

Abstract
Most pregnant women are exposed to some physical activity at work. This Concise Guidance is aimed at doctors advising healthy women with uncomplicated singleton pregnancies about the risks arising from five common workplace exposures (prolonged working hours, shift work, lifting, standing and heavy physical workload). The adverse outcomes considered are: miscarriage, preterm delivery, small for gestational age, low birth weight, pre-eclampsia and gestational hypertension. Systematic review of the literature indicates that these exposures are unlikely to carry much of an increased risk for any of the outcomes, since small apparent effects might be explicable in terms of chance, bias, or confounding, while larger and better studies yield lower estimated risks compared with smaller and weaker studies. In general, patients can be reassured that such work is associated with little, if any, adverse effect on pregnancy. Moreover, moderate physical exercise is thought to be healthy in pregnancy and most pregnant women undertake some physical work at home. The guidelines provide risk estimates and advice on counselling.
Background
In the UK, as in most parts of the world, women comprise a substantial proportion of the modern workforce (47.6% in Spring, 2010),1 with an estimated 350,000 pregnant women working each year.2 Several reproductive hazards associated with work are well established (eg from ionising radiation and lead) and particular strategies have been developed to manage the associated risks. However, there are other potential workplace hazards for which the scientific evidence is less certain.
Important among these is the possibility that physical activities at work might adversely affect outcomes of pregnancy.3 It has been suggested, for example, that women's work schedules (including rotating shifts and night work) can induce neuroendocrine changes as a consequence of sleep deprivation or disrupted circadian rhythms, affecting fetal growth and the timing of parturition. In theory, long working hours, prolonged standing, heavy lifting or an unusual workload might also pose several threats to pregnant workers. The high demand for uterine and placental blood flow during the third trimester could limit reserve capacity for vigorous exercise, whereas raised noradrenaline levels could increase uterine contractility and, thereby, the risk of preterm labour. By contrast, marked physiological adaptations to the demands of pregnancy tend to preserve constant fetal oxygen consumption.
Provision of appropriate information to the pregnant worker is made more difficult because most of the activities of concern (especially physical exertion), although suspected of being hazardous, could also be beneficial, as suggested in other contexts by several reviews.4–7 Thus, advice on avoiding work activity could, in theory, be detrimental and cause needless anxiety.
Scope of the guidelines
This Concise Guidance is aimed at clinicians advising healthy women with uncomplicated singleton pregnancies about the relative safety of physical factors at work. Women with comorbidities, a previous adverse obstetric history or complications in the present pregnancy, including multiple pregnancies, should seek specialist advice from their obstetrician or midwife. Further information has also been provided by the National Institute for Health and Clinical Excellence (NICE) and the National Collaborating Centre for Women's and Children's Health.8
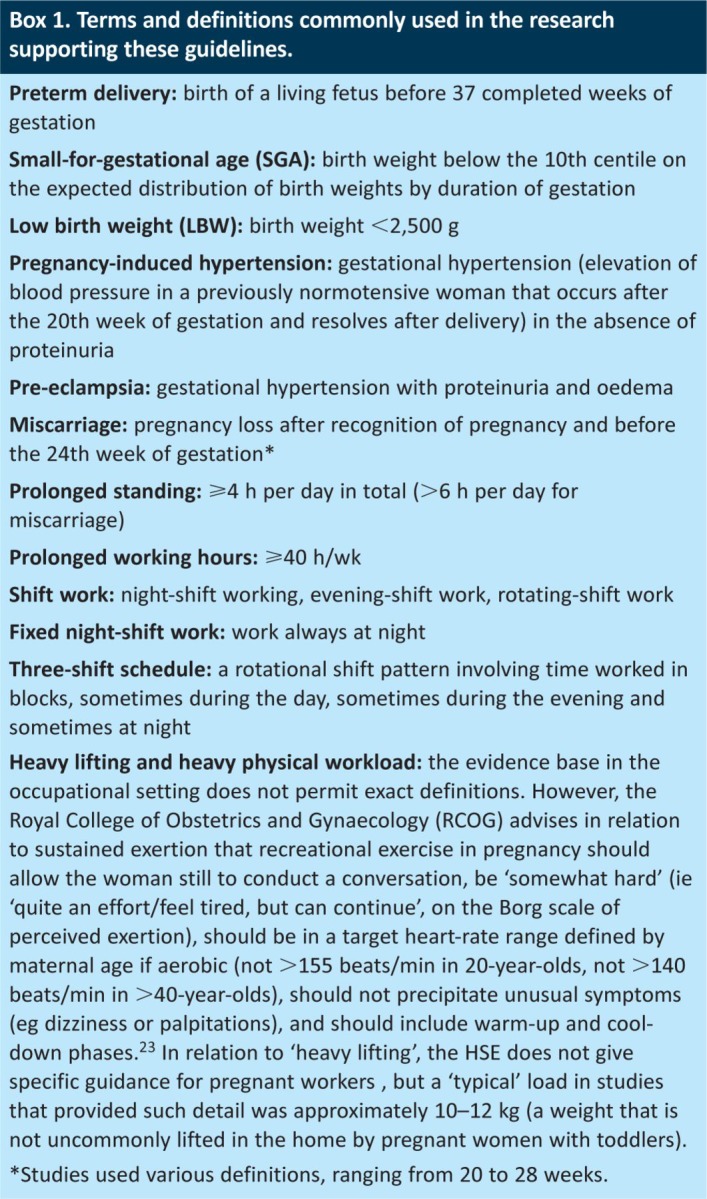
Box 1 provides definitions of the terms commonly used in these guidelines.
Box 1. Terms and definitions commonly used in the research supporting these guidelines.
Evidence synthesis and rationale
The evidence synthesis underpinning the present guidelines has been built on, and extends, three previous reviews on occupational activity and pregnancy outcome.3,9,10 It relates to five occupational exposures (working hours, shift work, lifting, standing and physical workload) that are all common among women of reproductive age. For example, in 2010, 16% of working women aged 15–39 years undertook shifts in their main job ‘most of the time’1 and 10% of women in full-time jobs worked more than 40 h/wk.11
The chosen outcomes (miscarriage, preterm delivery, small for gestational age (SGA), low birth weight (LBW), pre-eclampsia and/or gestational hypertension) are important to the health of the fetus, neonate and mother. Preterm birth is the most important single determinant of adverse infant outcome in terms of both survival and quality of life.12,13 LBW is a cause of infant morbidity and mortality,14 as well as predicting adverse outcomes in later life (eg poorer growth and development, neurological and cognitive deficit, high blood pressure, noninsulin-dependent diabetes, coronary heart disease, stroke and obstructive lung disease);15 pre-eclampsia and eclampsia were responsible for 8.4% of maternal deaths in the UK during 2006–2008;16 and miscarriage can cause enduring psychological distress. As well as being important, these adverse pregnancy outcomes are also common: 6.7% of live singleton births in hospitals in England during 2010–2011 were complicated by prematurity; 6.7% involved gestational hypertension and/or pre-eclampsia; and 6.6% of birth weights were <2,500 g;17 in addition, 10–14% of recognised pregnancies end in miscarriage.18
Current European Union (EU) legislation (92/85, EEC) and the related Management of Health and Safety at Work Regulations 1999 and guidance from the Health and Safety Executive (HSE)19 require employers to assess health and safety risks to pregnant workers, and to control them. However, there is currently limited advice for clinicians who care for healthy pregnant workers.20
Guideline development
Two systematic searches in Medline and EMBASE (January 1966 to June 13th 2012 for miscarriage, January 1966 to December 31st 2011 for other outcomes) identified 113 overlapping reports relating to these work exposures and pregnancy outcomes: 57 reports on preterm delivery, 54 on birth weight, 30 on miscarriage and 11 concerning pre-eclampsia or gestational hypertension. Eligible studies were critically assessed for their completeness of reporting and potential for bias and confounding following previously published methods,9,10 adapted in part from SIGN methodology and elements proposed by Ariens et al.21 and van der Windt et al.22 For studies with similar definitions, pooled meta-estimates of relative risk (RR) were calculated, updating earlier computations.9 A multidisciplinary stakeholders group, comprising representatives from obstetrics, midwifery, general practice, general medicine, occupational medicine, the Royal College of Physicians (RCP), the trades union movement and the public (a representative from the parents' charity National Childbirth Trust (NCT)), formulated these guidelines in light of the evidence.
Appraisal of the evidence
The evidence base is extensive for preterm delivery, LBW and SGA, more limited for miscarriage, and very limited for pre-eclampsia and gestational hypertension. It has several strengths: pregnancy outcomes were usually confirmed from objective sources, most studies were well reported, response rates were typically high and studies were often large. By contrast, nearly half of reports were potentially affected by confounding or bias and the exposures ‘occupational lifting’, ‘physical workload’ and even ‘shift work’ were not defined uniformly between studies.
Within these limitations (and strengths), findings were broadly reassuring. For preterm delivery, pooled estimates tended to indicate no more than modest elevations in risk (eg RR <1.2 or ≤1.3 extra case per 100 deliveries to exposed women). The larger and most complete studies reported the smallest levels of risk, suggesting that risk estimates in other studies were inflated by bias. For SGA, meta-estimates were close to the no-effect level. For miscarriage, meta-risk estimates were elevated moderately overall, but generally lower in better quality studies (RR <1.2); higher risks were implied from working fixed night shifts, but in only a few studies, each with individual limitations (RR 1.5). For pre-eclampsia and gestational hypertension, there were insufficient data to draw firm conclusions, although risks were seldom much elevated.
Table 1 presents evidence showing the best estimates of the excess risk (per 100 exposed women), together with an assessment of the strength of evidence and statistical uncertainty. In summary, none of the exposures appeared likely to carry much of an increased risk for any of the outcomes. Although small levels of excess risk might exist for preterm delivery, SGA, LBW and miscarriage, it is possible that many or all of these effects arise from a combination of chance, bias and residual confounding. (Even in the absence of bias or confounding, estimates of effect embrace the possibility of no effect or even a small benefit from many of the activities of interest.)
Table 1.
Table of evidence.

Legal position
Employers have an ongoing duty to assess and control risks to their employees' health and safety arising from their work. They also have a specific obligation in relation to pregnant workers (Management of Health and Safety at Work Regulations 1999), which extends where necessary and feasible to the offer of alternative work or, failing this, medical suspension with pay and job protection (Employment Rights Act 1996). This obligation might require employers to search for suitable alternative daytime work for a pregnant shift worker certified by a doctor or midwife as unfit to work nights.19 According to Directgov,23 lifting, carrying, standing, working hours and shift work bear consideration in employers' risk assessments of pregnant workers; similarly, HSE cautions that risks can arise from working conditions, including manual handing and working hours.24
The issues in context
However, the evidence base supporting mandatory medical restriction for the work activities covered by this guideline is weak. Such advice should not be issued without careful consideration, because some women might become anxious and unnecessary avoidance of work might ensue. By inference, also, similar physical activities outside work might seem contraindicated, whereas the Royal College of Obstetricians and Gynaecologists25 and the American College of Obstetricians and Gynaecologists26 recommend that ‘all women should be encouraged to participate in aerobic and strength-conditioning exercise as part of a healthy lifestyle during their pregnancy’ and that ‘reasonable goals’ of aerobic conditioning should be maintained; these appear to confer physical and psychological benefits (eg reduced fatigue, varicosities, swelling of extremities, insomnia, stress, anxiety and depression, perhaps even length of labour and delivery complications25).
On the other hand, outcomes such as preterm delivery can have important health consequences and patients will differ in their understanding and tolerance of uncertainty at apparently low levels of risk. In general, the evidence base is reassuring, especially given the potential disadvantages of refraining from work activities. Some women might remain clinically anxious and need tailored individual counselling, or a choice, for example, of moving from fixed night working to an alternative work pattern. In any event, many women will need to reduce long working hours, prolonged standing and heavy physical work, particularly during late pregnancy when physical stamina limits capacity for onerous duties.
Recommendations
In relation to healthy uncomplicated singleton pregnancies, the Guideline Development Group has drawn up the recommendations detailed in Table 2.
Table 2.
Recommendations advising pregnant women.

Coherence with other advice
These recommendations are consistent with previous recommendations issued on behalf of the RCP and NHS Plus in 2009 in relation to the same exposures and outcomes.18 However, the evidence base supporting them is deeper, enabling firmer conclusions to be drawn.
Implementation
No specific issues arise in relation to implementation, because the emphasis will largely be on allaying concerns raised by the patient, rather than some more proactive policy; and the advice recommended carries no resource implications for the advising clinician.
Information sheets for professionals for each exposure (Box 2) outlining any evidence on risk in relation to the outcomes covered by the literature review have been prepared, and are available on the RCP website at www.clinmed.rcpjournal.org. The advice given in the information sheets is designed to be used by professionals when advising women with a healthy, uncomplicated, singleton pregnancy.
Box 2. Available information sheets for professionals.

Acknowledgments
This guideline was developed with funding from the NHS Health at Work Network.
References
- 1.Economic and Social Data Service. Labour force survey: quarterly household dataset, April-June 2010. London: Office for National Statistics; 2010. [Google Scholar]
- 2.Department of Trade and Industry. Work and Parents: Competitiveness and Choice. Research and Analysis, Nov 2000. London: DTI; 2000. [Google Scholar]
- 3.Mozurkewich EL. Luke B. Avni M, et al. Working conditions and adverse pregnancy outcome: a meta-analysis. Obstet Gynecol. 2000;95:623–34. doi: 10.1016/S0029-7844(99)00598-0. [DOI] [PubMed] [Google Scholar]
- 4.Kramer MS. McDonald SW. Aerobic exercise for women during pregnancy. Cochrane Database Syst Rev. 2006;3:CD000180. doi: 10.1002/14651858.CD000180.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chasan-Taber L. Evenson KR. Sternfeld B, et al. Assessment of recreational physical activity during pregnancy in epidemiologic studies of birth weight and length of gestation: methodologic aspects. Women Health. 2007;45:85–107. doi: 10.1300/J013v45n04_05. [DOI] [PubMed] [Google Scholar]
- 6.Schlussel MM. de Souza EB. Reichenheim ME, et al. Physical activity during pregnancy and maternal-child health outcomes: a systematic literature review. Cad Saude Publica. 2008;24(suppl 4):531–44. doi: 10.1590/S0102-311X2008001600006. [DOI] [PubMed] [Google Scholar]
- 7.Lagerros YT. Physical activity: the more we measure, the more we know how to measure. Eur J Epidemiol. 2009;24:119–22. doi: 10.1007/s10654-009-9316-0. [DOI] [PubMed] [Google Scholar]
- 8.National Institute for Health and Clinical Excellence. Antenatal care. Routine care for the healthy pregnant woman. London: NICE; 2008. [Google Scholar]
- 9.Bonzini M. Coggon D. Palmer KT. Risk of prematurity, low birth weight, and pre-eclampsia in relation to working hours and physical activities: a systematic review. Occup Environ Med. 2007;64:228–43. doi: 10.1136/oem.2006.026872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bonzini M. Palmer KT. Coggon D, et al. Shift work and pregnancy outcomes: a systematic review with meta-analysis of currently available epidemiological studies. BJOG. 2011;118:1429–37. doi: 10.1111/j.1471-0528.2011.03066.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Annual Survey of Hours and Earnings. 2010. www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A77-238620 [Accessed 19 November 2012].
- 12.Saigal S. Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. 2008;371:261–9. doi: 10.1016/S0140-6736(08)60136-1. [DOI] [PubMed] [Google Scholar]
- 13.Costeloe K EPICure Study Group. EPICure: facts and figures: why preterm labour should be treated. BJOG. 2006;113(suppl 3):10–2. doi: 10.1111/j.1471-0528.2006.01118.x. [DOI] [PubMed] [Google Scholar]
- 14.Moser K. Li L. Power C. Social inequalities in low birth weight in England and Wales: trends and implications for future population health. J Epidemiol Community Health. 2003;57:687–91. doi: 10.1136/jech.57.9.687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barker DJB. Fetal and infant origins of adult disease. London: BMJ Publishing Group; 1992. [Google Scholar]
- 16.Centre for Maternal and Child Enquiries (CMACE) Saving Mothers Lives: reviewing maternal deaths to make motherhood safer: 2006–2008. The Eighth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG. 2011;118(suppl 1):1–203. doi: 10.1111/j.1471-0528.2010.02847.x. [DOI] [PubMed] [Google Scholar]
- 17.Hospital Episode Statistics 2011. Table 22: Complications recorded in the pregnancy episode. 2010–11, NHS Hospitals, England; Table 28: Singleton and multiple deliveries by birth weight and birth status, 2010–11, NHS Hospitals, England.
- 18.Wilcox A. Fertility and pregnancy – an epidemiological perspective. Oxford: Oxford University Press; 2010. [Google Scholar]
- 19.Health and Safety Executive. New and expectant mothers: the law. London: HSE; 1999. [Google Scholar]
- 20.Royal College of Physicians, NHS Plus. Physical and shift work in pregnancy: occupational aspects of management. A national guideline. London: RCP; 2009. [Google Scholar]
- 21.Ariens G. van Mechelen W. Bongers PM, et al. Physical risk factors for neck pain. Scand J Work Environ Health. 2000;26:7–19. doi: 10.5271/sjweh.504. [DOI] [PubMed] [Google Scholar]
- 22.Van der Windt DAWM. Thomas E. Pope DP, et al. Occupational risk factors for shoulder pain: a systematic review. Occup Environ Med. 2000;57:433–42. doi: 10.1136/oem.57.7.433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Directgov. 2012. www.direct.gov.uk/en/Parents/Moneyandworkentitlements/WorkAndFamilies/Pregnancyandmaternityrights/DG_10026556 [Accessed 19 November 2012].
- 24.Health and Safety Executive. 2012. www.hse.gov.uk/mothers/faqs.htm [Accessed 19 November 2012].
- 25.Royal College of Obstetricians and Gynaecologists. 2006. www.rcog.org.uk/files/rcog-corp/Statement4-14022011.pdf [Accessed 19 November 2012].
- 26.Artal R. O'Toole M. Guidelines of the American College of Obstetricians and Gynaecologists for exercise during pregnancy and the postpartum period. Br J Sports Med. 2003;37:6–12. doi: 10.1136/bjsm.37.1.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Regan L. Braude PR. Trembath PL. Influence of past reproductive performance on risk of spontaneous abortion. BMJ. 1989;299:541–5. doi: 10.1136/bmj.299.6698.541. [DOI] [PMC free article] [PubMed] [Google Scholar]