses, with the video feedback condition as the group comparison variable (yes = 23, no = 56). A Bayesian estimator was used because of its robust performance under conditions of smaller sample sizes compared with estimation based on maximum likelihood (Lee & Song, 2004; B. O. Muthén, 2010a). Similar to full information maximum likelihood, the Bayesian estimator uses all available data to estimate parameters (Asparouhov & Muthén, 2010; Little & Rubin, 2002). Minimal missing data in this sample were found to be missing completely at random (Little’s (1988)] MCAR test, χ2(33) = 41.71, ns), so the missing data did not introduce bias into the analyses. Mplus provides a 95% credibility interval for all estimated effects in structural equation models that use Bayesian estimation.
Rather than focus on the typical requirements for mediation (i.e., a significant direct effect of the predictor on the presumed mediator and on the distal outcome, a significant direct effect of the mediator on the outcome, and a significant indirect effect of the predictor on the outcome via the mediator; Judd, Kenny, & McClelland, 2001; MacKinnon & Dwyer, 1993), which some have argued is too restrictive (e.g., MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002), we focused on the joint significance of the paths from the predictor to the outcome through a mediating variable. MacKinnon et al. (2002) refer to the purported mediator as an intervening variable in this type of analysis. When the Bayes estimator is used, if the provided confidence interval (CI) of the specified indirect effect does not contain zero, the effect is considered statistically significant (Yuan & MacKinnon, 2009).
Results
Preliminary Analyses
Correlations among model variables are provided in Table 1, along with means and standard deviations. Nonrandom assignment to the video feedback condition necessitated examining possible group differences that could have influenced therapists’ use of this therapeutic technique. Given the focus on showing caregivers examples of desirable parenting, it is plausible that therapists elected to use video feedback with families that demonstrated more positive parenting behaviors. Thus, we examined mean differences in three coder impression indices of positive parenting behaviors at the age 2 assessment, derived from the same interaction tasks as our coercive interactions measure. Independent samples t-tests revealed no significant differences between the families that did and did not receive video feedback on the following: caregiver demonstrates proactive parenting, t(76) = .009, p = .99; caregiver promotes positive child behaviors, t(76) = −1.27, p = .21; and caregiver engages in positive interactions with the child, t(76) = −1.58, p = .12. Thus, it does not appear that receipt of video feedback was determined exclusively by presence or absence of positive parenting. We then proceeded to the planned path analysis.
Table 1.
Intercorrelations Between Video Feedback, Observed Coercion Measures, and Caregiver’s Negative Relational Schemas
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Participants (N = 79) | |||||||
| 1. Video feedback used at age 2 (Yes = 1/No = 0) | — | −.34* | −.16 | .15 | −.16 | .03 | −.16 |
| 2. Observed coercive interactions (age 2) | — | .32** | −.06 | .02 | −.13 | .31* | |
| 3. Observed coercive interactions (age 5) | — | .09 | .24 | .09 | .17 | ||
| 4. Caregiver’s negative relational schemas (age 2) | — | .36** | .07 | −.07 | |||
| 5. Caregiver’s negative relational schemas (age 3) | — | .03 | −.05 | ||||
| 6. Engagement in the FCU (ages 3 and 4) | — | −.04 | |||||
| 7. Cumulative risk | — | ||||||
| Mean | .29 | .23 | .17 | 3.42 | 3.15 | 1.53 | 2.14 |
| Standard deviation | .46 | .10 | .08 | 1.59 | 1.54 | .66 | 1.33 |
Note. Correlations were calculated using a Pearson’s r. p-values are two-tailed.
p < .01;
p < .05.
Path Analysis
Path analysis began with an examination of the model fit of the model presented in Figure 2. Model fit using Bayes estimation uses the posterior predictive checking (PPC) method. Model fit is determined in two ways using PPC: (a) Mplus produces a 95% CI in which a negative lower limit is considered to be one indicator of good model fit (B. O. Muthén, 2010b), and (b) Mplus also provides a posterior predictive p-value (PPP) of model fit based on the usual chi-square test of Ho against H1. Lower PPP values indicate poorer fit (B. O. Muthén, 2010b). Our model provided good fit to the data on the basis of the PPC (95% CI: −25.97 | 39.64) and the PPP (0.36). With adequate model fit, we proceeded by examining the results of the path model.
Figure 2. Results of path analysis.
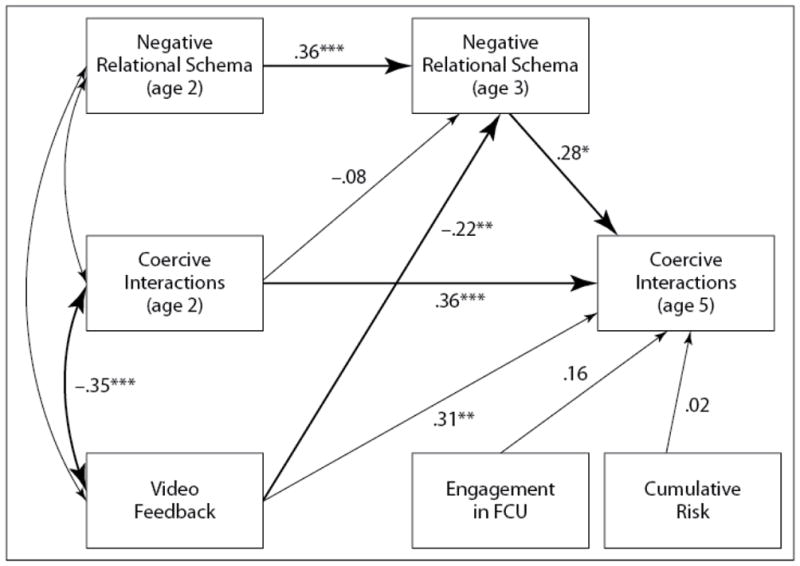
Note. * p < .05. ** p < .01. *** p < .001.
The path coefficients for the model in Figure 2 are provided in Table 2. Receipt of video feedback was significantly related to NRS at age 3, controlling for prior levels, which was significant. NRSs were significantly related to observed coercive interactions 2 years later, again controlling for earlier levels. Because the direct path between video feedback and coercive interactions at age 5 was not significant, we examined the significance of the indirect effect. We used the Model Constraint command in Mplus to test the joint path significance from video feedback to NRS to coercive interactions. The effect was found to be significant, indicating that primary caregivers’ NRS served as an intervening variable between video feedback and reduced coercive interactions at age 5. We controlled for two potentially confounding variables on coercive interactions in this model: engagement in the FCU and cumulative risk, both of which were not significant, indicating that familial risk factors, such as single adult household and poverty, among others, were not significantly associated with levels of coercive interactions observed at age 5. Similarly, the effect of video feedback at the age 2 FCU on coercive interactions at age 5 was not related to engagement in the intervention in the intermediary years (ages 3 and 4). We also included the race/ethnicity of the child as a possible covariate, which was nonsignificant and was not retained in the final model. The total R2 for coercion was .26.
Table 2.
Results of Path Analysis
| Participants N = 79 | ||||
|---|---|---|---|---|
|
| ||||
| Model path | B | Posterior SD | β | 95% credibility interval |
| Video feedback → NRS (age 3) | −.75** | .39 | −.22 | −1.57 | .066 |
| Video feedback → coercive interactions (age 5) | .00 | .02 | .02 | −.037 | .043 |
| NRS (age 3) → coercive interactions (age 5) | .02* | .01 | .28 | .003 | .029 |
| Coercive interactions (age 2) → coercive interactions (age 5) | .26 | .09 | .31 | .057 | .441 |
| Coercive interactions (age 2) → NRS (age 3) | −1.20 | 1.96 | −.08 | −4.646 | 2.583 |
| NRS (age 2) → NRS (age 3) | .35 | .11 | .36 | .171 | .612 |
| Engagement in FCU → coercive interactions (age 5) | .02 | .02 | .16 | −.014 | .052 |
| Cumulative risk → coercive interactions (age 5) | .00 | .01 | .02 | −.014 | .018 |
| Indirect effect | ||||
|
| ||||
| Video feedback → NRS (age 3) → coercive interactions (age 5) | −0.10* | .09 | −.06 | −.309 |− .001 |
Note. NRS = negative relational schema; FCU = Family Check-Up;
p < .01; *p < .05.
Discussion
The results of this small sample study provide support for the use of video feedback in the FCU and other parenting interventions for high-risk families with toddler-age children. Our findings also illuminate the potential mechanism of change involved in the reduction of coercive family interactions; that is, the primary caregiver’s negative attributions about the child. Video feedback intervention was shown to reduce the caregiver’s negativity about the child, which is related to less observed coercion, supporting the use of video feedback procedures in the FCU during the preschool years. These findings are consistent with the results of Fükkink’s (2008) meta-analysis. Perhaps most important for future intervention research and development is that these results occurred in a sample of families that all received the FCU, indicating the potential incremental effects of this additional component in the context of an evidence-supported model. This hypothesis should be empirically tested.
Parent observation of various types is becoming a recognized intervention in many subfields of child and family intervention and assessment, and its benefits are becoming increasingly appreciated. A number of evidence-supported collaborative and therapeutic models of family assessment, similar to the FCU, routinely incorporate parent observation in the assessment procedures (see Tharinger et al., 2012). Results consistently demonstrate that parent observation techniques, whether in real time or using carefully selected video feedback procedures similar to those described in our study, alter caregivers’ attributions of the child’s behaviors, which has been theorized to be a mechanism of action (e.g., Holigrocki, Crain, Bohr, Young, & Bensman, 2009; Smith, Nicholas, Handler, & Nash, 2011; Tharinger et al., 2009). Finn (2007) observed that parents may interpret their children’s behaviors in a manner that fits their current schema or “story” about the child and fail to perceive information that does not fit. Video feedback and parent observation procedures are potentially powerful therapeutic techniques to pinpoint and increase the accuracy of relational schemas that govern coercive caregiver–child interactions.
Our findings help illuminate this potential mechanism of action. Video feedback procedures might enable parents to objectify their emotionally arousing interactions with their child, during which negative and disengaged parenting behaviors often occur (e.g., Dishion, Burraston, & Li, 2003), and can motivate them to make changes to their parenting practices and parent–child interaction patterns. Finn and colleagues (Finn, 2007; Tharinger et al., 2012) describe this process as caregivers being invited onto an observation deck from which they can examine their behaviors with the support of an interventionist. According to Finn, observing family interactions in this manner helps caregivers develop empathy for the child and the family. We deduce that the inclusion of videotape in the feedback enabled caregivers to gain some perspective on the positive aspects of interactions with their child. As relational frame theory posits, schemas are automatic, unconscious response tendencies. Providing caregivers the opportunity to disembed from emotionally laden interactions and view them through a more objective lens, with the support of the therapist, may facilitate a shift in the way the child is viewed and result in more positive response tendencies. Using feedforward video feedback techniques empowers caregivers to make this shift because it reinforces desired behaviors already being used by the caregiver, as evidenced by their videotaped interactions, rather than attempt to learn entirely new ways of interacting and responding. This approach is consistent with the strengths-based nature of the FCU.
Although the trend was not explicitly measured in this study, video feedback might be leading the caregiver to develop a more compassionate view of the child and the problem behaviors for which they are seeking intervention, as well as self-compassion for the challenges of parenting. The reduction in negative attributions suggests a shift in the caregivers’ ability to see and support children’s positive behavior, as opposed to using harsh parenting to prevent and reduce negative behavior based on their preexisting schema about the child. However, future research is needed on the underlying mechanisms that mark a shift from coercive to more supportive parenting styles in the context of intervention studies. In particular, it will be helpful to specifically measure mediating mechanisms suggested by attachment and relational frame theory regarding relationship schemas, such as caregiver and child attachment status.
Another consideration in the interpretation of the findings is an issue with the design, specifically the nonrandomization of receipt of video feedback. Video feedback procedures were conducted only at one treatment site and families had lower levels of initial durations of caregiver coercion. Even though there were no significant differences in the two groups on indices of positive parenting practices observed during the assessment tasks, a prospective, randomized design would address these other design limitations. However, these findings provide some evidence regarding which families might benefit from the desired effects of video feedback as they were more often used with families that were observed to engage in less coercive interactions. In the context of a preventive intervention for high-risk families, it is desirable to target reductions in any initial level of early coercion, which in turn slows the escalation of later problem behaviors. At the same time, we hope to intervene effectively with families demonstrating higher levels of coercive interactions, in that we know coercion is a powerful predictor of later outcomes (e.g., Dishion & Patterson, 2006). Future research is needed to determine if families with greater coercive interactions will similarly benefit from using video feedback, including families from higher socioeconomic strata than that of this study sample. Perhaps feedforward procedures will be equally effective, but it could also be that a different means of addressing coercive interaction patterns will be needed for families in which desirable parenting practices are absent in the videotaped interactions. Our results also suggest that video feedback could be most effective for high-risk families with moderate levels of coercive interactions. This finding is somewhat consistent with the conclusion drawn by Fükkink (2008), which suggested that high-risk status was associated with smaller intervention effects. This should be tested prospectively with random assignment. It could be that initial levels of coercion moderate the effects of video feedback interventions.
Although it is a methodological drawback of the study not to have randomized assignment to the video feedback condition, there is a high probability that these effects will be replicated given the empirical link between NRSs and coercive interactions during early childhood (e.g., MacKinnon-Lewis et al., 1992; Waller et al., 2012) and the positive effects video feedback interventions have on parental attitudes and attributes about the child (e.g., Fükkink, 2008). Traditionally, inclusion of an intervention component is prescribed, meaning each participant in the intervention receives that aspect of the model, which is generally used to determine adherence to the treatment (Waltz, Addis, Koerner, & Jacobson, 1993). However, adaptive and individually tailored prevention and treatment models have recently gained traction (Collins, Murphy, & Bierman, 2004; Murphy, Collins, & Rush, 2007), including the FCU, which uses decision rules and extensive assessment results to guide the selection of indicated intervention components (Dishion & Stormshak, 2007). In an adaptive framework, intervention components are included if empirical evidence suggests they will be effective when added to the larger intervention (Collins, Murphy, & Strecher, 2007). The decision rules guiding the selection process are very important to ensuring effectiveness. In our study, therapists were given the option to include video feedback in the FCU feedback session in cases in which the caregiver(s) demonstrated desirable parenting practices that could be reinforced, but there were no formalized decision rules governing the selection process. These preliminary decision rules must be tested and empirically informed.
Limitations
Three primary limitations of this study indicate the need for replication and future research on this topic. The first limitation is the small sample size, which limits power and generalizability. In terms of generalizability, some features of this sample are somewhat unique. Families in this sample opted to participate in a family-based prevention intervention, suggesting sufficient motivation to learn new ways of parenting their child and perhaps sufficient child problem behaviors, as evidenced by the borderline or clinical elevations reported by the primary or alternative caregiver. The sample also comprised lower income families recruited through the WIC program. One can conclude that our results are likely to replicate with lower income, higher risk families engaging in moderate levels of coercive caregiver–child interactions. It is less clear whether the results would generalize to higher SES families with similar types of familial interactions and the motivation to change parenting. Fükkink’s (2008) meta-analysis found smaller effects of video feedback interventions for higher risk parents, further suggesting that our results might generalize to higher SES families that share other characteristics of this sample. However, the most reasonable conclusion that can be drawn from our results is that a follow-up investigation using a randomized trial is needed.
The second limitation, as already mentioned, was the procedures used to select the delivery of video feedback. Because there was no random assignment, which would have increased the internal validity of the findings, and no specific decision rules were in place to guide therapists on electing whether or not to use video feedback, the results of the study are somewhat limited in terms of applying wide-ranging conclusions to other samples. The third limitation, which is a byproduct of the second, is the issue of a potential site-specific effect. The parent study from which this subsample was drawn was conducted in three geographically diverse regions: Charlottesville, VA; Eugene, OR; and Pittsburgh, PA. At the age-2 FCU, only therapists at the Eugene site elected to use video feedback, at least with this subsample of high-risk families with children with elevated problem behaviors, although not all the families at this site received video feedback. The cultural, racial, and ethnic diversity of these regions and of the families included in the study from those regions is undoubtedly different, but is confounded with the study site, making it unfeasible to test for racial and cultural differences. A prospective research design would address this problem.
Conclusions
Although this study has limitations, the results suggest that video feedback procedures increase intervention effects on coercive caregiver–child dynamics within the FCU, but perhaps more so for high-risk families with moderate initial levels of coercion who are motivated to learn new ways of parenting their children. Further, the use of video feedback appears to shift caregivers’ NRSs about the child, which seems to be a mechanism of action for effectively reducing coercion. Video feedback interventions are a very brief technique within the already succinct FCU model, making it a feasible and effective addition. Given the strong empirical links between early coercive dynamics and later problems for children and adolescents (e.g., Dishion & Patterson, 2006; Patterson, 2002; Shaw et al., 2003), improving intervention effects on coercion, particularly with short, simple to implement methods such as video feedback, ought to be pursued.
Acknowledgments
This research was supported by National Institute on Drug Abuse grant DA016110 to the second, fourth, and fifth authors. Justin D. Smith received support from research training grant MH20012 from the National Institute of Mental Health, awarded to Elizabeth Stormshak. The authors also gratefully thank Cheryl Mikkola for editorial support, David MacKinnon for consultation pertaining to intervening variable effects using Bayesian estimation in structural equation modeling, the observational coding team at the Child and Family Center, the rest of the Early Steps team in Eugene, Pittsburgh, and Charlottesville, and the families who have participated in the study.
Contributor Information
Justin D. Smith, Email: jsmith6@uoregon.edu, Child and Family Center, University of Oregon
Thomas J. Dishion, Email: dishion@asu.edu, dishion@uoregon.edu, Child and Family Center, University of Oregon, & Prevention Research Center, Arizona State University
Kevin J. Moore, Email: kmoore2@uoregon.edu, Child and Family Center, University of Oregon
Daniel S. Shaw, Email: casey@pitt.edu, University of Pittsburgh
Melvin N. Wilson, Email: mnw@uvirginia.edu, University of Virginia
References
- Achenbach TM, Rescorla LA. Manual for the ASEBA school-age forms and profiles. U.S.A: Library of Congress; 2001. [Google Scholar]
- Asparouhov T, Muthén BO. Bayesian analysis using Mplus: Technical implementation. Mplus Technical Report. 2010 Retrieved from http://www.statmodel.com.
- Bakermans-Kranenburg MJ, van IJzendoorn MH, Juffer F. Less is more: Meta-analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin. 2003;129(2):195–215. doi: 10.1037/0033-2909.129.2.195. [DOI] [PubMed] [Google Scholar]
- Beebe B. Brief mother–infant treatment: Psychoanalytically informed video feedback. Infant Mental Health Journal. 2003;24(1):24–52. [Google Scholar]
- Bowlby J. Attachment and loss: Retrospect and prospect. American Journal of Orthopsychiatry. 1982;52(4):664–678. doi: 10.1111/j.1939-0025.1982.tb01456.x. [DOI] [PubMed] [Google Scholar]
- Brisch KH, von Gontard A, Pohlandt F, Kächele H, Lehmkuhl G, Roth B. Interventions program für Eltern von Frühgeborenen: Kritische Übersicht [Intervention programs for parents with premature infants: A critical review] Monatsschrift Kinderheilkunde. 1997;145:457–465. [Google Scholar]
- Bullock BM, Dishion TJ. Family Affective Attitude Rating Scale (FAARS) C. Winter, Child and Family Center; 6217 University of Oregon, Eugene, OR 97403: 2004. e-mail: cwinter@uoregon.edu. [Google Scholar]
- Bullock BM, Dishion TJ. Family processes and adolescent problem behavior: Integrating relationship narratives into understanding development and change. Journal of the American Academy of Child & Adolescent Psychiatry. 2007;46(3):396–407. doi: 10.1097/chi.0b013e31802d0b27. [DOI] [PubMed] [Google Scholar]
- Bullock BM, Schneiger A, Dishion TJ. Manual for coding five- minute speech samples using the Family Affective Attitude Rating Scale (FAARS) the Child and Family Center; 6217 University of Oregon, Eugene, OR 97403: 2005. [Google Scholar]
- Campbell SB, Spieker S, Burchinal M, Poe MD The NICHD Early Child Care Research Network. Trajectories of aggression from toddlerhood to age 9 predict academic and social functioning through age 12. Journal of Child Psychology and Psychiatry. 2006;47(8):791–800. doi: 10.1111/j.1469-7610.2006.01636.x. [DOI] [PubMed] [Google Scholar]
- Catania AC, Matthews BA, Shimoff E. Instructed versus shaped human verbal behavior: Interaction with nonverbal responding. Journal of Experimental Analysis of Behavior. 1982;38:233–248. doi: 10.1901/jeab.1982.38-233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins LM, Murphy SA, Bierman KL. A conceptual framework for adaptive preventive interventions. Prevention Science. 2004;5:185–196. doi: 10.1023/b:prev.0000037641.26017.00. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins LM, Murphy SA, Strecher V. The Multiphase Optimization Strategy (MOST) and the Sequential Multiple Assignment Randomized Trial (SMART): New methods for more potent ehealth interventions. American Journal of Preventive Medicine. 2007;32(5, Supplement):S112–S118. doi: 10.1016/j.amepre.2007.01.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Brennan LM, Shaw DS, McEachern AD, Wilson MN, Jo B. Prevention of problem behavior through annual Family Check-Ups in early childhood: Intervention effects from the home to the second grade of elementary school. Journal of Consulting and Clinical Psychology. doi: 10.1007/s10802-013-9768-2. (under review) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Burraston B, Li F. Family management practices: Research design and measurement issues. In: Sloboda Z, Bukoski WJ, editors. Handbook for drug abuse prevention: Theory, science, and practice. New York, NY: Plenum; 2003. pp. 587–607. [Google Scholar]
- Dishion TJ, Knutson N, Brauer L, Gill A, Risso J. Unpublished coding manual. the Child and Family Center; 6217 University of Oregon, Eugene, OR 97403: 2010. Family Check-Up: COACH ratings manual. [Google Scholar]
- Dishion TJ, Patterson GR. Age effects in parent training outcome. Behavior Therapy. 1992;23:719–729. [Google Scholar]
- Dishion TJ, Patterson GR. The development and ecology of antisocial behavior. In: Cicchetti D, Cohen DJ, editors. Developmental psychopathology, Vol. 3: Risk, disorder, and adaptation. New York, NY: Wiley; 2006. pp. 503–541. [Google Scholar]
- Dishion TJ, Patterson GR, Kavanaugh K. An experimental test of the coercion model: Linking theory, measurement, and intervention. In: McCord J, Tremblay R, editors. The interaction of the theory and practice: Experimental studies of interventions. New York, NY: Guilford; 1992. pp. 253–282. [Google Scholar]
- Dishion TJ, Shaw DS, Connell A, Gardner FEM, Weaver C, Wilson M. The Family Check-Up with high-risk indigent families: Preventing problem behavior by increasing parents’ positive behavior support in early childhood. Child Development. 2008;79(5):1395–1414. doi: 10.1111/j.1467-8624.2008.01195.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Stormshak EA. Intervening in children’s lives: An ecological, family-centered approach to mental health care. Washington, DC: American Psychological Association; 2007. [Google Scholar]
- Dishion TJ, Véronneau MH, Myers MW. Cascading peer dynamics underlying the progression from problem behavior to violence in early to late adolescence. Development and Psychopathology. 2010;22(Special Issue 03):603–619. doi: 10.1017/S0954579410000313. [DOI] [PubMed] [Google Scholar]
- Dodge KA, Malone PS, Lansford JE, Miller S, Pettit GS, Bates JE. A dynamic cascade model of the development of substance-use onset: Early peer relations problem factors. Monographs of the Society for Research in Child Development. 2009;74(3):51–54. doi: 10.1111/j.1540-5834.2009.00528.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dowrick PW. A review of self-modeling and related interventions. Applied & Prevention Psychology. 1999;8:23–39. [Google Scholar]
- Egeland B, Weinfeld NS, Bosquet M, Cheng VK. Remembering, repeating, and working through: Lessons from attachment-based interventions. In: Osofsky JD, Fitzgerald HE, editors. WAIMH handbook of infant mental health. Vol. 4. New York, NY: John Wiley & Sons; 2000. pp. 38–89. [Google Scholar]
- Finn SE. In our client’s shoes: Theory and techniques of Therapeutic Assessment. Mahwah, NJ: Erlbaum; 2007. [Google Scholar]
- Forgatch MS, Patterson GR. Parent management training-Oregon model: An intervention for antisocial behavior in children and adolescents. In: Weisz JR, Kazdin AE, editors. Evidence-based psychotherapies for children and adolescents. New York, NY: Guilford Press; 2010. pp. 159–178. [Google Scholar]
- Fükkink RG. Video feedback in widescreen: A meta-analysis of family programs. Clinical Psychology Review. 2008;28(6):904–916. doi: 10.1016/j.cpr.2008.01.003. [DOI] [PubMed] [Google Scholar]
- Gardner FEM, Shaw DS, Dishion TJ, Burton J, Supplee L. Randomized prevention trial for early conduct problems: Effects on proactive parenting and links to toddler disruptive behavior. Journal of Family Psychology. 2007;21(3):398–406. doi: 10.1037/0893-3200.21.3.398. [DOI] [PubMed] [Google Scholar]
- Gardner FEM, Ward S, Burton J, Wilson C. The role of mother–child joint play in the early development of children’s conduct problems: A longitudinal observational study. Social Development. 2003;12:361–379. [Google Scholar]
- George C, Solomon J. The caregiving system: A behavioral systems approach to parenting. In: Cassidy J, Shaver PR, editors. Handbook of attachment: Theory, research, and clinical applications. 2. New York, NY: Guilford Press; 2008. pp. 833–856. [Google Scholar]
- Granic I, Hollenstein T, Dishion TJ, Patterson GR. Longitudinal analysis of flexibility and reorganization in early adolescence: A dynamic systems study of family interactions. Developmental Psychology. 2003;39(3):606–617. doi: 10.1037/0012-1649.39.3.606. [DOI] [PubMed] [Google Scholar]
- Hayes SC, Barnes-Holmes D, Roche B, editors. Relational frame theory: A post-skinnerian account of human language and cognition. Vol. 28. New York, NY: Kluwer Academic/Plenum Publishers; 2001. [DOI] [PubMed] [Google Scholar]
- Hayes SC, Strosahl K, Wilson K. Acceptance and commitment therapy: An experimental approach to behavior change. New York, NY: Guilford Press; 1999. [Google Scholar]
- Holigrocki R, Crain C, Bohr Y, Young K, Bensman H. Interventional use of the Parent–Child Interaction Assessment–II Enactments: Modifying an abused mother’s attributions to her son. Journal of Personality Assessment. 2009;91(5):397–408. doi: 10.1080/00223890903087430. [DOI] [PubMed] [Google Scholar]
- Hollenstein T. State space grids: Analyzing dynamics across development. International Journal of Behavioral Development. 2007;31(4):384–396. [Google Scholar]
- Hollenstein T, Granic I, Stoolmiller M, Snyder J. Rigidity in parent–child interactions and the development of externalizing and internalizing behavior in early childhood. Journal of Abnormal Child Psychology. 2004;32(6):595–607. doi: 10.1023/b:jacp.0000047209.37650.41. [DOI] [PubMed] [Google Scholar]
- Judd CM, Kenny DA, McClelland GH. Estimating and testing mediation and moderation in within-subject designs. Psychological Methods. 2001;6(2):115–134. doi: 10.1037/1082-989x.6.2.115. [DOI] [PubMed] [Google Scholar]
- Lee SY, Song XY. Evaluation of the Bayesian and maximum likelihood approaches in analyzing structural equation models with small sample sizes. Multivariate Behavioral Research. 2004;39(4):653–686. doi: 10.1207/s15327906mbr3904_4. [DOI] [PubMed] [Google Scholar]
- Lieberman AF. Child–parent psychotherapy: A relationship-based approach to the treatment of mental health disorders in infancy and early childhood. In: Sameroff AJ, McDonough SC, Rosenblum KL, editors. Treating parent–infant relationship problems. New York, NY: Guilford Press; 2004. pp. 97–122. [Google Scholar]
- Little RJA. A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association. 1988;83:1198–1202. [Google Scholar]
- Little RJA, Rubin DB. Statistical analysis with missing data. 2. New York, NY: Wiley; 2002. [Google Scholar]
- Loeber R, Dishion TJ. Early predictors of male delinquency: A review. Psychological Bulletin. 1983;94:68–99. [PubMed] [Google Scholar]
- MacKinnon DP, Dwyer JH. Estimating mediated effects in prevention studies. Evaluation Review. 1993;17(2):144–158. [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7(1):83–104. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon-Lewis C, Lamb ME, Arbuckle B, Baradaran LP, Volling BL. The relationship between biased maternal and filial attributions and the aggressiveness of their interactions. Development and Psychopathology. 1992;4(3):403–415. [Google Scholar]
- Magaña AB, Goldstein MJ, Karno M, Miklowitz DJ, Jenkins J, Falloon IRH. A brief method for assessing expressed emotion in relatives of psychiatric patients. Psychiatry Research. 1986;17(3):203–212. doi: 10.1016/0165-1781(86)90049-1. [DOI] [PubMed] [Google Scholar]
- Murphy SA, Collins LM, Rush AJ. Customizing treatment to the patient: Adaptive treatment strategies. Drug and Alcohol Dependence. 2007;88:S1–S3. doi: 10.1016/j.drugalcdep.2007.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén BO. Bayesian analysis in Mplus: A brief introduction. Mplus Technical Report. 2010a Retrieved from http://tinyurl.com/429vz8n.
- Muthén BO. Technical Report. Version 3. Muthén & Muthén; Los Angeles, CA: 2010b. Bayesian analysis in Mplus: A brief introduction. Retrieved from http://www.statmodel.com/ [Google Scholar]
- Muthén LK, Muthén BO. Mplus (Version 6.12) Los Angeles, CA: 2012. [Google Scholar]
- Muthén, Muthén, Nix R, Pinderhughes E, Dodge KA, Bates JE, Pettit GS, McFayden-Ketchum S. The relation between mothers’ hostile attribution tendencies and children’s externalizing behavior problems: The mediating role of mothers’ hard discipline practices. Child Development. 1999;70:896–909. doi: 10.1111/1467-8624.00065. [DOI] [PubMed] [Google Scholar]
- Noldus Information Technology. The Observer reference manual 5.0. Wageningen, the Netherlands: Author; 2003. [Google Scholar]
- Pasalich DS, Dadds MR, Hawes DJ, Brennan J. Assessing relational schemas in parents of children with externalizing behavior disorders: Reliability and validity of the Family Affective Attitude Rating Scale. Psychiatry Research. 2011;185:438–443. doi: 10.1016/j.psychres.2010.07.034. [DOI] [PubMed] [Google Scholar]
- Patterson GR. Coercive family process. Eugene, OR: Castalia; 1982. [Google Scholar]
- Patterson GR. The early development of coercive family process. In: Reid JB, Patterson GR, Snyder J, editors. Antisocial behavior in children and adolescents: A developmental analysis and model for intervention. Washington, DC: American Psychological Association; 2002. pp. 25–44. [Google Scholar]
- Patterson GR, Reid JB, Dishion TJ. Antisocial boys. Eugene, OR: Castalia; 1992. [Google Scholar]
- Peterson J, Winter C, Jabson J, Dishion TJ. The Relationship Affect Coding System. Child and Family Center, University of Oregon; Eugene, OR: 2008. coding manual. [Google Scholar]
- Robins MS, Alexander JF. The immediate effect of reframing on client attitude and family therapy. Journal of Family Psychology. 1996;10:28–34. [Google Scholar]
- Scaramella LV, Leve LD. Clarifying parent–child reciprocities during early childhood: The early childhood coercion model. Clinical Child and Family Psychology Review. 2004;7(2):89–107. doi: 10.1023/b:ccfp.0000030287.13160.a3. [DOI] [PubMed] [Google Scholar]
- Shaw DS, Bell RQ. Developmental theories of parental contributors to antisocial behavior. Journal of Abnormal Child Psychology. 1993;21(5):493–518. doi: 10.1007/BF00916316. [DOI] [PubMed] [Google Scholar]
- Shaw DS, Bell RQ, Gilliom M. A truly early starter model of antisocial behavior revisited. Clinical Child and Family Psychology Review. 2000;3(3):155–172. doi: 10.1023/a:1009599208790. [DOI] [PubMed] [Google Scholar]
- Shaw DS, Dishion TJ, Supplee L, Gardner FEM, Arnds K. Randomized trial of a family-centered approach to prevention of early conduct problems: 2-year effects of the Family Check-Up in early childhood. Journal of Consulting and Clinical Psychology. 2006;74(1):1–9. doi: 10.1037/0022-006X.74.1.1. [DOI] [PubMed] [Google Scholar]
- Shaw DS, Gilliom M, Ingoldsby EM, Nagin DS. Trajectories leading to school-age conduct problems. Developmental Psychology. 2003;39(2):189–200. doi: 10.1037//0012-1649.39.2.189. [DOI] [PubMed] [Google Scholar]
- Sidman M, Tailby W. Conditional discrimination vs. matching to sample: An expansion of the testing paradigm. Journal of Experimental Analysis of Behavior. 1982;37(1):5–22. doi: 10.1901/jeab.1982.37-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simpson JA, Rholes WS, Winterheld HA. Attachment working models twist memories of relationship events. Psychological Science. 2010;21(2):252–259. doi: 10.1177/0956797609357175. [DOI] [PubMed] [Google Scholar]
- Smith JD, Dishion TJ, Shaw DS, Wilson C, Winter C, Patterson GR. Coercive family process and early-onset problem behavior: A longitudinal analysis of low-income families from age 2 to school entry. Development & Psychopathology. doi: 10.1017/S0954579414000169. (under review) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith JD, Dishion TJ, Shaw DS, Wilson MN. Indirect effects of fidelity to the Family Check-Up on changes in parenting and early childhood problem behaviors. Journal of Consulting and Clinical Psychology. doi: 10.1037/a0033950. (under review) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith JD, Nicholas CRN, Handler L, Nash MR. Examining the potential effectiveness of a family intervention session in Therapeutic Assessment: A single-case experiment. Journal of Personality Assessment. 2011;93(3):149–158. doi: 10.1080/00223891.2011.559497. [DOI] [PubMed] [Google Scholar]
- Smith JD, Welsh DP, Fite PJ. Adolescents’ relational schemas and their subjective understanding of romantic relationship interactions. Journal of Adolescence. 2010;33:147–157. doi: 10.1016/j.adolescence.2009.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stern DN. The motherhood constellation: Therapeutic approaches to early relational problems. In: Sameroff AJ, McDonough SC, Rosenblum KL, editors. Treating parent–infant relationship problems. New York, NY: Guilford Press; 2004. pp. 29–43. [Google Scholar]
- Tharinger DJ, Finn SE, Arora P, Judd-Glossy L, Ihorn SM, Wan JT. Therapeutic Assessment with children: Intervening with parents “behind the mirror”. Journal of Personality Assessment. 2012;94(2):111–123. doi: 10.1080/00223891.2011.645932. [DOI] [PubMed] [Google Scholar]
- Tharinger DJ, Finn SE, Gentry L, Hamilton AM, Fowler JL, Matson M, Walkowiak J. Therapeutic Assessment with children: A pilot study of treatment acceptability and outcome. Journal of Personality Assessment. 2009;91(3):238–244. doi: 10.1080/00223890902794275. [DOI] [PubMed] [Google Scholar]
- Waller R, Gardner FEM, Dishion TJ, Shaw DS, Wilson MN. Validity of a brief measure of parental affective attitudes in high-risk preschoolers. Journal of Abnnormal Child Psychology. 2012;40(6):945–955. doi: 10.1007/s10802-012-9621-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waltz J, Addis ME, Koerner K, Jacobson NS. Testing the integrity of a psychotherapy protocol: Assessment of adherence and competence. Journal of Consulting and Clinical Psychology. 1993;61(4):620–630. doi: 10.1037//0022-006x.61.4.620. [DOI] [PubMed] [Google Scholar]
- Yuan Y, MacKinnon DP. Bayesian mediation analysis. Psychological Methods. 2009;14(4):301–322. doi: 10.1037/a0016972. [DOI] [PMC free article] [PubMed] [Google Scholar]