

Summary
Semantic dementia is characterized by semantic deficits and behavioural abnormalities which occur in the wake of bilateral inferolateral and predominantly left-sided anterior temporal lobe atrophy. The temporal poles have been shown to be involved in theory of mind, namely the ability to ascribe cognitive and affective mental states to others that regulates social interactions by predicting and interpreting human behaviour. However, very few studies have examined theory of mind in semantic dementia. In this study, we investigated both cognitive and affective theory of mind in a group of semantic dementia patients, using separate objective and subjective assessment tasks. Results provided objective evidence of an impact of semantic dementia on cognitive and affective theory of mind, consistent with the patients’ atrophy in the left temporal lobe and hypometabolism in the temporal lobes and the medial frontal cortex. However, the subjective assessment of theory of mind suggested that awareness of the affective but not cognitive theory of mind deficit persists into the moderate stage of the disease.
Keywords: Aged, Atrophy, pathology, psychology, Attention, Executive Function, Female, Frontotemporal Lobar Degeneration, pathology, psychology, Humans, Male, Memory, Middle Aged, Neuropsychological Tests, Temporal Lobe, pathology, Theory of Mind
Keywords: semantic dementia, cognitive/affective theory of mind, objective/subjective assessment, imaging.
1. Introduction
Semantic dementia (SD) is the term that was proposed by Snowden et al., (1989) to designate patients suffering from a progressive neurodegenerative disorder characterized by a “loss of semantic information”. From a cognitive point of view, patients start to display multimodal semantic memory deterioration, manifested in specific language disturbances, in the early stages of SD. Spontaneous speech is fluent but empty, with preserved phonological and grammatical aspects as well as repetition, while naming and comprehension gradually become impaired. These symptoms are generally accompanied by semantic paraphasias, agnosia for objects and prosopagnosia, but visuospatial skills and day-to-day memory are relatively preserved (Hodges and Patterson, 2007). From a nosological perspective, SD, also known as the temporal variant of frontotemporal dementia, is one of the three clinical forms of frontotemporal lobar degeneration, along with the frontal or behavioural variant one (bv-FTD) and progressive non-fluent aphasia (Neary et al., 1998). Frontotemporal lobar degeneration is a neurodegenerative process affecting the frontal and/or temporal lobes. Its clinical picture includes aberrations in language and cognition, but also in behaviour and social function (for a review, see Wittenberg et al., 2008). For instance, loss of empathy and impaired emotion recognition are some of the main symptoms (Snowden et al., 2001; Lough et al., 2006).
Personality modifications and social dysfunctions in frontotemporal lobar degeneration are assumed to be related to theory of mind (ToM) impairments (Kipps et al., 2006). ToM is the ability to infer people’s mental states (Premack and Woodruff, 1978; Frith and Frith, 1999). It allows individuals both to ascribe cognitive and affective states to others and to deduce their intentions from their attitudes (Brothers and Ring, 1992; Corricelli, 2005). Insofar as ToM enables individuals to predict, anticipate and interpret human behaviour, it is essential for regulating social interactions (Beer and Ochsner, 2006). A distinction can be made between “cognitive ToM”, which concerns the cognitive states, beliefs, thoughts, or intentions of other people (Brothers and Ring, 1992; Coricelli, 2005), and “affective ToM”, which concerns the affective states, emotions or feelings of others (Brothers and Ring, 1992). Furthermore, Baron-Cohen and colleagues (1997; Adolphs et al., 2002) have found that basic and complex emotions are differently addressed: while basic emotions are automatically and cross-culturally recognized, and probably rely on an innate mechanism (Izard, 1994), complex emotions express blends of mental states or social emotions which generally arise within an interpersonal context. Although some researchers hold that affective ToM is similar to empathy (Decety and Lamm, 2006), these two concepts are actually somewhat different. Although both conduct to the genuine understanding of mental affective states, we consider that the term “empathy” refers to the feeling and experiencing of another person’s emotion, whereas affective ToM refers to the ability to adopt the other person’s point of view, or “put oneself in his/her shoes”, without necessarily experiencing any emotion (Pacherie, 2004). That said, some theoretical conceptions of empathy distinguish between the “emotional empathy” described above and “cognitive empathy”, which is synonymous with affective ToM (Davis, 1980; Eslinger, 1998; Shamay-Tsoory et al., 2004). In addition to the cognitive/affective ToM distinction, we can distinguish between first- and second-order mental representations. “First-order” refers to representations of an individual’s thoughts that are achieved by adopting the latter’s perspective (e.g. ‘I think that Mr X thinks that…’). “Second-order” representations, which can be likened to “metarepresentations” (Morin, 2006, 2010), involve simultaneously adopting two perspectives (e.g. ‘Mr X thinks that Miss Y thinks that…’).
Numerous neuroimaging studies have investigated the neural correlates of ToM via different ToM tasks, such as inferring characters’ cognitive mental states through verbal or visual stories (Brunet et al., 2000; Walter et al., 2004), inferring affective states from photographs of emotional faces or the eye region (Baron-Cohen et al., 1999; 2001), observing the movements and interactions of geometrical shapes (Schultz et al., 2003; Gobbini et al., 2007), and other subject-agent interaction procedures (Gallagher et al., 2002; Schilbach et al., 2006). These studies have highlighted a ToM-related cerebral network (for reviews, see Abu-Akel, 2003; Frith and Frith, 2003; Carrington and Bailey, 2009) which is broadly constituted by the prefrontal cortex, including the orbital and medial prefrontal cortices (Baron-Cohen and Goodhart, 1994; Fletcher et al., 1995; Goel et al., 1995; Gallagher et al., 2000; Happaney et al., 2004; Adenzato et al., 2010), the temporal lobes, including the superior temporal sulci and the temporal poles (Olson et al., 2007), and the amygdala (Baron-Cohen et al., 1999). While less attention has been paid to the temporal poles than the prefrontal cortex in ToM, Ross and Olson (2010) recently drew attention to the contribution of the anterior temporal lobes in social attribution and ToM tasks. Their findings, in healthy adults, underline the fact that ToM abilities rely on the anterior temporal lobes to activate a set of social semantic representations. In other words, a body of social semantic knowledge stored in the anterior temporal lobes is required in order to understand other people’s mental states.
The profound semantic deterioration seen in SD patients is generally the result of bilateral atrophy of the temporal lobes. Neuroimaging studies in SD patients have indicated an anteroposterior gradient, with greater atrophy anteriorly. Moreover, this atrophy tends to be predominantly left-sided, rather than right-sided or symmetrical (Gorno-Tempini et al., 2004; Desgranges et al., 2007; Wittenberg, 2008). Otherwise, authors have reported significant hypometabolism in the whole left temporal cortex and in the right temporal pole. More extensive than the atrophy, this hypometabolism also encompasses the frontal areas (Edward-Lee et al., 1997) especially the bilateral orbitofrontal cortex (Desgranges et al., 2007).
In the light of the cognitive and cerebral impairments in SD, it is legitimate to ask whether ToM is normal in SD patients. Surprisingly little is known about this issue, while ToM has been widely studied in bv-FTD (for a review, see Adenzato et al., 2010). Some authors have, however, assessed empathy in SD via different scales, such as the Interpersonal Reactivity Index (Davis, 1983). They have generally found that SD patients have impairments in both the cognitive and emotional components of empathy. This decline has been related to right-sided temporal atrophy (Perry et al., 2001; Rankin et al., 2005). However, in a recent case report, Calabria et al. (2009) showed that the cognitive component of empathy is more impaired than the emotional one in the presence of left-sided temporal atrophy. Their finding suggests that the cognitive aspects of empathy (and, by extension, of affective ToM) are sustained by the left temporal lobe. As far as ToM per se is concerned, Eslinger and colleagues (2007) studied cognitive ToM in a group of 14 patients, some of whom had SD. Using cognitive ToM tasks that elicited either intention-based predictions or first- and second-order beliefs of characters in a social context they demonstrated impairment in both tasks. This impairment was less severe than that found in a group of patients suffering from bv-FTD. However, one major limitation to this study was that patients with SD were mixed with patients with non-fluent progressive aphasia, without giving any indication as to either the number and characteristics of the SD patients, or their specific performances. Adopting a different approach, Rankin et al. (2009) studied sarcasm and whether it could be detected from paralinguistic cues in several groups of patients with neurodegenerative diseases, including a group of 11 SD patients. Like irony, sarcasm is a high-level communicative intention requiring cognitive ToM (Sabbagh et al., 2004). The authors found that independently of their language deficit, SD patients failed to detect sarcasm in nonverbal features, whereas they outperformed controls in the innuendo-free condition. These findings suggest that the cognitive aspects of ToM tend to deteriorate in SD, although the study used only one cognitive ToM task and did not explore affective ToM. That said, in a previous exploratory investigation of a single SD case, we found deficits in cognitive ToM in the absence of deficits in affective ToM (Bon et al., 2009).
The aim of the present study was to examine ToM abilities in SD by investigating for the very first time both the cognitive and affective dimensions of ToM in the same group of SD patients. Using the thorough ToM assessment validated by Duval et al. (2011), we carried out not just an objective ToM assessment but a subjective one, too. The objective assessment comprised specially adapted standard tests evaluating either cognitive or affective ToM, plus an original composite test covering both these aspects, that was designed to explore ToM under conditions matching the social context of everyday life. In the subjective assessment, a self-rating ToM scale was used to probe ToM deficit awareness.
In the light of the cognitive and cerebral deterioration in SD and the scant data available in the literature, we expected to find impairment of SD patients’ cognitive ToM involving the inference of intentions and high-level beliefs, as well as of affective ToM involving the inference of emotions.
2. Material and methods
2.1. SD patients
We studied fifteen patients (6 men, 9 women) in the early to moderate stages of SD (mean age = 64.27 ± 6.53 years, range: 51–78 years; mean disease duration = 3.93 ± 1.98 years), who were selected on the basis of research criteria for SD established by Neary et al. (1998). Demographic data are detailed in Table 1. The selection of patients was carried out according to a codified procedure in French expert centres (University hospitals of Caen and Rennes) by senior neurologists whose main activity consists of the diagnosis and follow-up of patients suffering from neurodegenerative disorders, as well as by neuropsychologists and speech therapists. Patients with a history of alcoholism, head trauma, neurological or psychiatric illness were excluded. In all patients, according to their families, the predominant and inaugural symptom had been a semantic memory deficit, reflected by anomia and word comprehension difficulties, as well as by deficits in the recognition of familiar people. With the exception of one patient who had additional day-to-day memory impairment, in each case, the family reported preserved everyday memory and autonomy. These patients could therefore continue to carry out everyday activities such as doing their own shopping, using public transport, keeping general practitioner’s appointments and remembering recent or current events. They were also well oriented in time and space. For each patient, cognitive complaints and levels of depression were measured via the short Cognitive Difficulties Scale (McNair and Kahn, 1983) and the short Geriatric Depression Scale (Yesavage et al., 1983), respectively. There was no significant difference with healthy subjects. Their overall cognitive efficiency was assessed using the Mattis Dementia Rating Scale (Mattis, 1976). All patients displayed overall cognitive decline (Table 1).
Table 1.
General data about the SD patients and healthy controls groups
| SD patients (N=15) | Healthy controls (N=36) | |
|---|---|---|
| Gender (Male/Female) | 6/9 | 12/24 |
| Age (years) | 64.27 ± 6.53 | 64.14 ± 8.25 |
| Education (years) | 11.02 ± 4.07 | 11.69 ± 3.91 |
| sCDSa | 24.15 ± 9.41 | 19.81 ± 9.99 |
| sGDSb | 1.15 ± 1.34 | 0.72 ± 0.74 |
| Mattisc | 118 ± 9.57 | 139.05 ± 4.38 |
| Illness duration (years) | 3.93 ± 1.98 | _ |
short Cognitive Difficulties Scale, administered to 13 SD patients. The cut-off score is 30.
short Geriatric Depression Scale, administered to 13 SD patients. The cut-off score is 2.
Mattis Dementia Rating Scale, administered to 12 SD patients and solely to participants over 65 years. The cut-off score is 130.
Furthermore, 10 patients underwent a high-resolution T1-weighted volume Magnetic Resonance Imaging scan (3T scanner) and 9 of them a resting Positron Emission Tomography investigation using [18F]fluoro-2-deoxy-D-glucose at the CYCERON centre (Caen, France). For both types of imaging data, we assessed group differences in SPM5 using a threshold of p = 0.01 family-wise error-corrected, to obtain maps of significant atrophy and hypometabolism in patients with SD compared with an independent sample of 26 control adults, paired in age and years of education, from our imaging database. The remaining patients underwent a standard Magnetic Resonance Imaging scan which confirmed the diagnosis. This mainly revealed atrophy of the temporal neocortex, predominantly in the left hemisphere in all cases but one.
For the 10 abovementioned patients, our SPM analysis showed that regions of significant grey matter loss involved the whole temporal neocortex (temporal pole and inferior, middle and superior temporal gyri), extending to the hippocampal region (hippocampus, parahippocampal gyrus, amygdala), as well as the fusiform gyrus, insula and caudate nucleus (see Figure 1A). Although present bilaterally, the atrophy predominated in the left hemisphere, especially for posterior and superior temporal regions. Regions of significant hypometabolism overlapped roughly the significant grey matter loss (see Figure 1B). On the left side, it encompassed the entire temporal lobe, including both the whole temporal neocortex and the hippocampal region, and also encroached on the fusiform gyrus, insula, caudate and pallidum nucleus. On the right side, the hypometabolism was less significant and mainly concerned the temporal pole and medial temporal region (including the amygdala and parahippocampal gyrus). Frontal regions, especially the bilateral medial orbitofrontal cortex and rectus gyrus, as well as the left anterior cingulate cortex, were also involved, albeit to a lesser extent.
Fig 1.
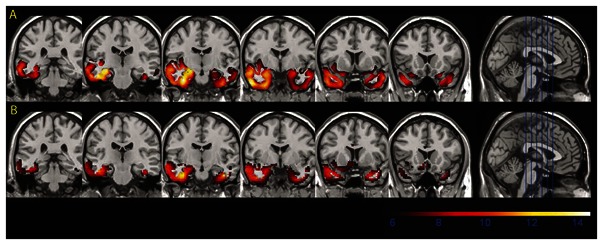
Clusters of significant (p<0.01 family-wise error corrected) atrophy (A), and hypometabolism (B), in patients with SD compared to controls, as superimposed onto coronal slices of the Montreal National Institute template.
This protocol was approved by the Regional Ethics Committee. Controls and patients gave written consent to the procedure prior to the investigation.
2.2. General neuropsychological assessment
In order to gain a clear picture of their neuropsychological disturbance, the SD patients underwent a general neuropsychological assessment beforehand (mean: 5.3 ± 2.76 months prior to inclusion in the study), comprising semantic, episodic and working memory tests. Neuropsychological test performances for the group of SD patients are summarised in Table 2. We explored semantic memory by means of 1) the Concept subscale of the Mattis scale (Mattis, 1976), 2) literal and categorical verbal fluency tasks in 2 minutes each (Cardebat et al., 1990) and, 3) picture naming tasks (DO80, Deloche and Hannequin, 1997, or BECS-GRECO naming, Belliard et al., 2008). We assessed verbal episodic memory using the Logical Memory subtest of the Wechsler Memory Scale (Wechsler, 2001), while visuospatial episodic memory was probed with the “Test de la Ruche” (Violon and Wijns, 1984) and/or the delayed recall of the Rey-Osterrieth complex figure (from Lezak, 1995). Working memory was evaluated by means of a digit span test (Wechsler, 2001). To assess executive functions, as defined by Miyake et al. (2000), we investigated the shifting process, updating function and inhibition of inappropriate responses using the Trail-Making Test (Reitan, 1958), the running span task (Quinette et al., 2003) and the Stroop Test (Stroop, 1935), respectively, while problem-solving was evaluated by means of Raven’s coloured progressives matrices (Raven, 1965). Finally, visuoconstructive abilities were probed with the copy of the Rey-Osterrieth Complex Figure (Lezak, 1995).
Table 2.
Neuropsychological data of the SD patient group
| Cognitive tests | n | m ± s | μz-score | %impaired SD | |
|---|---|---|---|---|---|
| Memory functions | |||||
|
| |||||
| Semantic memory | |||||
| Fluency task | |||||
| - Literal (letter “P”) | 12 | 12.33 | (± 4.44) | −1.8 (± 0.71) | 66.67 |
| - Categorical (animals) | 12 | 9.25 | (± 3.08) | −2.86 (± 0.35) | 100 |
| Picture naming (%) | 15 | 39.97 | (± 25.06) | −15.64 (± 7.53) | 100 |
| Concept (Mattis) (/39) | 15 | 32.4 | (± 3.07) | - | 33.33 |
| Episodic memory | |||||
| Logical memory | |||||
| - Immediate recall (/75) | 10 | 22.2 | (± 10.32) | −1.8 (± 1.23) | 50 |
| - Delayed recall (/50) | 10 | 12.5 | (± 7.44) | −1.66 (± 1.12) | 40 |
| - Recognition (/50) | 10 | 16.5 | (± 7.92) | −2.21 (± 2.21) | 30 |
| Test de la Ruche | |||||
| - Immediate recall (/10) | 11 | 9.09 | (± 2.21) | 0.29 (± 1.22) | 9.09 |
| - Delayed recall (/10) | 10 | 9.2 | (± 1.62) | 0.66 (± 0.7) | 0 |
| - Recognition (/10) | 10 | 10 | - | 0.55 (± 0.22) | 0 |
| Rey-Osterrieth complex figure | |||||
| - Delayed recall (/36) | 13 | 14.54 | (± 8.31) | −0.64 (± 1.53) | 15.38 |
| Working memory | |||||
| Forward digit span | 15 | 5.8 | (± 1.32) | 0.12 (± 1.23) | 0 |
| Backward digit span | 15 | 4.2 | (± 1.47) | 0.22 (± 1.43) | 13.33 |
| Executive functions | |||||
|
| |||||
| Attention | |||||
| Trail-Making Test A (s) | 15 | 52.93 | (± 14.05) | 0.69 (± 1.00) | 20 |
| Errors | 0.07 | (± 0.26) | - | 6.67 | |
| Shifting | |||||
| Trail-Making Test B (s) | 14 | 110.29 | (± 33.23) | 0.04 (± 0.58) | 6.67 |
| Errors | 0.33 | (± 0.82) | - | 13.33 | |
| Trail-Making Test B-A (s) | 14 | 59.36 | (± 30.74) | −0.11 (± 0.61) | 6.67 |
| Updating | |||||
| Running span (/16) | 11 | 5.27 | (± 3.72) | −0.98 (± 1.19) | 27.27 |
| Inhibition | |||||
| Colour Stroop Test (interference in s) | 14 | 162.57 | (± 54.08) | 0.75 (± 1.13) | 21.43 |
| Nonverbal reasoning | |||||
| Raven’s coloured progressive matrices (/36) | 12 | 32.25 | (± 4.39) | 0.74 (± 0.93) | 0 |
| Instrumental functions | |||||
|
| |||||
| Praxis | |||||
| Copy of Rey-Osterrieth complex figure (/36) | 15 | 34.87 | (± 1.96) | 0.19 (± 0.81) | 0 |
n = number of SD patients for the task considered
In brief, the results, reported in Table 2, clearly indicated that the SD patients displayed massive semantic memory difficulties, with anomia and impoverished general semantic knowledge of concepts. While visual episodic memory was relatively preserved, verbal episodic memory was impaired, although this may have been accentuated by interference with semantic and language disorders. However, these deficits were probably not enough to explain the poor memory performances, suggesting genuine deficits of episodic memory, in accordance with abnormalities in the hippocampal region, and previous findings both by our group (Desgranges et al., 2007) and by others (Chan et al., 2001; Good et al., 2002; Nestor et al., 2006). Similarly, executive functions appeared preserved in most of the patients, and no deficits were found in visuoconstructive abilities.
2.4. ToM assessment
In order to perform consistent and exhaustive measures of ToM within the group of SD patients, we administered a series of assessment tasks taken from Duval et al. (2011) that were designed to probe both the cognitive and affective dimensions of ToM. More specifically, we conducted an objective assessment of ToM by means of classic visual and verbal tasks, adapting them in order to reduce cognitive load. Cognitive ToM was assessed by an attribution of intention test (Brunet et al., 2000) and a false-belief task (Wimmer and Perner, 1983), and affective ToM via a version of the Reading the Mind in the Eyes Test (Baron-Cohen et al., 1997). We also added a composite task called “Tom’s taste”, which we developed to give a better account of this ability. Furthermore, an original self-rating questionnaire was used to assess awareness of the putative ToM deficit. We checked that participants fully understood each ToM task and, where necessary, provided an aid, mainly in the form of a glossary or the rewording of sentences. If their understanding remained impaired, the test was not performed.
SD patients’ performances were compared with those obtained in 36 healthy age-matched controls recruited from a local panel of volunteers (Duval et al., 2011). Each one gave his/her informed consent to the experimental procedure. Their inclusion was based on the absence of neurological or psychiatric medical history reported on a health questionnaire, signs of depression as measured on the short Geriatric Depression Scale, and memory complaints, as measured on the short Cognitive Difficulties Scale. Moreover, adults over 65 years old were screened for dementia using the Mattis Dementia Rating Scale. We also checked executive functioning with the Trail Making Test (mental flexibility) and the Stroop test (inhibition). All participants’ scores were within the norm (data not shown).
2.4.1. Objective ToM assessment
Attribution of intention task
This visual task was derived from Brunet et al. (2000). It consisted of a set of 30 short comic strips, selected from 88 comics. Each of them comprised three pictures illustrating a scenario. The aim was to find the most logical conclusion for each scenario by choosing a fourth picture among three others. The comic strips were divided into three conditions. In the first one, 10 stories required participants to draw inferences from a character’s actions (ToM condition). In the second one, 10 stories showed a character without any intention (control condition with characters), while in the third one, 10 scenarios were based on the physical properties of objects (control condition with object). The latter two formed a control condition. Scores were percentages of correct responses in each condition.
False-belief task
This original visual-and-verbal task was based on false-belief cartoon tasks such as “Sally and Ann” (Wimmer and Perner, 1983). It was made up of 15 short comic strips illustrating scenarios that had been dreamed up within our laboratory (Bon et al., 2009). Each comic strip comprised three pictures with a short written description (for an example, see Figure 2). The aim was to understand the story by reading the scenario, then answer a question with two possible responses. There were two conditions. In the ToM condition, the question was about the belief of one of the characters in the story. Eight of the 15 cartoons involved first-order representations (‘X thinks that…’) and seven second-order ones (‘X thinks that Y thinks that…’). In the control condition, the same cartoons were used, but the question probed participants’ understanding of the reality of the cartoon scenario. In order to reduce cognitive load, the pictures and written descriptions remained visible throughout. We inserted an interference task (classic digit span task) between the first-and second-order cartoons and between the ToM and control conditions. Each performance was expressed as a percentage for each condition.
Fig 2.
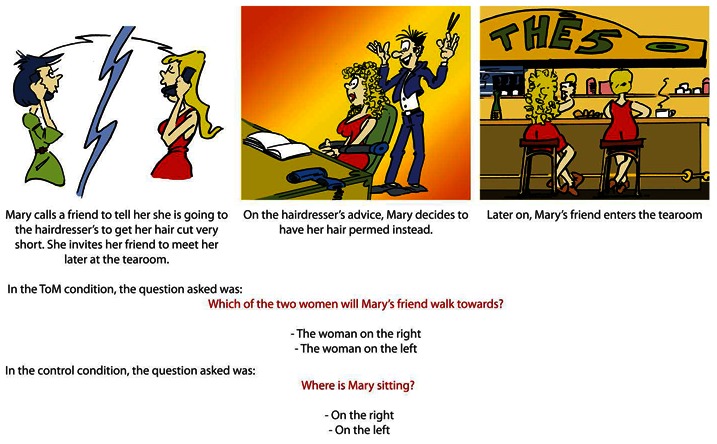
Example of story (first order) used in the false belief task.
The Eyes test
This task was inspired by the test devised by Baron-Cohen et al. (1997). It consisted of 20 black-and-white photographs of the eye region of a female actor who was asked to produce different facial expressions. Ten of the photographs depicted “basic emotions” (i.e happiness, surprise, sadness, anger, and fear) and ten “complex emotions” (e.i. guilt, thoughtful, flirting, scheming, puzzled, interested (twice), quizzical, arrogant and bored). Under each picture, three adjectives (one target and two foils) described basic or complex emotions. Participants were asked to identify which adjective best described the person’s mental state. This test allowed us to measure emotion recognition in the basic emotions condition and affective ToM in the complex emotions one. We took the view that affective ToM abilities are closely related to the recognition of complex mental emotions. Basic emotions are automatically processed, can occur outside a social context and consequently depend on a simple emotion recognition process. By contrast, complex emotions generally involve an actual or imagined social object which could be another individual or a socially constructed self and hence need to be inferred (Hareli and Parkinson, 2008). They therefore require thinking and reasoning processes. Accordingly, we calculated the percentage of correct responses for basic emotions (control condition) and the percentage of correct responses for complex emotions (ToM condition); the correct responses came from a previous study in healthy subjects (Duval et al., 2011). A glossary had been made available to the SD patients so that they would attend to the adjectives’ meaning.
Tom’s taste
This original task, taken from Duval et al. (2011) and distantly inspired by Snowden et al. (2003), assessed the ability to judge the preference of another person in a given context, based on the content of his or her thoughts. The material consisted of 16 cartoon drawings on separate sheets, each showing the centrally positioned face of a character called Tom. This face either smiled or pouted, in order to express Tom’s preference (i.e. affective ToM aspect). Tom’s gaze was directed towards a balloon containing the picture of an object (e.g. biscuits) to illustrate the content of Tom’s thoughts (i.e. cognitive ToM aspect) meaning, for example, that he likes biscuits. In the ToM condition, when the cartoon was shown to the participant, the experimenter orally described a short scenario to put it in context (e.g. “Imagine that you’ve kindly invited Tom to your house for tea or coffee. What would you serve with the tea or coffee?”). The experimenter then showed four possible response pictures, chosen for their degree of relevance: madeleines (CR: correct response, taking both Tom’s preference and the context into account); chocolates (C-P: response taking the context into account but not Tom’s preference); salted crackers (P-C: response taking Tom’s preference into account but not the context); and oysters (UR: unsuitable response taking neither Tom’s preference nor the context into account). Afterwards, participants were asked to justify their choice for each item. Justifications were classified into four types: 1) P: justified according to Tom’s preference, 2) C: justified according to the context, 3) Self: justified according to participant’s own preference in the context, and 4) Other: any other justifications. A total score was calculated for each type. Finally, in a last condition, we presented just the character’s face and thought (i.e. without the four response pictures), and asked the participant what he/she could deduce about the character’s tastes (e.g. “Tom likes biscuits”). In this “control-like condition”, we checked whether the test had been properly understood. In other words, we made sure that the patients’ basic inferences (i.e. symbolic significance of the expressive face and the thought balloon) were accurate. Patients were excluded from the analysis if they failed on more than 50% of the items, a clear sign of their incomprehension. A total success score (%) was calculated for each condition.
2.4.2. Subjective ToM assessment
ToM scale
This instrument consisted of 10 positive or negative sentences divided into two five-item subscales, with items drawn from several questionnaires, including Davis’ (1983) Interpersonal Reactivity Index, and subscales of the Eysenck Personality Questionnaire (Eysenck and Eysenck, 1985). It described various types of relationship one might have with others, eliciting either cognitive (thoughts, attitudes, behaviour) or affective (emotions, feelings) perspective-taking. Thus, the cognitive ToM subscale assessed the ability to understand, infer or interpret the cognitive mental states of others (e.g. ‘I can easily deduce someone’s intentions’), while the affective ToM subscale measured the ability to infer or understand the feelings of others, or to act in response to emotions observed in other people (e.g. ‘I can easily identify the emotions that a person is experiencing’). Participants rated each item on a 4-point Likert-type scale ranging from 1 (‘Does not describe me at all’) to 4 (‘Describes me completely’). A total score (subjective ToM measure) and two subscores (cognitive/affective ToM) were calculated and expressed as percentages, with higher scores associated with greater ToM abilities. To facilitate the use of this scale with the SD patients, its mode of administration was modified: each item was read aloud by the examiner and the patient simply had to point to his/her response on a 4-point scale printed on a separate sheet. Task instructions were repeated and two rewordings of each item were provided, if necessary. However, if a patient nonetheless misunderstood one or two items, his/her score was calculated from the number of remaining items; if he/she misunderstood three items or more, he/she was excluded from the analysis of this task.
3. Results
Given the sample size of the patient group, nonparametric analyses were used to measure internal consistency. The Mann-Whitney U-test was conducted to gauge intergroup differences and Wilcoxon pairwise comparisons to assess the effect of the experimental condition compared with the control one. For the purposes of these analyses, a unilateral statistical level of significance was set at .05. Statistical analyses were conducted with all the patients. However, when a patient totally failed to perform the task due to a profound comprehension deficit, he/she was excluded from the analysis for that particular task. These instances are indicated in Table 3, which shows the performances of the SD patients and healthy controls on all the ToM tasks in each condition (ToM vs. control). Finally, in order to better understand SD patients’ ToM performance, we also performed Spearman correlations between their neuropsychological scores and the ToM scores.
Table 3.
Comparison between SD patients and healthy controls on ToM abilities
| ToM Tests and measures (%) | SD patients | Healthy controls | z | p |
|---|---|---|---|---|
| Objective assessment | ||||
|
| ||||
| Cognitive ToM | ||||
| Attribution of intention task1 | ||||
| ToM condition | 72.86 (±23.35) | 93.38 (±9.36) | 3.63 | <.001 |
| Character control condition | 88.49 (±17.03) | 94.49 (±8.90) | 0.95 | ns |
| Object control condition | 94.29 (±16.51) | 97.31 (±5.74) | −0.40 | ns |
| False beliefs (total ToM score) | 66.66 (±18.86) | 85.73 (±13.44) | 3.51 | <.001 |
| 1st-order ToM condition | 73.33 (±21.06) | 90.58 (±12. 26) | 3.16 | .002 |
| 2nd-order ToM condition | 58.69 (±19.73) | 80.56 (±20.82) | 3.16 | .002 |
| Control condition | 96.44 (±8.31) | 95.03 (±6.98) | −1.36 | ns |
| Affective ToM | ||||
| Face/eyes test | ||||
| basic emotions | 55.33 (±14.07) | 71.94 (±14.11) | 3.52 | <.001 |
| complex emotions | 44.15 (±18.24) | 55 (±17.48) | 1.99 | .05 |
| Composite ToM 2 | ||||
| Tom’s taste | ||||
| Experimental condition | 63.64 (±13.81) | 87.50 (±14.56) | 3.81 | <.001 |
| Control-like condition | 65 (±14.49) | 97.06 (±11.01) | 4.25 | <.001 |
| Subjective assessment | ||||
|
| ||||
| ToM scale (total score) 3 | 39.70 (±10.59) | 57.50 (±12.81) | 3.17 | .002 |
| Cognitive ToM subscale | 38.43 (±18.89) | 52.41 (±20.67) | 1.65 | ns |
| Affective ToM subscale | 46.39 (±12.26) | 62.59 (±12.48) | 3.45 | <.001 |
Note.
Analyses were conducted on 14 SD patients;
Analyses were conducted on 10 SD patients;
Analyses were conducted on 12 SD patients. Otherwise, analyses were conducted on 15 SD patients.
Significant comparisons after false discovery rate corrections are in bold.
3.1. Objective ToM assessment
3.1.1. Attribution of intention task
Intergroup comparisons
In the experimental ToM condition, Mann-Whitney comparisons revealed a significant effect of group (U = 92, z = 3.63, p < .001), indicating that the SD group performed more poorly than the controls. However, SD patients did not significantly differ from the healthy controls on the two control conditions.
Intragroup comparisons
In the patient group, Wilcoxon pairwise comparisons revealed a significant difference between the ToM and both control conditions: performances in the control conditions with characters/objects were better than performances in the ToM condition (z = 2.86/3.06, p < .005 for both). No difference was found between the two control conditions. In the control group, analyses revealed a significant difference between the ToM condition and the control condition with objects, with a better performance in the control condition (z = 2.02, p < .05).
3.1.2. False-belief task
Intergroup comparisons
In the experimental ToM condition, Mann-Whitney comparisons revealed a significant effect of group in the first-order condition (U = 124, z = 3.16, p < .005) as well as in the second-order one (U = 120.5, z = 3.16, p < .005), with SD patients performing more poorly than controls. No significant intergroup difference was found in the control condition.
Intragroup comparisons
Analyses showed a significant effect of the ToM condition in both the SD (z = 3.30, p = .001) and healthy control (z = 3.75, p < .001) groups: performances in the total (first- and second-order) ToM condition were poorer than in the control one (Table 3). Moreover, a significant difference was found according to the level of representations, with poorer performances on second-order false beliefs than on first-order ones for both SD patients (z = 2.67, p = .01) and healthy controls (z = 2.91, p < .005).
3.1.3. The Eyes test
Intergroup comparisons
A significant effect of group was found in both the basic emotions (U = 103.5, z = 3.52, p < .001) and the complex emotions conditions (U = 175, z = 1.99, p = .05), in that SD patients performed more poorly than the healthy controls.
Intragroup comparisons
Analyses showed a significant effect of condition in both the SD (z = 2.17, p = .05) and healthy control (z = 3.65, p < .001) groups, in that they performed better in the basic emotions condition than in the complex emotions one.
3.1.4. Tom’s taste
Intergroup comparisons
An effect of group was found in both the ToM (U = 39, z = 3.81, p < .001) and the control-like (U = 54,5, z = 4.26, p < .001) conditions, in that SD patients performed more poorly than the healthy controls (Table 3).
Intragroup comparisons
Analyses showed a significant effect of condition for both the healthy controls (T = 17, z = 3.42, p < .001) and SD patients (T = 1.5, z = 2.65, p < .01), in that they performed better in the control condition than in the ToM one.
Analysis of choices of responses
In order to understand the SD patients’ deficit in this complex ToM task, Mann-Whitney comparisons were conducted for each category of responses. Results (Figure 3A) showed that SD patients gave more C-P responses (i.e. taking the context but not Tom’s preference into account; U = 49, z = −3.62, p < .001) and unsuitable responses (U = 105, z =−2.53, p < .05) than the controls when they provided incorrect responses.
Fig 3.
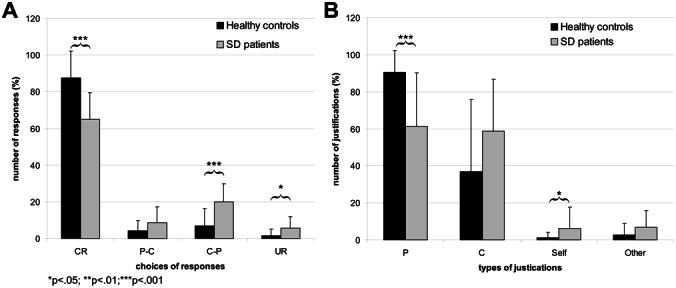
Fig 3A. Choices of responses on the Tom’s taste.
CR: correct response; C-P: response taking the context into account but not Tom’s preference; PC: response taking Tom’s preference into account but not the context; UR: unsuitable response
Fig 3B. Justifications of responses on the Tom’s taste.
P: justified according to Tom’s preference; C: justified according to the context; Self: justified according to participant’s own preference in the context; Other: any other justifications.
Analysis of types of justifications
Mann-Whitney comparisons were conducted on each type of justification. Results (Figure 3B) indicated that SD patients justified their responses significantly less on the basis of Tom’s preference (U = 46.5, z = 3.64, p < .001) and more on their self-views (U = 119, z = −2.19, p = .05) than the control group.
3.2. Subjective ToM assessment
Intergroup comparisons
Mann-Whitney comparisons revealed an effect of group on the affective ToM subscale (U = 72.5, z = 3.45, p < .001): SD patients estimated their affective ToM abilities more negatively than the healthy controls. No difference was found in the cognitive ToM subscale (U = 147, z = 1.65, ns).
Intragroup comparisons
Analyses showed a significant difference between the two subscales for the healthy control group (T = 122, z = 2.47, p = .01), in that they judged their affective ToM abilities more favourably than their cognitive ones. Even though SD patients scored less well on the cognitive ToM subscale, the difference was not significant.
To go one step further, we conducted a supplementary analysis by computing two new scores illustrating ToM insight in SD patients. First, we calculated two objective ToM z-scores: 1) a cognitive ToM z-score combining performances on the attribution of intention (ToM condition) and false-belief tasks (Total score in the ToM condition); 2) an affective ToM z-score for the complex emotions condition of the Eyes test. Second, we calculated subjective cognitive and affective ToM z-scores for the cognitive and affective ToM subscales, respectively. Finally, we calculated the difference between the objective and subjective scores using the following formula: 1) Objective cognitive z-score minus subjective cognitive z-score for the cognitive ToM insight measure; 2) Objective affective z-score minus subjective affective z-score for the affective ToM insight measure. Each score was then compared with the normal standard (i.e. 0) (Table 4). The closer to zero the score was, the greater the cognitive (or affective) ToM insight. Results showed that SD patients significantly differed from the reference value only for cognitive ToM insight, indicating that they were unaware of their cognitive ToM disabilities, but not their affective ones. Thus, this analysis confirmed the dissociation observed in the ToM scale.
Table 4.
Comparison between SD patients ToM insight and normal standard
| Z-score mean | Reference value | t | p | |
|---|---|---|---|---|
| Cognitive ToM insight measure | −0.96 | 0.00 | −2.28 | .04 |
| Affective ToM insight measure | 0.77 | 0.00 | 1.76 | ns |
Overall, SD patients performed poorly on several objective tasks probing cognitive and affective ToM. They also gave lower ratings than the healthy controls on the sole subjective affective ToM scale.
In order to obtain more stringent results, we used the Benjamini-Hochberg (1995) procedure for controlling the false discovery rate. Results were similar, except for the complex emotions condition of the Eyes test and the ‘Self’ and ‘Other’ justification conditions of Tom’s taste, which became nonsignificant (Table 3).
3.3. Relationhips between ToM and neuropsychological impairments
Regarding the objective ToM assessment, Spearman correlations between the experimental conditions of the ToM tasks and the SD patients’ neuropsychological scores revealed significant positive correlations between the Concept subscale of the Mattis scale and the second-order condition of the false-belief task (r = 0.52, p < .05), and between the Rey-Osterrieth complex figure recall score and the ToM attribution of intention condition (r = 0.73, p < .01). Regarding the subjective ToM assessment, a significant positive correlation was found between the cognitive ToM subscale and literal fluency (r = .69, p < .05). After false discovery rate control, the correlations between ToM and neuropsychological tasks became nonsignificant.
4. Discussion
The aim of the present study was to explore cognitive and affective ToM, which are suspected of being impaired in SD. By administering a thorough ToM examination, we were able to demonstrate a deficit in all the ToM components assessed via objective ToM tasks, and a loss of insight of their cognitive ToM impairment.
As regards cognitive ToM, SD patients failed to infer either the intentions or the false beliefs of a character involved in a social scenario. This deficit could not be explained by a visual semantic disorder or a comprehension deficit, as they achieved normal scores in the two control conditions. In the test of attribution of intention, for instance, SD patients were particularly poor at predicting a character’s action, though not the future of characters without intention or of physical objects. This result could be explained by the major temporal lobe abnormalities which characterize those patients, especially in the left temporal pole. Using a similar ToM task in a functional magnetic resonance imaging study with healthy participants, Völlm et al. (2006) found that the temporal poles, with a left-sided preponderance, were activated in the ToM condition but not in the two control conditions (i.e. physical causality relative to a character without intention or a simple object). Likewise, Walter et al. (2004) reported similar results with an equivalent task of deducing other people’s intentions.
We also showed a link between visual episodic memory and the ToM condition of this task. The relationship between episodic memory and mentalizing has already been flagged up in developmental studies (Perner, 2000), and neuroimaging studies have shown that the two processes are mediated by similar brain networks, including the hippocampus (Perry et al., 2011; Rabin et al., 2010; Spreng and Grady, 2010). According to Perry and colleagues (2011), mentalizing may be based on self-projection, where the individual recalls experiencing a similar event. Thus, SD patients may have attempted to rely on their memories of social experiences in order to comprehend the protagonists ‘intentions’. While not compensating for their ToM deficit, episodic memory abilities did account for a proportion of the variability in their ToM performances in the attribution of intention test.
As far as the false-belief task is concerned, we showed that SD patients had difficulties inferring the characters’ beliefs, especially when they had to take two perspectives simultaneously into account. According to Samson et al. (2005), two components of ToM are typically involved in classic false-belief tasks: inhibition of one’s own perspective and inference of another person’s mental state. In our task, participants could only choose between two responses: one referring to the character’s mental state, the other to the reality of the scenario. It is, therefore, entirely possible that the patients’ erroneous responses reflected a deficit in the inhibition of their own perspective, given that they obviously understood the scenario properly. However, it is more likely that SD patients presented a specific disturbance in the inference of mental states. For a start, their performance declined according to the degree of inference, such that second-order ToM was more impaired than first-order ToM. Second, no relationship was found between the false-belief task and the SD patients’ inhibition performance. The significant correlation between the Concept subscale of the Mattis scale and second-order false belief ToM suggests that the patients’ semantic impairment may have interfered with and/or impoverished their complex reasoning.
Most studies using false-belief tasks in healthy adults have underlined the involvement of the temporal regions, as well as the median prefrontal cortex and, more especially, the anterior cingulate cortex (Gallagher et al., 2000; Vogeley et al., 2001; Ferstl and Von Cramon, 2002). Moreover, bv-FTD patients with bilateral atrophy in the orbitomedial region and anterior temporal lobe have been shown to perform poorly on first- and second-order tests (Lough et al., 2001; Adenzato et al., 2010). The SD patients in the current study presented broad left-sided temporal atrophy, together with hypometabolism in similar areas, but also in the median orbitofrontal and anterior cingulate regions, which may explain their cognitive ToM decline.
Overall, performances were better in the control condition than in the ToM condition for both groups, raising the question of differences in task difficulty. To address this issue, two points need to be considered. First, ageing is known to affect ToM, such that healthy older people perform more poorly than younger ones on both attribution of intention and false-belief tests (Duval et al., 2011). This normal ageing effect on ToM abilities may therefore explain why the control group performed better in the control condition than in the ToM one. Second, in the attribution of intention test, we used exactly the same format of stories and subsequent questions in all three conditions. Thus, the differences between them must have stemmed from the nature of the representations being manipulated. Consequently, task difficulty would seem to be an inadequate explanation for the impairment of cognitive ToM observed in SD patients. Dysfunction of ToM processes (inference and manipulation of intention and epistemic representations) is more likely to account for their impaired performances.
As regards the affective ToM test, we found that SD patients performed significantly more poorly than healthy controls on both basic and complex emotions recognition. Regarding the basic emotion condition, our results are consistent with numerous previous studies showing an emotional recognition processing disorder in SD via facial expression tests (Rosen et al., 2002; 2004; Calabria et al., 2009). Moreover, authors have found that negative emotion recognition is particularly badly affected. Our results may have been influenced by an emotional valence bias, since only 30% of items illustrated positive emotions (e.g. happiness, surprise), compared with 70%, negative ones (e.g. sadness, fear, anger). Post hoc analyses revealed significant differences in the recognition of basic emotions according to valence in both groups (data not shown): in the SD patients, positive and negative emotions were recognized in 80% and 45.90% of cases respectively, whereas these figures were 81.33% and 66.86% for the healthy controls. Consistent with the literature (Rosen et al., 2002; 2004), the only significant intergroup difference concerned negative emotions. This deficit of SD patients could be explained by brain abnormalities other than their anterior temporal ones. Numerous studies in healthy and neurological populations have pointed to the crucial involvement of the amygdala, insula, fusiform gyrus or superior temporal gyrus in the recognition of emotion, including negative emotion (Anderson et al., 2000; Rosen et al., 2002; Omar et al., in press; for a review, see Adolphs, 2002). The considerable atrophy and hypometabolism of these brain regions in our SD patients may thus have impaired their basic negative emotion processing.
Concerning complex emotions, we also found significant differences between our SD patients and controls, and these differences might have been even greater had it not been for the floor-level scores obtained by the control group for several emotions (data not shown). This result is not surprising, given that previous studies have reported the involvement of the temporal poles in complex emotion processing in the healthy population (Burnett and Blackmore, 2009). Although numerous studies support the notion that complex (or social) emotion processing is sustained by a more extensive brain network than that of basic emotions, temporal regions represent key processing sites (Britton et al., 2006; Castelli et al., 2010; Takahasi et al., 2008). Researchers have also demonstrated that complex emotions are processed in the amygdala (Adolphs et al., 2002). In the latter study, authors found that patients with unilateral or bilateral amygdala damage failed to recognize social emotions in the Eyes test. Hence, the atrophy and hypometabolism in the temporal pole and amygdala in our SD patient group may explain their failure to infer complex emotions.
Likewise, in the composite ToM task, the SD patient group performed poorly in both the experimental and control conditions. Given that the control condition checked the inferences they made from the characters’ pictures alone (i.e. without any context or response pictures), their failure in the experimental condition must therefore have been related to their inability to deduce the character’s preference. The detailed analyses of responses in the ToM condition confirmed their tendency to choose more context-related responses (i.e. without taking the character’s preference into account) than the controls did. Interestingly, the SD patients were more likely than the controls to justify their choices on the basis of their own preferences or other unexpected criteria. This fits in with previous behavioural studies in SD patients reporting their self-centredness and egocentric world view (Snowden et al., 2001). SD patients often present abnormal egocentric behaviour, referred to as “behavioural egocentrism” by Belliard et al. (2007). Whereas its origin is still unknown, this disorder seems to be specific to SD (compared with bv-FTD) and could be partially related to ToM impairment (Bon et al., 2009). A future study could be conducted to understand this pattern of results by exploring relations between ToM’s taste scores and behavioural egocentrism measures. In any event, our participants’ performance on the composite ToM task clearly indicates that SD patients have difficulty understanding other people’s cognitive and affective mental states when these are embedded. Considering the contextual responses and personal justifications made by SD patients in the test, we suggest that they mainly rely on contextual knowledge and their own personal interests when dealing with social interactions. Because our test was designed to explore ToM under conditions that corresponded to the daily social context, it inherently encompassed both affective and cognitive ToM, thus preventing us from distinguishing between the two. We therefore cannot conclude whether the deficit we observed resulted from a cognitive impairment (inferring thought), affective impairment (inferring preference) or both. Future research is needed to unravel this issue.
Finally, our subjective cognitive and affective ToM subscale findings suggest that the SD patients were aware of their affective ToM disturbance but not of their difficulty in inferring and understanding the intentions and beliefs of others. In addition, despite massive semantic memory disturbance and episodic memory failures, SD patients did not complain more than controls about their daily memory functioning, as attested by their responses to the Cognitive Difficulties Scale. Taken together, these results suggest an impairment of cognitive functioning awareness in our SD patients. Anosognosia has been widely reported in frontotemporal lobar degeneration (Eslinger et al., 2005; O’Keeffee et al., 2007): patients tend to underestimate the extent of their cognitive and behavioural changes, even if metacognition deficits are more severe in bv-FTD than in SD patients and affect a broader range of cognitive domains (Eslinger et al., 2005; Zamboni et al., 2010). Anosognosia for behavioural disability has been associated with right temporal atrophy in patients with FTD or corticobasal syndrome (Zamboni et al., 2010) and with left temporal pole hypometabolism in patients with bv-FTD (Ruby et al., 2007). The atrophy and hypometabolism of these structures in our own SD patients may have contributed to their lack of awareness of cognitive ToM deficits. We observed a significant correlation between the cognitive ToM subscale and literal fluency performance in the SD patients. Because the literal fluency task involved strategic processes, it is tempting to conclude that this result reflects the involvement of executive functions in making such self-assessments. However, in SD, literal fluency performance is determined mainly by semantic memory capacity and left temporal cortex metabolism (Laisney et al., 2009). Accordingly, in SD, fluency performances can be regarded as an index of disease severity and we can assume that patients become increasingly unaware of their cognitive ToM difficulties as the disease progresses.
The SD patients’ awareness of their affective ToM disturbance is more surprising. In a previous study, Eslinger et al. (2005) found that SD patients overestimated their affective ToM ability on a cognitive empathic subscale. These discrepant results may stem from the way in which metacognition was assessed, for while Eslinger and colleagues (2005) compared reports of patients and their relatives, we compared the SD patients’ subjective assessments with those of the healthy controls. Thus, our study revealed a dichotomy between cognitive and affective ToM insight in SD patients. Given the impact of ToM deficits, especially affective ToM deficits, on family and social interactions, the patients’ relatives may well have attempted to force the patients to consider their affective difficulties, thus facilitating their awareness. Other studies need to be conducted in order to understand this pattern of results more fully.
Overall, this study provides evidence of an objective impact of SD on cognitive and affective ToM. While the patients’ semantic impairment may have contributed to their poor ToM performances, it is unlikely to provide the full explanation. The patients in our study were still in the mild stage of the disease and we used procedures designed to minimize the confounding effect of the patients’ semantic impairment on their ToM performance. It is interesting to note that the correlation analysis between the semantic memory scores and the ToM performances revealed only one significant correlation (between the Concept subscale of the Mattis scale and the second-order condition of the false-belief task). The SD patients’ inference ability was impaired for intentions, beliefs and affective states. The cognitive ToM deficits in SD patients would appear to be associated with the cerebral atrophy in the left temporal lobe and hypometabolism in the temporal lobes and medial frontal cortex. Impairment of the affective ToM would seem to be the result of abnormalities in the temporal regions and amygdala. Finally, the subjective assessment of ToM suggests a dichotomy between cognitive and affective aspects with anosognosia only for cognitive ToM disabilities in the early to moderate stages of the disease. SD patients hence differ from bv-FTD patients, who present deficits on all objective ToM tasks (Gregory et al., 2002) and severe anosognosia. SD patients were shown here to display deficits in intersubjectivity due to a cognitive and affective ToM impairment. We therefore suggest that it is this difficulty in attributing mental states to others that leads SD patients to become focused on themselves, which would explain their self-centred responses to the composite ToM task and/or their general behavioural egocentrism described in literature. In turn, behavioural egocentrism may also influence ToM abilities and interpersonal relationships. However, our results must be viewed with caution, given the heterogeneous patterns of ToM deficits displayed by the patients, as well as the use of a unique task of affective ToM. They now need to be confirmed and reinforced in further experiments exploring the link with their behavioural egocentrism in greater detail.
Acknowledgments
We wish to thank Alice Pélerin (Caen University Hospital) and Catherine Merck (Rennes University Hospital) for their help in recruiting the patients, Florence Mezenge (Cyceron center, Caen) for her contribution to the brain data analyses, and Elizabeth Wiles-Portier for reviewing the English style.
Abbreviations
- SD
semantic dementia
- ToM
theory of mind
- bv-FTD
behavioural variant of frontotemporal dementia
References
- Abu-Akel A. A neurobiological mapping of theory of mind. Brain Res Rev. 2003;43:29–40. doi: 10.1016/s0165-0173(03)00190-5. [DOI] [PubMed] [Google Scholar]
- Adenzato M, Cavallo M, Enrici I. Theory of mind ability in the behavioural variant of frontotemporal dementia: an analysis of the neural, cognitive, and social levels. Neuropsychologia. 2010;48:2–12. doi: 10.1016/j.neuropsychologia.2009.08.001. [DOI] [PubMed] [Google Scholar]
- Adolphs R. Recognizing emotion from facial expressions: psychological and neurological mechanisms. Behav Cogn Neurosci Rev. 2002;1:21–62. doi: 10.1177/1534582302001001003. [DOI] [PubMed] [Google Scholar]
- Adolphs R, Baron-Cohen S, Tranel D. Impaired recognition of social emotions following amygdala damage. J Cogn Neurosci. 2002;14:1264–1274. doi: 10.1162/089892902760807258. [DOI] [PubMed] [Google Scholar]
- Anderson AK, Spencer DD, Fulbright RK, Phelps EA. Contribution of the anteromedial temporal lobes to the evaluation of facial emotion. Neuropsychology. 2000;14:526–536. doi: 10.1037//0894-4105.14.4.526. [DOI] [PubMed] [Google Scholar]
- Baron-Cohen S, Goodhart F. The “seeing leads to knowing” deficit in autism: the Pratt and Bryant probe. Brit J Dev Psychol. 1994;12:397–402. [Google Scholar]
- Baron-Cohen S, O’Riordan M, Stone V, Jones R, Plaisted K. Recognition of faux pas by normally developing children and children with Asperger syndrome or high-functioning autism. J Autism Dev Disord. 1999;29:407–418. doi: 10.1023/a:1023035012436. [DOI] [PubMed] [Google Scholar]
- Baron-Cohen S, Wheelwright S, Jolliffe T. Is there a “language of the eyes”? Evidence from normal adults, and adults with autism or Asperger syndrome. Vis Cogn. 1997;4:311. [Google Scholar]
- Baron-Cohen S, Wheelwright S, Hill J, Raste Y, Plumb I. The “Reading the Mind in the Eyes” Test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J Child Psychol Psychiatry. 2001;42:241–251. [PubMed] [Google Scholar]
- Beer JS, Ochsner KN. Social cognition: a multi level analysis. Brain Res. 2006;1079:98–105. doi: 10.1016/j.brainres.2006.01.002. [DOI] [PubMed] [Google Scholar]
- Belliard S, Bon L, LeMoal S, Jonin PY, Vercelletto M, LeBail B. Semantic dementia. Psychol Neuropsychiatr Vieil. 2007;5:127–138. [PubMed] [Google Scholar]
- Belliard S, Moreaud O. GRESEM. Batterie d’évaluation des connaissances sémantiques (BECS-GRECO) In: Hugonot-Diener L, Barbeau E, Michel BF, Thomas-Antérion C, Robert P, editors. GREMOIRE : tests et échelles de la maladie d’Alzheimer et des syndromes apparentés. Marseille; Solal: 2008. pp. 83–85. [Google Scholar]
- Benjamini Y, Hochberg Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J Roy Statistical Society. 1995;57:289–30. [Google Scholar]
- Bon L, Belliard S, Eustache F, Desgranges B. L’égocentrisme comportemental dans la démence sémantique: conséquence d’un trouble de la théorie de l’esprit et/ou de l’égocentrisme cognitif? Rev Neuropsychol. 2009;1:133–149. [Google Scholar]
- Britton JC, Phan KL, Taylor SF, Welsh RC, Berridge KC, Liberzon I. Neural correlates of social and nonsocial emotions: an fMRI study. Neuroimage. 2006;31:397–409. doi: 10.1016/j.neuroimage.2005.11.027. [DOI] [PubMed] [Google Scholar]
- Brothers L, Ring B. A neuroethological framework for the representation of minds. J Cogn Neurosci. 1992;4:107–118. doi: 10.1162/jocn.1992.4.2.107. [DOI] [PubMed] [Google Scholar]
- Brunet E, Sarfati Y, Hardy-Baylé MC, Decety J. A PET investigation of the attribution of intentions with a nonverbal task. Neuroimage. 2000;11:157–166. doi: 10.1006/nimg.1999.0525. [DOI] [PubMed] [Google Scholar]
- Burnett S, Blakemore S. Functional connectivity during a social emotion task in adolescents and in adults. Eur J Neurosci. 2009;29:1294–1301. doi: 10.1111/j.1460-9568.2009.06674.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calabria M, Cotelli M, Adenzato M, Zanetti O, Miniussi C. Empathy and emotion recognition in semantic dementia: a case report. Brain Cogn. 2009;70:247–252. doi: 10.1016/j.bandc.2009.02.009. [DOI] [PubMed] [Google Scholar]
- Cardebat D, Doyon B, Puel M, Goulet P, Joanette Y. Evocation lexicale formelle et sémantique chez des sujets normaux. Performances et dynamiques de production en fonction du sexe, de l’âge et du niveau d’étude. Acta Neurol Belg. 1990;90:207–217. [PubMed] [Google Scholar]
- Carrington SJ, Bailey AJ. Are there theory of mind regions in the brain? A review of the neuroimaging literature. Hum Brain Mapp. 2009;30:2313–2335. doi: 10.1002/hbm.20671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castelli I, Baglio F, Blasi V, Alberoni M, Falini A, Liverta-Sempio O, et al. Effects of aging on mindreading ability through the eyes: an fMRI study. Neuropsychologia. 2010;48:2586–2594. doi: 10.1016/j.neuropsychologia.2010.05.005. [DOI] [PubMed] [Google Scholar]
- Chan D, Fox NC, Scahill RI, Crum WR, Whitwell JL, Leschziner G, Rossor AM, Stevens JM, Cipolotti L, Rossor MN. Patterns of temporal lobe atrophy in semantic dementia and Alzheimer’s disease. Ann Neurol. 2001;49:433–442. [PubMed] [Google Scholar]
- Coricelli G. Two-levels of mental states attribution: from automaticity to voluntariness. Neuropsychologia. 2005;43:294–300. doi: 10.1016/j.neuropsychologia.2004.11.015. [DOI] [PubMed] [Google Scholar]
- Davis M. A multidimensional approach to individual differences in empathy. JSAS Catalog of Selected Documents in Psychology. 1980:10. [Google Scholar]
- Davis MH. Measuring individual differences in empathy: evidence for a multidimensional approach. J Pers Soc Psychol. 1983;44:113–126. [Google Scholar]
- Decety J, Lamm C. Human empathy through the lens of social neuroscience. Scientific World Journal. 2006;6:1146–1163. doi: 10.1100/tsw.2006.221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deloche G, Hannequin D. Test de dénomination oral d’images DO80. Paris: Les Editions du Centre de Psychologie Appliquée; 1997. [Google Scholar]
- Desgranges B, Matuszewski V, Piolino P, Chételat G, Mézenge F, Landeau B, et al. Anatomical and functional alterations in semantic dementia: a voxel-based MRI and PET study. Neurobiol Aging. 2007;28:1904–1913. doi: 10.1016/j.neurobiolaging.2006.08.006. [DOI] [PubMed] [Google Scholar]
- Duval C, Piolino P, Bejanin A, Eustache F, Desgranges B. Age effects on different components of theory of mind. Conscious Cogn. 2011;20:627–642. doi: 10.1016/j.concog.2010.10.025. [DOI] [PubMed] [Google Scholar]
- Edwards-Lee T, Miller BL, Benson DF, Cummings JL, Russell GL, Boone K, et al. The temporal variant of frontotemporal dementia. Brain. 1997;120 (Pt 6):1027–1040. doi: 10.1093/brain/120.6.1027. [DOI] [PubMed] [Google Scholar]
- Eslinger PJ. Neurological and neuropsychological bases of empathy. Eur Neurol. 1998;39:193–199. doi: 10.1159/000007933. [DOI] [PubMed] [Google Scholar]
- Eslinger PJ, Dennis K, Moore P, Antani S, Hauck R, Grossman M. Metacognitive deficits in frontotemporal dementia. J Neurol Neurosur Ps. 2005;76:1630–1635. doi: 10.1136/jnnp.2004.053157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eslinger PJ, Moore P, Troiani V, Antani S, Cross K, Kwok S, et al. Oops! Resolving social dilemmas in frontotemporal dementia. J Neurol Neurosurg Ps. 2007;78:457–460. doi: 10.1136/jnnp.2006.098228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eysenck HJ, Eysenck MW. Personality and individual differences: a natural science approach. New York: Plenum Press; 1985. [Google Scholar]
- Ferstl EC, von Cramon DY. What does the frontomedian cortex contribute to language processing: coherence or theory of mind? Neuroimage. 2002;17:1599–1612. doi: 10.1006/nimg.2002.1247. [DOI] [PubMed] [Google Scholar]
- Fletcher PC, Happé F, Frith U, Baker SC, Dolan RJ, Frackowiak RS, et al. Other minds in the brain: a functional imaging study of “theory of mind” in story comprehension. Cognition. 1995;57:109–128. doi: 10.1016/0010-0277(95)00692-r. [DOI] [PubMed] [Google Scholar]
- Frith CD, Frith U. Interacting minds--a biological basis. Science. 1999;286:1692–1695. doi: 10.1126/science.286.5445.1692. [DOI] [PubMed] [Google Scholar]
- Frith U, Frith CD. Development and neurophysiology of mentalizing. Philos T Roy Soc B. 2003;358:459–473. doi: 10.1098/rstb.2002.1218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gallagher HL, Happé F, Brunswick N, Fletcher PC, Frith U, Frith CD. Reading the mind in cartoons and stories: an fMRI study of “theory of mind” in verbal and nonverbal tasks. Neuropsychologia. 2000;38:11–21. doi: 10.1016/s0028-3932(99)00053-6. [DOI] [PubMed] [Google Scholar]
- Gallagher HL, Jack AI, Roepstorff A, Frith CD. Imaging the intentional stance in a competitive game. Neuroimage. 2002;16:814–821. doi: 10.1006/nimg.2002.1117. [DOI] [PubMed] [Google Scholar]
- Gobbini MI, Koralek AC, Bryan RE, Montgomery KJ, Haxby JV. Two takes on the social brain: a comparison of theory of mind tasks. J Cogn Neurosci. 2007;19:1803–1814. doi: 10.1162/jocn.2007.19.11.1803. [DOI] [PubMed] [Google Scholar]
- Goel V, Grafman J, Sadato N, Hallett M. Modeling other minds. Neuroreport. 1995;6:1741–1746. doi: 10.1097/00001756-199509000-00009. [DOI] [PubMed] [Google Scholar]
- Good CD, Scahill RI, Fox NC, Ashburner J, Friston KJ, Chan D, Crum WR, Rossor MN, Frackowiak RS. Automatic differentiation of anatomical patterns in the human brain: validation with studies of degenerative dementias. Neuroimage. 2002;17:29–46. doi: 10.1006/nimg.2002.1202. [DOI] [PubMed] [Google Scholar]
- Gorno-Tempini ML, Dronkers NF, Rankin KP, Ogar JM, Phengrasamy L, Rosen HJ, Johnson JK, Weiner MW, Miller BL. Cognition and anatomy in three variants of primary progressive aphasia. Ann Neurol. 2004;55:335–346. doi: 10.1002/ana.10825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gregory C, Lough S, Stone V, Erzinclioglu S, Martin L, Baron-Cohen S, et al. Theory of mind in patients with frontal variant frontotemporal dementia and Alzheimer’s disease: theoretical and practical implications. Brain. 2002;125:752–764. doi: 10.1093/brain/awf079. [DOI] [PubMed] [Google Scholar]
- Happaney K, Zelazo PD, Stuss DT. Development of orbitofrontal function: current themes and future directions. Brain Cogn. 2004;55:1–10. doi: 10.1016/j.bandc.2004.01.001. [DOI] [PubMed] [Google Scholar]
- Hareli S, Parkinson B. What’s social about social emotions? J Theor Soc Behav. 2008;38:131–156. [Google Scholar]
- Hodges JR, Patterson K. Semantic dementia: a unique clinicopathological syndrome. Lancet Neurol. 2007;6:1004–1014. doi: 10.1016/S1474-4422(07)70266-1. [DOI] [PubMed] [Google Scholar]
- Izard CE. Innate and universal facial expressions: evidence from developmental and cross-cultural research. Psychol Bull. 1994;115:288–299. doi: 10.1037/0033-2909.115.2.288. [DOI] [PubMed] [Google Scholar]
- Kipps CM, Hodges JR. Theory of mind in frontotemporal dementia. Soc Neurosci. 2006;1:235–244. doi: 10.1080/17470910600989847. [DOI] [PubMed] [Google Scholar]
- Laisney M, Matuszewski V, Mézenge F, Belliard S, de La Sayette V, Eustache F, Desgranges B. The underlying mechanisms of verbal fluency in frontotemporal dementia and semantic dementia. J Neurol. 2009;256:1083–1094. doi: 10.1007/s00415-009-5073-y. [DOI] [PubMed] [Google Scholar]
- Lezak MD. Neuropsychological assessment. New York: Oxford University Press; 1995. [Google Scholar]
- Lough S, Gregory C, Hodges JR. Dissociation of social cognition and executive function in frontal variant frontotemporal dementia. Neurocase. 2001;7:123–130. doi: 10.1093/neucas/7.2.123. [DOI] [PubMed] [Google Scholar]
- Lough S, Kipps CM, Treise C, Watson P, Blair JR, Hodges JR. Social reasoning, emotion and empathy in frontotemporal dementia. Neuropsychologia. 2006;44:950–958. doi: 10.1016/j.neuropsychologia.2005.08.009. [DOI] [PubMed] [Google Scholar]
- Mattis S. Mental status examination for organic mental syndrome in the elderly patient. In: Bellack L, Karasu TB, editors. Geriatric psychiatry: a handbook for psychiatrists and primary care physicians. New York: Grune and Stratton; 1976. pp. 77–121. [Google Scholar]
- McNair DM, Kahn RJ. Self-assessment of cognitive deficits. In: Crook T, editor. Assessment in geriatric psychopharmacology. New Canaan, CT: Mark Powler Associates; 1983. pp. 137–143. [Google Scholar]
- Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn Psychol. 2000;41:49–100. doi: 10.1006/cogp.1999.0734. [DOI] [PubMed] [Google Scholar]
- Morin A. Levels of consciousness and self-awareness: a comparison and integration of various neurocognitive views. Conscious Cogn. 2006;15:358–371. doi: 10.1016/j.concog.2005.09.006. [DOI] [PubMed] [Google Scholar]
- Morin A. Self-recognition, theory-of-mind, and self-awareness: what side are you on? Laterality. 2010:1–17. doi: 10.1080/13576501003702648. [DOI] [PubMed] [Google Scholar]
- Neary D, Snowden JS, Gustafson L, Passant U, Stuss D, Black S, et al. Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology. 1998;51:1546–1554. doi: 10.1212/wnl.51.6.1546. [DOI] [PubMed] [Google Scholar]
- Nestor PJ, Fryer TD, Hodges JR. Declarative memory impairments in Alzheimer’s disease and semantic dementia. Neuroimage. 2006;30:1010–1020. doi: 10.1016/j.neuroimage.2005.10.008. [DOI] [PubMed] [Google Scholar]
- O’Keeffe FM, Murray B, Coen RF, Dockree PM, Bellgrove MA, et al. Loss of insight in frontotemporal dementia, corticobasal degeneration and progressive supranuclear palsy. Brain. 2007;130:753–764. doi: 10.1093/brain/awl367. [DOI] [PubMed] [Google Scholar]
- Olson IR, Plotzker A, Ezzyat Y. The enigmatic temporal pole: a review of findings on social and emotional processing. Brain. 2007;130:1718–1731. doi: 10.1093/brain/awm052. [DOI] [PubMed] [Google Scholar]
- Omar R, Rohrer JD, Hailstone JC, Warren JD. Structural neuroanatomy of face processing in frontotemporal lobar degeneration. J Neurol Neurosurg Ps. doi: 10.1136/jnnp.2010.227983. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pacherie E. L’émpathie et ses degres. In: Berthoz A, Jorland G, editors. L’empathie. Paris: Odile Jacob; 2004. pp. 149–181. [Google Scholar]
- Perner J. Memory and theory of mind. In: Tulving EFIM, Craik FIM, editors. The Oxford handbook of memory. New York: Oxford University Press; 2000. pp. 297–312. [Google Scholar]
- Perry D, Hendler T, Shamay-Tsoory SG. Projecting memories: The role of the hippocampus in emotional mentalizing. NeuroImage. 2011;54:1669–1676. doi: 10.1016/j.neuroimage.2010.08.057. [DOI] [PubMed] [Google Scholar]
- Perry RJ, Rosen HR, Kramer JH, Beer JS, Levenson RL, Miller BL. Hemispheric dominance for emotions, empathy and social behaviour: evidence from right and left handers with frontotemporal dementia. Neurocase. 2001;7:145–160. doi: 10.1093/neucas/7.2.145. [DOI] [PubMed] [Google Scholar]
- Premack D, Woodruff G. Does the chimpanzee have a theory of mind? Behav Brain Sci. 1978;1:515–526. [Google Scholar]
- Quinette P, Guillery B, Desgranges B, de la Sayette V, Viader F, Eustache F. Working memory and executive functions in transient global amnesia. Brain. 2003;126:1917–1934. doi: 10.1093/brain/awg201. [DOI] [PubMed] [Google Scholar]
- Raven J. Guide to using the coloured progressive matrices. London: Lewis; 1965. [Google Scholar]
- Reitan RM. Validity of the trail making test as an indication of organic brain damage. Percept Motor Skill. 1958;8 :271–286. [Google Scholar]
- Rabin JS, Gilboa A, Stuss DT, Mar RA, Rosenbaum RS. Common and unique neural correlates of autobiographical memory and theory of mind. J Cog Neurosci. 2010;22:1095–1111. doi: 10.1162/jocn.2009.21344. [DOI] [PubMed] [Google Scholar]
- Rankin KP, Kramer JH, Miller BL. Patterns of cognitive and emotional empathy in frontotemporal lobar degeneration. Cogn Behav Neurol. 2005;18:28–36. doi: 10.1097/01.wnn.0000152225.05377.ab. [DOI] [PubMed] [Google Scholar]
- Rankin KP, Salazar A, Gorno-Tempini ML, Sollberger M, Wilson SM, Pavlic D, et al. Detecting sarcasm from paralinguistic cues: anatomic and cognitive correlates in neurodegenerative disease. Neuroimage. 2009;47:2005–2015. doi: 10.1016/j.neuroimage.2009.05.077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen HJ, Pace-Savitsky K, Perry RJ, Kramer JH, Miller BL, Levenson RW. Recognition of emotion in the frontal and temporal variants of frontotemporal dementia. Dement Geriatr Cogn Disord. 2004;17:277–281. doi: 10.1159/000077154. [DOI] [PubMed] [Google Scholar]
- Rosen HJ, Perry RJ, Murphy J, Kramer JH, Mychack P, Schuff N, et al. Emotion comprehension in the temporal variant of frontotemporal dementia. Brain. 2002;125:2286–2295. doi: 10.1093/brain/awf225. [DOI] [PubMed] [Google Scholar]
- Ross LA, Olson IR. Social cognition and the anterior temporal lobes. Neuroimage. 2010;49:3452–3462. doi: 10.1016/j.neuroimage.2009.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruby P, Schmidt C, Hogge M, D’Argembeau A, Collette F, Salmon E. Social mind representation: where does it fail in frontotemporal dementia? J Cogn Neurosci. 2007;19:671–83. doi: 10.1162/jocn.2007.19.4.671. [DOI] [PubMed] [Google Scholar]
- Sabbagh MA. Understanding orbitofrontal contributions to theory-of-mind reasoning: implications for autism. Brain Cogn. 2004;55:209–219. doi: 10.1016/j.bandc.2003.04.002. [DOI] [PubMed] [Google Scholar]
- Samson D, Apperly IA, Kathirgamanathan U, Humphreys GW. Seeing it my way: a case of a selective deficit in inhibiting self-perspective. Brain. 2005;128:1102–1111. doi: 10.1093/brain/awh464. [DOI] [PubMed] [Google Scholar]
- Schilbach L, Wohlschlaeger AM, Kraemer NC, Newen A, Shah NJ, Fink GR, et al. Being with virtual others: neural correlates of social interaction. Neuropsychologia. 2006;44:718–730. doi: 10.1016/j.neuropsychologia.2005.07.017. [DOI] [PubMed] [Google Scholar]
- Schultz RT, Grelotti DJ, Klin A, Kleinman J, Van der Gaag C, Marois R, et al. The role of the fusiform face area in social cognition: implications for the pathobiology of autism. Philos T Roy Soc B. 2003;358:415–427. doi: 10.1098/rstb.2002.1208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shamay-Tsoory SG, Tomer R, Goldsher D, Berger BD, Aharon-Peretz J. Impairment in cognitive and affective empathy in patients with brain lesions: anatomical and cognitive correlates. J Clin Exp Neuropsychol. 2004;26:1113–1127. doi: 10.1080/13803390490515531. [DOI] [PubMed] [Google Scholar]
- Snowden JS, Bathgate D, Varma A, Blackshaw A, Gibbons ZC, Neary D. Distinct behavioural profiles in frontotemporal dementia and semantic dementia. J Neurol Neurosurg Ps. 2001;70:323–332. doi: 10.1136/jnnp.70.3.323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snowden JS, Gibbons ZC, Blackshaw A, Doubleday E, Thompson J, Craufurd D, et al. Social cognition in frontotemporal dementia and Huntington’s disease. Neuropsychologia. 2003;41:688–701. doi: 10.1016/s0028-3932(02)00221-x. [DOI] [PubMed] [Google Scholar]
- Snowden JS, Goulding PJ, Neary D. Semantic dementia: a form of circumscribed cerebral atrophy. Behav Neurol. 1989;2:167–182. [Google Scholar]
- Spreng RN, Grady C. Patterns of brain activity supporting autobiographical memory, prospection and theory-of-mind and their relationship to the default mode network. J Cognitive Neurosci. 2010;22:1112–1123. doi: 10.1162/jocn.2009.21282. [DOI] [PubMed] [Google Scholar]
- Stroop J. Studies of interference in serial verbal reactions. J Exp Psych. 1935;28:643–662. [Google Scholar]
- Takahashi H, Matsuura M, Koeda M, Yahata N, Suhara T, Kato M, et al. Brain activations during judgments of positive self-conscious emotion and positive basic emotion: pride and joy. Cereb Cortex. 2008;18:898–903. doi: 10.1093/cercor/bhm120. [DOI] [PubMed] [Google Scholar]
- Violon A, Wijns C. Test de perception et d’apprentissage progressif en mémoire visuelle. Braine le Château, Belgium: L’Application des techniques modernes; 1984. Le test de la ruche. [Google Scholar]
- Vogeley K, Bussfeld P, Newen A, Herrmann S, Happé F, Falkai P, et al. Mind reading: neural mechanisms of theory of mind and self-perspective. Neuroimage. 2001;14:170–181. doi: 10.1006/nimg.2001.0789. [DOI] [PubMed] [Google Scholar]
- Völlm BA, Taylor ANW, Richardson P, Corcoran R, Stirling J, McKie S, et al. Neuronal correlates of theory of mind and empathy: a functional magnetic resonance imaging study in a nonverbal task. Neuroimage. 2006;29:90–98. doi: 10.1016/j.neuroimage.2005.07.022. [DOI] [PubMed] [Google Scholar]
- Walter H, Adenzato M, Ciaramidaro A, Enrici I, Pia L, Bara BG. Understanding intentions in social interaction: the role of the anterior paracingulate cortex. J Cogn Neurosci. 2004;16:1854–1863. doi: 10.1162/0898929042947838. [DOI] [PubMed] [Google Scholar]
- Wechsler D. Echelle clinique de mémoire MEM-III. Paris: Les éditions du Centre de Psychologie Appliquée; 2001. [Google Scholar]
- Wimmer H, Perner J. Beliefs about beliefs: representation and constraining function of wrong beliefs in young children’s understanding of deception. Cognition. 1983;13:103–128. doi: 10.1016/0010-0277(83)90004-5. [DOI] [PubMed] [Google Scholar]
- Wittenberg D, Possin KL, Rascovsky K, Rankin KP, Miller BL, Kramer JH. The early neuropsychological and behavioral characteristics of frontotemporal dementia. Neuropsychol Rev. 2008;18:91–102. doi: 10.1007/s11065-008-9056-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1983;17:37–49. doi: 10.1016/0022-3956(82)90033-4. [DOI] [PubMed] [Google Scholar]
- Zamboni G, Grafman J, Krueger F, Knutson KM, Huey ED. Anosognosia for behavioral disturbances in frontotemporal dementia and corticobasal syndrome: a voxel-based morphometry study. Dement Geriatr Cogn Disord. 2010;29:88–96. doi: 10.1159/000255141. [DOI] [PMC free article] [PubMed] [Google Scholar]