

Abstract
Introduction:
Suicide is one of the most prominent problems in health care system in current Iran. It could be impacted by various factors such as social, economic, individual and so on. Researchers show that socio-economic factors and suicide has significantly related. The people in low social class may more engage with social problems than higher social class. They may confront to problems such as crime, violence, unemployment, financial hardship, population density, disorder personality, etc. However, these difficulties could be resulted from relationship of inequality socio-economic and mental or physical health. This research attempted to examine social class status and its relationship with parts of suicide characteristics.
Methods:
This study applied a descriptive approach. In the cross-sectional research 179 patients who attempted suicide and admitted to the toxicology ward of Nour hospital and to the burning ward of Imam Mousa Kazem hospital, in Isfahan, during a period of 6 months in 2010 were recruited. The randomize sampling for patients admitted to toxicology ward and census for burning ward are applied. Data collected through a questionnaire which Chronbagh coefficient’s alpha was calculated (r= 0/72). Data was analyzed in SPSS software.
Findings:
The data showed that the majority of patients who attempted suicide were young married women who had diploma and under diploma of level education. They were housewife, engaged in education and unemployment. Finding showed that there are no significant relationships between sex, age, marital status, frequency of attempted suicide and their social class. But there is significant relationship between methods of suicide and social class. Similarly, there are significant relationship between social factors (i.e. family friction, betrothal, unemployment, financial problems and so on) effected on suicide and their social classes. Parts of findings were supported by previous studies.
Key words: Attempted suicide, Social class.
1. INTRODUCTION
Suicide is both a serious medical problem and an important social problem. It is claimed there are three hypotheses related to suicide: first, suicide may be considered as a psychological phenomenon (1), second, suicide may be seen as a social phenomenon (2) and third, suicide may be explained as a phenomenon associated with other psychiatric disorders, and genetic problems (3). Then suicide could be considered as a phenomenon resulting from biological factors, psychological and social issues.
From Durkhiem’s time, when he raised arguments (2) regarding to social factors related to suicide, many studies have tried to explain suicide social risk factors. Some researchers (4, 5) believe that social and economic pressures have an impact on suicide. They show, for example, unemployment makes an undeniable impact on the suicide (6, 7, 8). Other studies show (9) that people in lower social classes are more in risk social problems, such as crime, violence, financial problems, population density and personality disorders. These issues led to more attention to the relationship between social inequality and health, for instance issue such as suicide. It has been reported that in America (10) and Australia (11) there is a negative correlation between suicide rates and socioeconomic status. On the other hand, in England, more complex results from this relationship have been reported (12). In this country, in the late nineteenth century suicide rate among higher social classes was so more, but in the mid-twentieth century, the highest and lowest social classes had the highest risk of suicide. The highest suicide rate in the late twentieth century was found among the lower social classes (11).
It has been reported that the prevalence of suicide in recent years has increased (13, 14). Researches in Iran show that suicide rates in some undeveloped areas, such as province of Ilam are relatively high (15). Studies conducted on Iranian Kurdish (16) shows that unemployment is associated with their suicidal action. Other studies also suggest that there are relationships between attempted suicide with unemployment and education levels (17). However, this study seeks to understand what people with social and economic backgrounds tend to have suicidal behavior. The main aim of this study is to explore social class status of people who have attempted suicide. In this way, this research try to examine social class status and its relationship with parts of suicide characteristics such as methods of suicide attempt, numbers of suicide attempts and causes of suicide attempts.
2. METHOD
This is a survey research that applied a descriptive-analytic approach. Statistical society included patients who attempted suicide and admitted to the toxicology ward of Nour hospital and to the burning ward of Imam Musa Kazem hospital, in Isfahan, during a period of 6 months in 2010. Total 179 patients were selected by random sampling method, thus the research team visit hospital emergency randomly (i.e. two days each week) and chose deliberate self-harm patients. The number of patients who used method of burning for suicide was less than the patient used overdose. Therefore, research team visit hospital of Imam Musa Kazem only one day a week and asked patients hospitalized to answer the questions, if they were able to respond them . In the other hand, in this stage census was conducted. The criteria for participation to this research included: attempted suicide by overdose, poison or self-burning, be admitted by hospitals of Nour and Imam Musa Kazem, patients’ satisfaction to answer the questions, possibility to communicate with them, and physically as well as mentally be able to respond the questions. The exclusion criteria were patient’s disagreement to continue after the initial approval.
The instrument used for this research was questionnaire. The questionnaire was constructed by researchers and included demographic variables, number of suicide attempted, place and time of suicide attempt, and method of attempted suicide. Social class questionnaire was constructed according to the Iranian literature of social class (18, 19). It is included: patient’s income, education, accommodation, occupation, his/ her spouse’ job house and land ownership as well as car type and model. The variety of consumption and purchase of equipment for home such as clothes and other necessities and personal consumptions were included. The person’s life style and family life style such as travel, food, sport and using outdoor foods also employed. The indicators of income, education, occupation and employment status calculated as ‘one degree coefficient’ and indicators of parents’ education and spouse education calculated as ‘two degree coefficient’. All these indicators added and then divided to three, high, middle and low social class. Content validity was taken according to professional staff point of views. The reliability of questionnaire was calculated according to coefficients Cronbach’s alpha (r = .072). Collected data were analyzed by SPSS software. For this, Chi-square test employed for possibility relationship between social class and of causes of suicide, methods of suicide, social and economic factors, marital status and sex variables. The test of Anova used to possibility relationship between social class and age variables.
3. FINDINGS
The demographic characteristics show that maximum age of respondents is 68 and minimum is 14 years, the average age of respondents is 26.30 and their standard deviation (SD) is 8.51. 74.3% respondents are female, 25.7% are male, 58.7% are married, 38% are single, 1.1% are widow and 2.2% are divorced. The educational level of respondents show that 39.7% of respondents have diploma, 10.6% have a bachelor’s degree, 7.8% are illiterate and finally 0.6% have a higher degree of Ph.D. Occupational situations of respondents indicated 17.9% are employed, 20.1% engaged education in school and university, 43.6% are housewives, 2.8% are soldiers and 15.1% are unemployed.
The combination between main dimensions of social class (i.e. education, occupational class and income) and other dimensions (i.e. family consumptions, life style, etc) shows that majority of respondents (i.e. 40.8%) take place in middle social class, 24.6% take place in low social class and 20.1% take place in high social class.
Table 1 shows the frequency distribution of respondents according to methods of suicide attempts and the number of suicide. As it display 69.8% of respondents took overdose for suicide attempts, 20.7% burns him/her self and 9.5% of respondents used poison to attempt suicide. This table also shows that 78.8% of respondents attempted suicide for the first time, 8.4% of them for second time, 5% of them for the third time and 4.1% of them for the fourth time.
Table 1.
Frequency distribution of respondents according to method of suicide attempts and number of suicide attempts
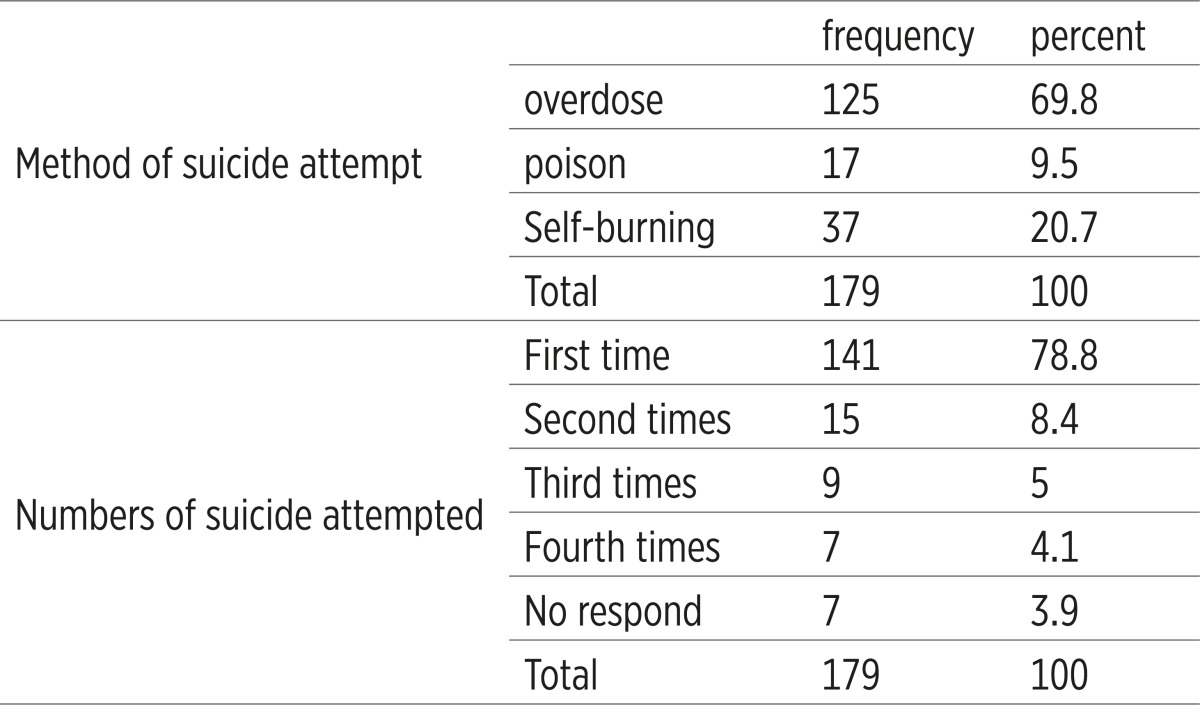 |
Table 2 shows the results of statistical tests of relationship between social class status with age, sex and marital status of patients attempted suicide. As is clear there is no relationship between these variables and their social classes.
Table 2.
Results of statistical tests relationship between social class status with age, sex and marital status of patients attempted suicide
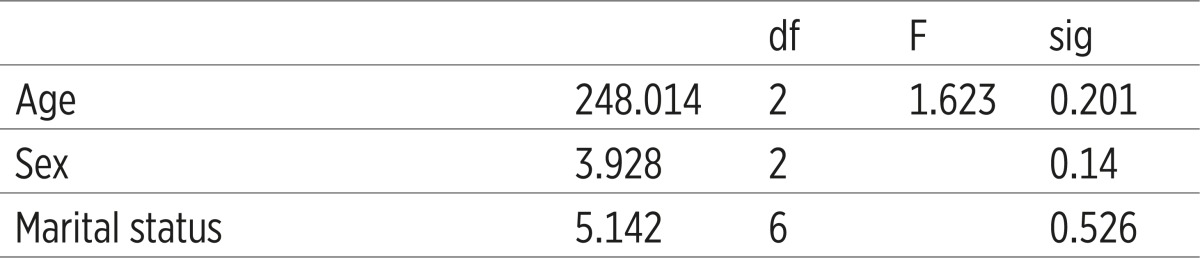 |
Table 3 shows relationship between social class of respondent and methods of suicide. The results of Chi-square test and p-value = 0.000 indicate that there is significant relationship between social class and method suicide attempt. High and middle social classes used the methods of overdose and poison and low social class patients use self-burning.
Table 3.
Relationship between social class of respondent and methods of suicide
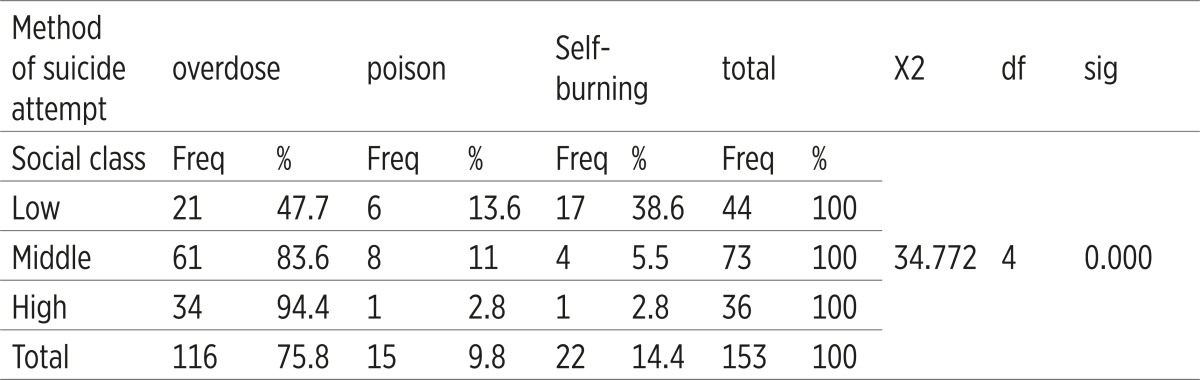 |
Table 4 shows relationship between social class of respondent and the numbers of suicide attempts. The results of Chi-square test and p-value = 0.396 indicate that there is no significant relationship between social class and the numbers of suicide attempt.
Table 4.
Relationship between social class of respondent and the numbers of suicide attempts
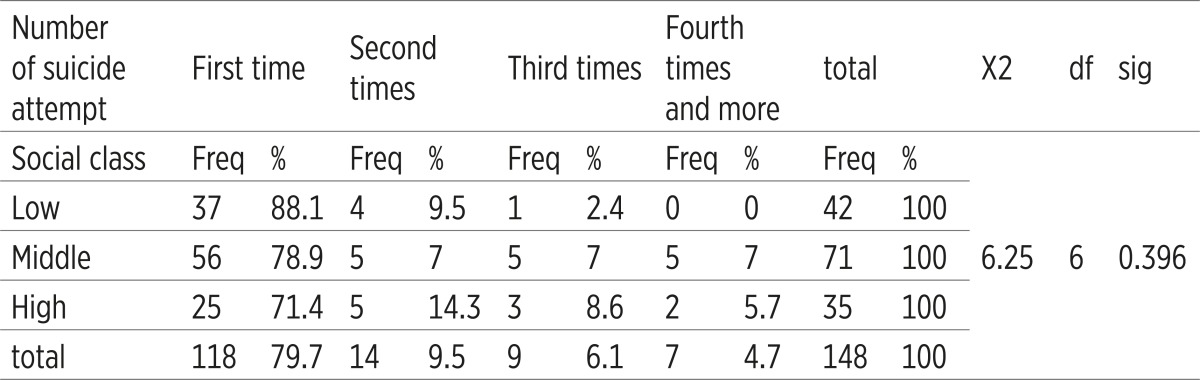 |
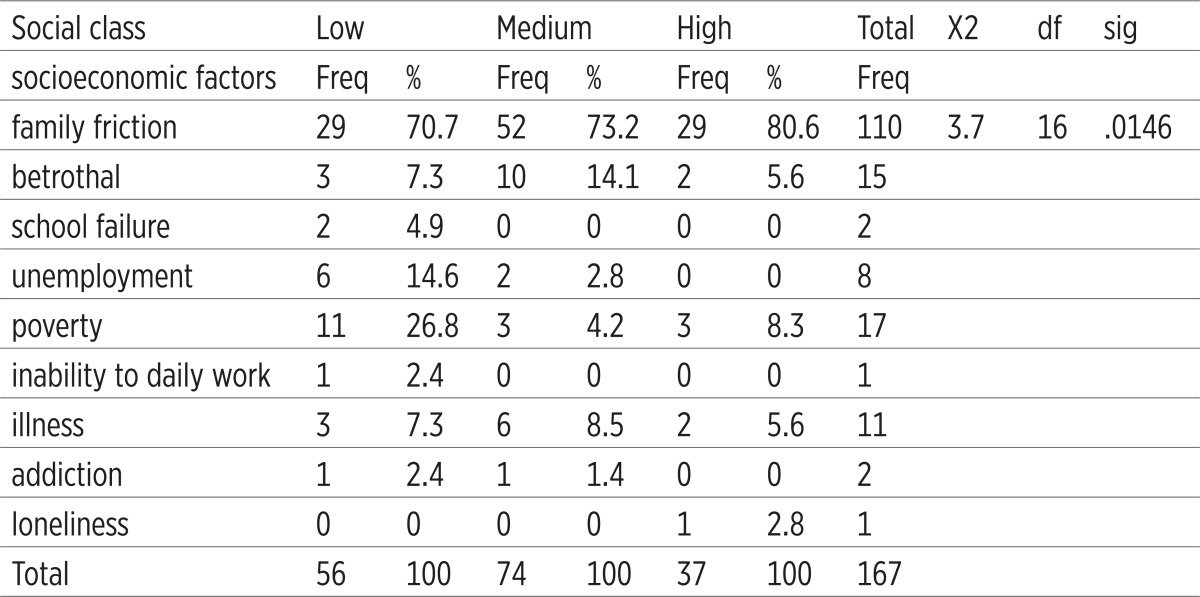
Table 5 shows relationship between social class of respondent and socioeconomic factors affected on their suicide attempts. The results of Chi-square test and p-value = 0.015 indicate that there is a significant relationship between these variables. In other words, it can be argued that there are significant relationship between variables of family friction, betrothal, school failure, poverty, unemployment, inability to daily work, illness, addiction and loneliness with variable of social class respondents.
Table 5.
Relationship between social class of respondent and socioeconomic factors affected on their suicide attempts
 |
4. DISCUSSION
The main purpose of this research was to examine social class status and its relationship with parts of suicide characteristics. The other aims were to study of relationship between social class status with variables of socioeconomic factors related to attempted suicide, methods of attempting suicide and number of suicide. This research also focused on the relationship between social class of patients attempted suicide and contextual variables such as age, sex and marital status.
Findings suggest that cases are married young women that their education levels are diploma and under diploma. The most cases could categorize as housewives and unemployed. They most method has been used for attempted suicide are overdose and poison. Their main social classes of respondents are middle social class and then low and high social classes. In other words, most of respondents could take place on the middle and low socioeconomic status. Findings of this research also show that there are significant relationship between patient’s social class and their methods used for attempted suicide. Most patients in middle social class take overdose and most patients in low social class used method of self-burning for suicide attempts.
Findings also indicate there is no significant relationship between social class and number of suicide attempted. In other words, the times of attempting suicide do not depended on the social class status. It means patients with lower or higher social classes do not necessarily have highest or lowest number of suicide attempts and all those who have attempted suicide, regardless of social class are at risk of suicide for one or more times.
Data also suggested that it could be found relationship between patient’s socioeconomic causes of suicide and their social class. In other words, it could find significant differences between high, middle and low social class in the socioeconomic causes of suicide. It can be argued that there is a significant relationship between family friction, betrothal, school failure, unemployment, poverty, inability daily work, illness, addiction, loneliness and social class.
The findings also show that there is no relationship between age and responded social class, in the other hand, in all social classes can be found patients of any age who attempted suicide. There is not a significant relationship between gender and social class of patients. It could not find any relationship between marital status and social classes. In other words, it could find patients whether single or married in all social classes.
According to the findings, most respondents are married young women, this result is similar with other studies in different parts of Iran (20-25). This study also shows that people with lower education have more suicide attempts. This result is also corresponded with findings of other studies in Iran (14, 20).
These findings of this study are not alongside with Mofid’s work (16). He has shown that more suicide is occurred among high level education individuals than the low-literate and illiterate. The findings also different from with other studies in some countries (26) which have shown higher education is much increased risk of suicide.
Findings also showed that prevalence of suicide among people with middle and lower social is more. The results also suggest that there is a significant relationship between socioeconomic causes of suicide and different social classes, in this way, the main cause for suicide in lower classes includes unemployment, poverty, school failure and addiction. The findings of another work (27) showed that 70% of suicides in Iran are occurred among people with low socioeconomic status. The main indicators of low socioeconomic status are poverty, unemployment, low education and low income. These indicators have been considered in various studies in Iran, for example some researchers showed that poverty and the rate of suicide are interconnected (28), others show that unemployed individuals and low income are more than other subjected to suicide (29). However, the international study confirms relationship between suicide and unemployment (7). Other study among Asian countries that relatively more prosperous, particularly those which have developed rapidly such as South Korea, India, even Newlands shows that suicides are more likely to occur among individuals experiencing poverty unemployment, and/or debts (30, 31, 32, 33). These causes also could be found in some less developed countries like Sri Lanka (34). World Health Organization (WHO) in its report consider on the poverty as one the main factor related to suicide, especially when it combined with other factors likes stress and mental illness (35).
The main method for suicide attempt in lower social class in this study is self-burning, this findings is corresponded to the other work in Iran (27) that shows 70% people who employed self-burning for suicide take place a low socioeconomic status. Another works also shows that the method of self-burning occurs among illiterate, low literacy and rural people who have low socioeconomic status (36). However, the means of burning likely is more accessible for rural people. Using this method is violent and saving victim is so difficult.
It could suggest the socioeconomic situation of people attempted suicide at the national level is a sensitive issue that it could visible inequality in attempted suicide. It is also suggested researcher focused on the prevention of suicide. It seems different social classes have different reasons for suicide, thus, independent studies that focus on prevention in different social classes are recommended.
Conflict of interest
None declared.
REFERENCES
- 1.Freud S. Mourning and Melancholia. 1917. In: Strachey J, editor. Standard Edition of the Complete Psychological Works of Sigmund Freud. London: Hogarth; 1957. pp. 237–260. [Google Scholar]
- 2.Durkheim E. Suicide: a study in sociology. Great Britain: Routledge; 1952. [Google Scholar]
- 3.Erkki T, Markus M, Henriksson HM. Suicide in major depression. American Journal of Psychiatry. 1994;151:530–536. doi: 10.1176/ajp.151.4.530. [DOI] [PubMed] [Google Scholar]
- 4.Kishi Y, Robinson RG, Kosier JT. Suicidal Ideation among Patients with Acute Life-threatening Physical Illness: Patients with Stroke, Traumatic Brain Injury, Myocardial Infection and Spinal Cord Injury. Psychosomatics. 2001;42:382–390. doi: 10.1176/appi.psy.42.5.382. [DOI] [PubMed] [Google Scholar]
- 5.Schutt RK, Meschede T, Rierdan J. Distress, Suicidal Thoughts and Social Support among Homless Adults. Journal of Health and Social Behaviour. 1994;35:134–142. [PubMed] [Google Scholar]
- 6.Blakely TA, Collings SC, Atkinson J. Unemployment and Suicide, Eviedence for a causal association? Journal of Epidemiology and Community Health. 2003;57:594–600. doi: 10.1136/jech.57.8.594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Platt S. Unemployment and Suicidal Behaviour: A Review of the Literature. Social Science and Medicine. 1994;19:93–115. doi: 10.1016/0277-9536(84)90276-4. [DOI] [PubMed] [Google Scholar]
- 8.Platt S, Hawton K, editors. Suicide behaviour and the laubour market. New York: Wiley; 2000. [Google Scholar]
- 9.Buglass D. The Relation of Social Class to the Characteristics and treatment of Parasuicide. Social Psychiatry. 1976;11:107–119. [Google Scholar]
- 10.Kposowa AJ. Unemployment and Suicide: A Cohort Analysis of Social Factor Predicting Suicide in the US: National Longitudinal Mortality Study. Psychological Medicine. 1999;31:127–138. doi: 10.1017/s0033291799002925. [DOI] [PubMed] [Google Scholar]
- 11.Taylor R, Morrell S, Slaytor E, Ford P. Suicide in Urban New South Wales, Australia 1985-1994. Socio-economic and Migrant Interactions. Social Science and Medicine. 1998;47:1677–1686. doi: 10.1016/s0277-9536(98)00243-3. [DOI] [PubMed] [Google Scholar]
- 12.Hawton K, Harris L, Simkin S, Bale E, Bond A. Social Class and Suicidal Behaviour: the Associations between Social Class and the Characteristiscs of Delibetate self-harm Patients and the Treatment They Are Offererd. Social Psychiatry and psychiatric Epidemiology. 2001;36:437–443. doi: 10.1007/s001270170021. [DOI] [PubMed] [Google Scholar]
- 13.Ghoreishi SA, Mousavinasab N. Systematic Review of Resaerches on Suicide and Suicide Attempt in Iran. Iranian Journal of Psychiatry and Clinical psychology. 2008;14:115–121. [Google Scholar]
- 14.Moradi S, Khademi A. Evaluation of suicides resulting in death in Iran, comparing with the world rates. Scientific Journal of Forensic Medicine. 2002;8(27):16–21. [Google Scholar]
- 15.Janghorbani M, Sharifirad G. Completed and attempted suicide in Ilam, Iran (1995-2002): increase and associated factors. Archives of Iranian Medicine. 2005;8(2):199–229. [Google Scholar]
- 16.Mofidi N, Ghazinour M, Salander-Renberg E, Richter J. Attitudes towards suicide among Kurdish people in Iran. Soc Psychiatry psychiatr Epidemiol. 2008;43:291–298. doi: 10.1007/s00127-007-0296-7. [DOI] [PubMed] [Google Scholar]
- 17.Mohammadi MR, Ghanizadeh A, Rahgozart M, Noorbala AA, Malekafzali H, Davidian H, et al. Suicidal attempt and psychiatric disorders in Iran. Suicide and Life-Threatening Behaviour. 2005;35(3):390. doi: 10.1521/suli.2005.35.3.309. [DOI] [PubMed] [Google Scholar]
- 18.Keyvanara M, Rabbani R, Zhianpour M. Social stratification and physical improvements. Women’s Strategic Studies. 2010;12(47) [Google Scholar]
- 19.Masoudnia M, Orayzi E, Rabbani R, Zamani AR, Ahmadi SA. Impact of Social Class on Rheumatoid Arthritis Patient’s Perception of Illness Symptoms & Pain. Daneshvar Raftar. 2005;1(13):37–46. [Google Scholar]
- 20.Khazaee H, Parvizifard A. Survey Demographic Characteristics and Evaluation of psychological Individuals who Attempted Suicide in Tabriz. Behbood. 2003;7(18):42–51. [Google Scholar]
- 21.Ghaedi H, Hashemi SM, Mohammadi M, Sniei F, Hosseini SY, Jabarnejad A. Epidemilogical study on suicide attempts in the City of Dashtestan in 2004. Dena Quarterly Journal of Yasuj Faculty of Nursing and Midwifery. 2006;1(3):53–60. [Google Scholar]
- 22.Saberi-Zafarqandi MB, Ghorbani R, Mousavi Sh. Epidemiologic study on suicide attempt in affiliated hospitals of Semnan University of medical sciences. Koomesh. 2005;6(4):311–318. [Google Scholar]
- 23.Salari lak S, Entezar M, Afshani MT, Abassi H. Survey of factors affected on the rate of suicide in West Azarbayejan province. Urmia Medical Journal. 2006;17(2):9–15. [Google Scholar]
- 24.Shamsi khani S, Rahgoo A, Fallahi KMR. Effects of problem solving training on coping skills of suicidal clients. Iranian Journal of Nursing Research. 2007;1(3):31–39. [Google Scholar]
- 25.Taziki MH, Taziki SA, Semnani SH, Rajaei S, Gol Alipour MJ, Ezad KH, et al. Epidemiologycal survey of suicide in Golestan province in the North of Iran (2003) Jornal of Mazandaran University of Medical Sciences. 2007;16(55):27–77. [Google Scholar]
- 26.Kaplan HI, Sadock BJ. Kaplan and Sadock Synopsis of psychiatry. 9th edition. Lippincott: Williams and wilkins; 2003. [Google Scholar]
- 27.Lari RA, Alaghebandan R. Epidemiological study of self- inflicted burns in Tehran, Iran. Journal of Burn care Rehabilitation. 2003;24(1):15–20. doi: 10.1097/00004630-200301000-00005. [DOI] [PubMed] [Google Scholar]
- 28.Anbari M, Bahrami A. Survey of Poverty and violence on the rate of suicide in Iran: case study in the rural of city of Poldokhtar. Iranian Journal of Social Problems. 2010;1(2) [Google Scholar]
- 29.Ahmadi A, Janbazi Sh, Laghaei Z, Ahmadi A, Davarinejad O, Haidari MB. Epidemiological study of committed self-inflicted burns admitted to the Hospitals of Kermanshah University of Medical Sciences, Iran. The Quarterly Journal of Fundamentals of Mental Health. 2006;8(29, 30):23–35. [Google Scholar]
- 30.Kim M-D, Hong S-C, Lee S-Y, Kwak Y-S, Lee C-I, Hwang S-W, et al. Suicide Risk in Relation to Social Class: A National Register-Based Study of Adult Suicides in Korea, 1999-2001. International Journal of Social Psychiatry. 2006;52(2):138–151. doi: 10.1177/0020764006061254. [DOI] [PubMed] [Google Scholar]
- 31.Collings SCD. Suicide Trends and Social Factors–New Zealand from 1981 to 1999: Analyzes from the New Zealand Census-Mortality Study. Wellington: University of Otago; 2005. [Google Scholar]
- 32.Guruvaj G, Isaac G, Isaac MK, Subbakrishna DK, Ranjani R. Risk factors for completed suicide: A case-control study from Bangalore, India. International Journal of Injury Control and Safety Promotion. 2004;11:183–191. doi: 10.1080/156609704/233/289706. [DOI] [PubMed] [Google Scholar]
- 33.Zhang J, Conwell Y, Zhou L, Jiang C. Culture, risk factors and suicide in rural China: A psychological autopsy case control study. Acta Psychiatrica Scandinavica. 2004;110:430–437. doi: 10.1111/j.1600-0447.2004.00388.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Silva KT, Pushpakumana R, editors. Suicide and sexual anomie in a new settlement in Sri Lanka. Kandy: Institute of fundamental studies; 1989. [Google Scholar]
- 35.Jonclose M. The poorest first: WHO is activities to help the people in greatest need. World Health Forum. 1998;19(2):182–187. [PubMed] [Google Scholar]
- 36.Ghalambor A, Zarei J, Pipelzadeh MH. Assessment of Personal and Social Characteristics as Risk Factors in Self-Inflicted Burns. Journal of Medical scientific, Jondishapour Medical University. 2010;9(3):233–346. [Google Scholar]