

Abstract
Introduction:
The main objective of the present study is to review the psychological profile of female patients with borderline personality disorder in the women referring to the Centers of Counseling and Psychological Services at Isfahan city based on MMPI-2 test and comparing them with ordinary women.
Method:
The present study is of the type of cause-comparative and the selection of examinees was done in form of random sampling with 50 women with the BPD and 50 ordinary women and through confirmation of test recognition of MCMI-III and clinical interviews. In addition, 370 questions of MMPI-2 have also been implemented.
Results:
The results of this research showed a significant difference in validity of scales and the clinical scales of MMPI-2 test among women with BPD and regular women. The results of MANOVA test with the power of valuable test confirmed the existing differences.
Conclusion:
The obtained results shows that female patients with BPD has a specific and different psychological profile as compared with ordinary (regular) women and the obtained profile can be used in recognition and forecasting any disorder.
Key words: Borderline Personality Disorder, MMPI-2 Test, MCMI-III, psychological Profile.
1. INTRODUCTION
Patients with Borderline Personality Disorder (BPD) are in the border of neurosis and psychosis. Their feature is instability in emotional, mood, behavior and relation statues and their self-image. This disorder is known as temporary Schizophrenia, pseudo-Neurotic Schizophrenia or hidden Schizophrenia (1).
The spread of this kind of disorder is prevailing one to two percents among the public population and in women; it is two times of those of the men. It seems that these patients are always in crisis and the fast mood swing is prevailing among them. It is also possible that they experience mental distress with a short life or micro-psychotic attacks. However, a fully-fledged attack of mental distress is not observed in these series of patients. The behavior of these patients is not predictable and they never reach efficiency which they are supposed to present (2). Frequent Masochism, attracting the attention of others, expressing anger, feeling dependency, and enmity are characteristics of these types of patients and their individual relationships are disrupted and irregular. These patients enjoy a capability to transfer their mental distress, so that they can experience the therapist as a “bad parent” who has been detached (3). They might become dependent on someone to whom they feel are close to and if they are disappointed with their sincere friends, they express a very intensive anger. These kinds of patients are seeking relationship in order to heal their disease-like behavior. Irregularity in this search and feeling of futile and impatience are some other symptoms. They use a defense mechanism like projective identification and splitting frequently. Most of them are facing defeat in their important relationships. They are like sad and disappointed individuals and are intensively seeking peace and attention.
However, they afraid of something and their friendship period are short. They know themselves as someone in lack of a sincerer and constant partner (4). One of the most important characteristics of patients with BPD is the inefficiency of their system of excitements which is associated with their inability in conformity with existing responses (5).
The recognition of this type of disorder is usually before the age of 40 and some biochemical and psychological factors have been considered to be effective in the formation of this disorder. These patients show a regular reasoning power in the structural tests such as Wechsler Adult Intelligence Scale, WAIS and in projective unstructured tests like The Rorschach test, the disorders related to thinking processing is observable in them (2).
The treatments presented in this patients are emphasizing on set limits and empathy for example to determine the periods of giving calls, showing quarrelsome attitude to treatment staff and the frequency of their meeting with therapist (6).
Among other treatment methods, one may refer to the specific integration with the psychological language which is known as analytical psychology or CAT (7). On the other hands, design pivot treatment is another treatment method which has been effective in recent years (8). Moreover, medical treatments have also been useful to control anger, enmity and distress transit attacks and disappointment (2). On the other hands, many researches have dealt with the relationship between bipolar mood disorder (manic depression) and BPD and also the difference between these two disorders from causative and diagnostic aspects (9). The BPD and Bipolar mood disorder have some common clinical common features and this issue can give rise to the emergence of some problems such as false positive or false negative and difficulties. Emotional instabilities and shocks are common features of these two disorders (10).
Efforts to identify recognition signs and features of BPD have been the subject-matter of many researches. For example, it is possible to mention the application of Schizotypal Trait Questionnaire-B Form (STB) in order to measure the characteristics of BPD and its acceptable power in measuring the symptoms of BPD (11). Also the application of the questionnaire of Seresht and Monsh Cloninger (TCI-125) in the patients with BPD (12). Since MMPI-2 test is one of the most consuming tests in clinical testing (13) , the present research with an aim to study the personality profile of women with BPID is pursuing to identify the personality profile of these patients based on MMPI-2 test.
2. METHOD
The present research with regard to its objectives and nature is of the type of causative-comparative research. In other words, in this research the personality profile of women with BPD and ordinary individuals have been compared through MMPI-2 test. The statistical community of the research includes all women with BPD referring to Centers of Isfahan during 2009-2010. They have been selected, estimated and studied in random sampling out of the 50 female patients with BPD (using MCMI-II questionnaires and clinical interview) with regard to the variance of previous studies.
So, out of the Counseling Centers of Isfahan, with previous coordination with the reception unit, in random form, 50 patients with BPD based on the psychometric unit and therapist were identified. Then, once again, they were placed under the MCMI-III test by a psycho therapist and were introduced to the psychiatrist for clinical interviews. The individuals who were identified as with BPD with regard to the two above scales formed the present research sample. Also 50 regular women (those in lack of any psychological disorder) were selected from five districts of Isfahan randomly.
2.1. Research Instruments
The Minnesota Multiphasic Personality Inventory (MMPI-2);
Clinical interview based on DSMIV-TR;
MCMI-III Test;
The Minnesota Multiphasic Personality Inventory (MMPI-2): This test is one of the most consuming clinical personality questionnaires and more than 10000 research sources have been published about it (14, 15).
The test being used in this research is MMPI-2 form with 370 questions (it has been translated into Persian by Fereshteh Motabi, Ali Shahrami, Mohammad Naghi Barahani, Jafar Bolhari, Reza Zaman in Tehran Institute of Psychiatry) and enjoys a good validity and reliability. This test has 13 standard scales of which 3 scales are related to validity and 10 others to related clinical and personality indexes. All MMPI-2 scales are fully durable and the scope of change of their stability coefficients is from 0/71 (ma scale) to 0/84 (pt scale).
Million Clinical Multi Axial Inventory (MCMI-III): it is a standardized self measuring questionnaire which measures a broad scope of data related to personality, emotional conformity and attitudes of cases under examination of the test.
The copy of MCMI-III test has 175 Articles which are scored under 28 separate scales based on the following classification: Indexes of changeability-models of clinical personality, intensive pathological study of the personality, clinical symptoms and intensive symptoms. This scale along with the Articles forming them is in conformity with the theory of personality of DSM-IV. The studies of validity and reliability of MCMIIII show that this questionnaire in general is a well structured psychometrical instrument.
The sizes of its internal conformity are in particular high and have a high re-testing credit coefficient with a mean of 0/91. The clinical interview based on DSM IV-TR: In this research, in order to select patients, the instruments of clinical interview based on DSM IV-TR were used and the patients with BPD were included in the research.
2.2. Method of Data Analysis
In this research, in order to analyze the data, the mean, standard deviation and for testing the assumptions, the Multivariate analysis of variance (MANOVA) was used.
3. RESULTS
In this part, first the descriptive analysis including mean and standard deviation of the related scale in two groups of women with BPD and regular (ordinary) women in relation with their performance in MMPI-2 test and then test of assumptions are presented.
The data of Table 1 shows the mean and standard deviation of indexes of MMPI-2 test validity. The data in Table 2 shows the mean and standard deviation of the group of women with BPD and Regular women in clinical indexes of MMPI-2 test.
Table 1.
Mean and Standard Deviation of Two Groups of Women with BPD and Regular in Validity Indexes of MMPI-2
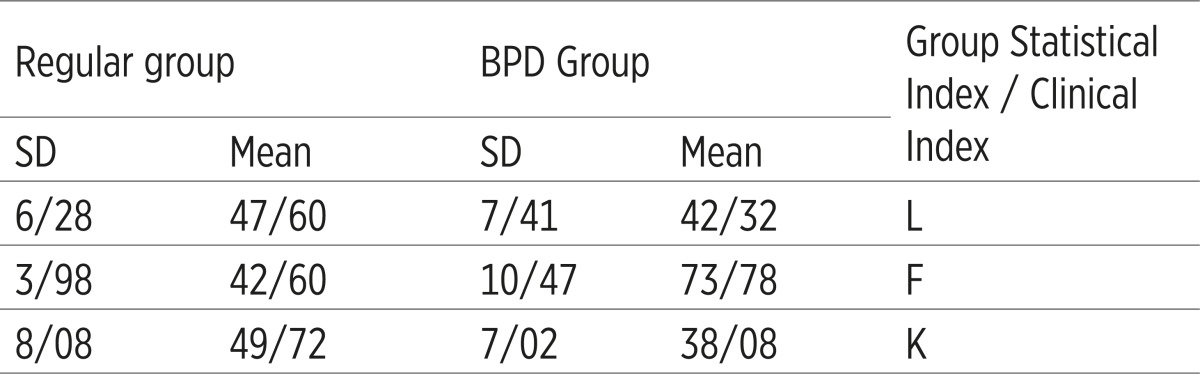 |
Table 2.
Mean and Standard Deviation of Two Groups of Women with BPD and Regular in Clinical Indexes of MMPI-2 test
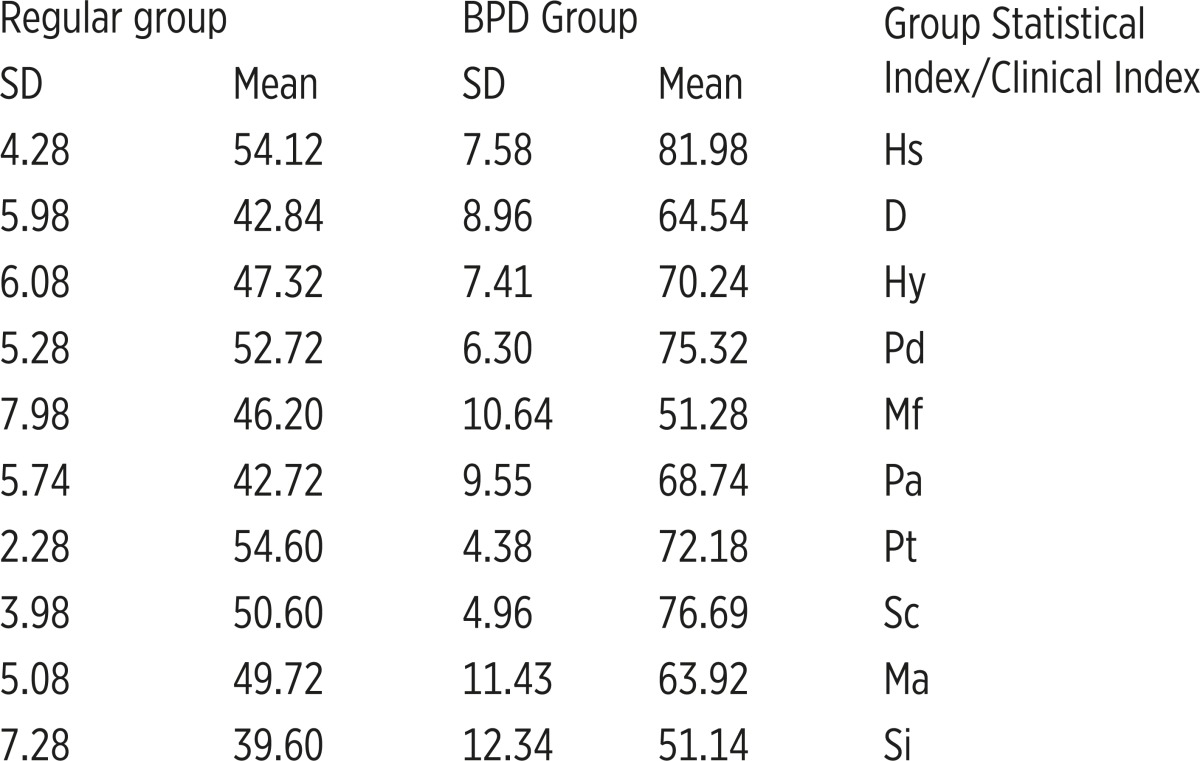 |
Based on these results, the group of individuals with BPD has a higher average as compared with the Regular group in all clinical indexes of MMPI-2 test.
The data of Table 3 shows the results of Multivariate analysis of variance (MANOVA) on differences of two groups of women with BPD and Ordinary Women in validity indexes of MMPI-2 test.
Table 3.
The results of the Multivariate analysis of variance (MANOVA), the Difference of Two Groups of Women with the Disorder of BPD and Regular Women in Validity Indexes of MMPI-2 test
 |
According to these results, there is a significant difference at the level of P<0/100 in validity of MMPI-2 test. The rate of square of ETA is 89 percent. That is to say, that 89 difference between the two groups are explained by validity indexes of MMPI-2 test.
The data of Table 4 shows the results of Multivariable Variance Analysis Test (MANOVA) on difference between the two groups of women with BPD and regular women in validity indexes of (K, F, L) of MMPI-2 test. Based on these results, there is a significant difference at the level of p<0/001 between the two groups in validity indexes of (K, F, L) of MMPI-2 test.
Table 4.
The results of Multivariate analysis of variance (MANOVA) of difference between two groups of women with BPD and regular in validity index of MMPI-2 test
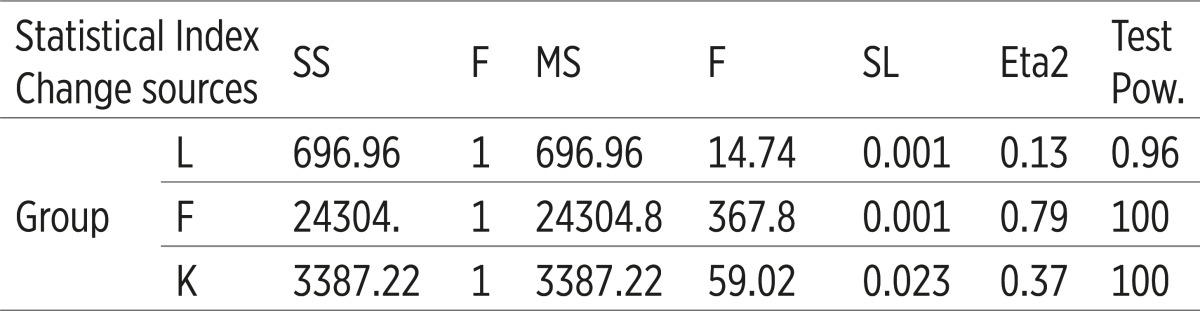 |
Based on these results, there is a significant difference at the level of p<0/001 in validity indexes of MMPI-2 test. The rate of square of ETA is 93 percent. That means 93 percent difference between the two groups is explained by clinical indexes of MMPI-2 test.
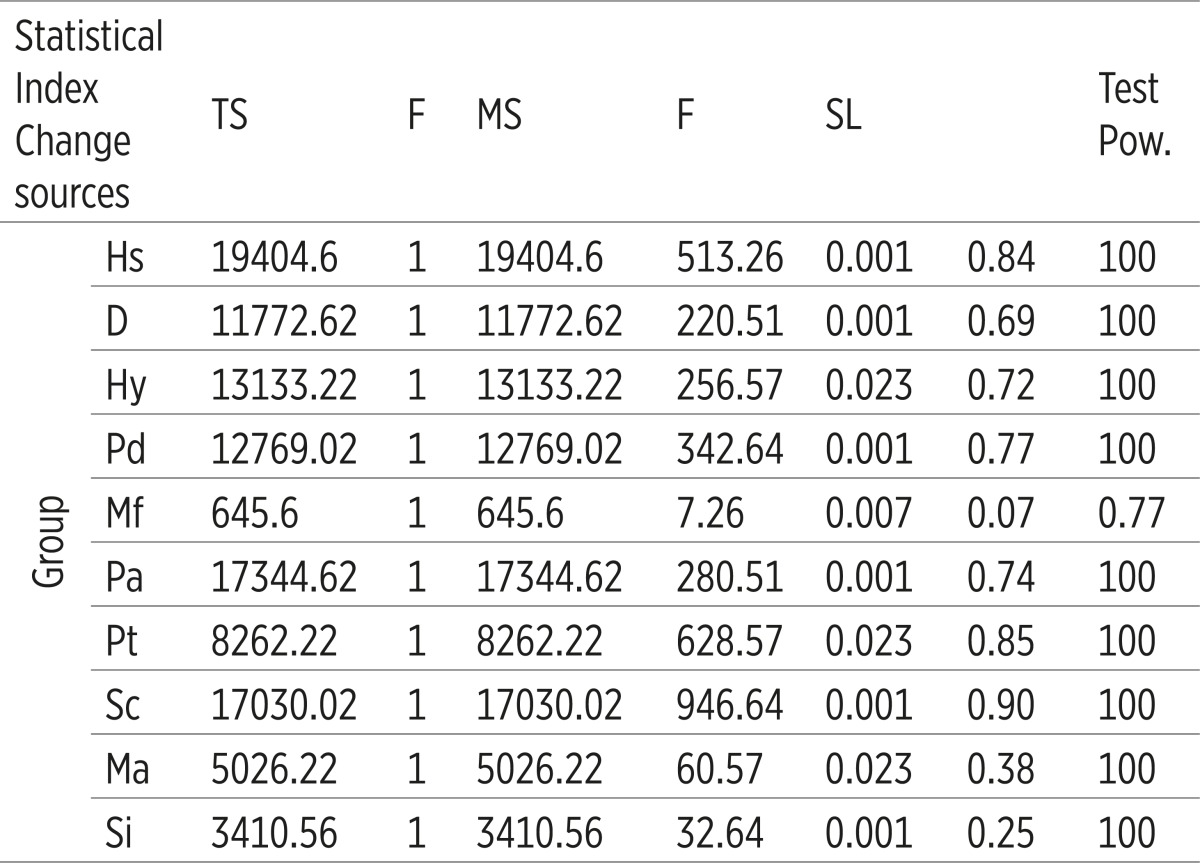
The data of Table 6 on the results of Multivariate analysis of variance (MANOVA) shows the difference of two groups of women with BPD and regular women in clinical indexes of MMPI-2 test. According to these results, there is a significant difference at the level of P<0/001 between the two groups in clinical indexes (Hs, D, Hy, Pd, Mf, Pa, Pt, Sc, Ma, Si) of MMPI-2 test, there is a significant difference at the level of p<0/001.
Table 6.
The results of Multivariate analysis of variance (MANOVA) on differences of two groups of women afflicted with BPD and Regular Women in clinical indexes of MMPI-2 test
 |
4. DISCUSSION AND CONCLUSION
The present research was conducted with an aim to compare the personality profile of women with BPD and regular and their performance in MMPI-2 test. The results of the research showed that individuals with BPD in MMPI-2 test and its validity and clinical indexes had a significant difference. The results of this research shows that patients with BPD are experiencing corresponding and specific distress in MMPI-2.
As it is seen in the results of Table 4, having mixed-up status (distress) of the scale F of the validity scales in particular with the average of 73/78 and standard deviation of 10/78 is one of the diagnostic indexes on women with BPD and on the other hands, the corresponding distresses of clinical scales of Hs, Hy, Pd, Pt, Sc is considered as other diagnostic symptoms of this disorder. With regard to the evaluating factors of these scales and clinical diagnostic concepts based on DSMIV-TR, there is also a noticeable overlapping.
Another point, which should be mentioned on this topic, is the scale difference of Pt and Sc with higher distress of SC as compared with Pt, which in the interpretation of MMPI-2 is mentioned as one of the indexes of chronicity (13). As it is shown in the Figure 1, the obtained corresponding distress is one of the apparent diagnostic symptoms in the results of this research on women with BPD. The results of this research are comparable with the findings of Marnat 2003 on distresses of the Sc scale on people with BPD.
Figure 1.

The Psychological (mental) profile of MMPI-2 of women afflicted with BPD.
Also the results of the Table 3 on mental profile of women with BPD in validity scales in comparison with regular women shows a difference and it can be concluded with 99 percent validity that the mental profile of those with BPD in validity scales is different from regular people. Also Table 5 which studies the results of Multivariate analysis of variance (MANOVA) of clinical indexes of MMPI-2 test in women with BPD and regular women shows a significant difference at clinical scale with a 99% validity.
Table 5.
The results of Multivariate Analysis of Variance (MANOVA) shows the difference between the two groups of women with BPD and Regular in clinical indexes of MMPI-2 test
 |
The noticeable distress of clinical scales of MMPI-2 tests in BPD patients is comparable with the studies of Malayeri and Kaveyani (2008) (12) in the study of dimensions of personality of BPD patients based on questionnaires of Cloninger Temperament and Character Inventory TCI-125.
Their findings emphasize on high scores of new-seeking, vulnerability, self-orientation, self-projection and also low level of collaboration in the patients with BPD. Considering the analysis of distress of these patients in MMPI-2 test, it is comparable.
The question which this project is looking for that is to identify the profile of female patients with BPD. However many challenges in identification and diagnostic scales have been put forth by DSMIV-TR, as Joel Paris (2008) (15) puts: Despite the fact in recent 10 years, knowledge in respect of this disorder has been increased but research on the validity of DSM scales are very slow. It is hoped that DSMV to be noticed basically. It seems if the profile of these types of patients could be identified, it will be possible to take effective steps to know it faster and take action to treat it.
On one side, the lack of existing sources in connection with the mental profiles of these patients in prevailing tests such as MMPI-2 encourages researcher to make more studies on the domain of psychological tests and diagnostic profile of BPD. One of the limits of this study was the shortage of creditable sources in the area of measuring BPD (16, 17, 18, 19).
Conflict of interest
None declared.
REFERENCES
- 1.Kaplan H, Sadock BJ. Comprehensive textbook of psychiatry VA. Williams and Willkins Company; 2009. pp. 560–564. [Google Scholar]
- 2.Kaplan H, Sadock BJ. Comprehensive textbook of psychiatry VA. Williams and Willkins Company; 2005. pp. 560–564. [Google Scholar]
- 3.Prochaska J, Norcross J. In: Systems of Psychotherapy. Yahya Seyed Mohammadi., translator. Ravan Publications; 2008. p. 108. [Google Scholar]
- 4.Bouchard S, Sabourin S. Borderline personality disorder and couple dysfunctions. Current psychiatry reports. 2009;11:55–62. doi: 10.1007/s11920-009-0009-x. [DOI] [PubMed] [Google Scholar]
- 5.Farrell JM, Shaw IA, Webber MA. A schema focused approach to group psychotherapy for outpatients with borderline personality disorder: a randomized controlled trial. Journal of Behavior Therapy. 2009;40:317–328. doi: 10.1016/j.jbtep.2009.01.002. [DOI] [PubMed] [Google Scholar]
- 6.Farrell JM, Shaw IA, Webber MA. A schema focused approach to group psychotherapy for outpatients with borderline personality disorder: a randomized controlled trial. Journal of Behavior Therapy. 2009;40:317–328. doi: 10.1016/j.jbtep.2009.01.002. [DOI] [PubMed] [Google Scholar]
- 7.Ryle A, editor. Cognitive Analytic Therapy: Developments in theory and Practice. New York: Wiley; 2005. [Google Scholar]
- 8.Farrell JM, Shaw IA, Webber MA. A schema focused approach to group psychotherapy for outpatients with borderline personality disorder: a randomized controlled trial. Journal of Behavior Therapy. 2009;40:317–328. doi: 10.1016/j.jbtep.2009.01.002. [DOI] [PubMed] [Google Scholar]
- 9.Eftekhar M, Shabani A. BPD is not a Bipolar Disorder. Journal of Psychiatry and Clinical Psychology. 2009;15(158):147–152. [Google Scholar]
- 10.New AS, Triebwasser G, Charney DS. The case for shifting border line personality disorder to Axis I. Biological Psychiatry. 2008;64:653–659. doi: 10.1016/j.biopsych.2008.04.020. [DOI] [PubMed] [Google Scholar]
- 11.Mohammad Zadeh, Ali, Goudarzi, Mohammad Ali, Taghavi Seyed Mohammmad Reza, Molazadeh Javad. A Study of the Structure of Factors, Reliability, Validity and Normative Status STB in Students of Shiraz University. Quarterly for Mental Health, Year Seven. 2007;27-28:75–89. [Google Scholar]
- 12.Ali Malayeri, Nooshin Kaviyani, Hossein Assadi, Seyed Mohammad, Farid, Hossein, Farhad Evaluation of Dimensions of Personality based on Questionnaire of Sezesht and Menesh Klou Ninger TCI-125 in Patients with BPD. Journal of Faculty of Medicine, Tehran University of Medical Science. 2008;66(9):622–638. [Google Scholar]
- 13.Marnat Gary Grath. In: A Guidebook for Measuring the Validity of Test, edited 2003. Dr. Hasan Pasha Sharifi, Dr. Mohammad Reza Nikhou., translators. Vol. 1. Roshd and Sokhan Publications; 2008. p. 419. [Google Scholar]
- 14.Graham JR, Lilly RS. Psychological Testing. Englewood Cliffs. Ng: Prentice–Hall; 1984. [Google Scholar]
- 15.Paris Joel. Treatment of Borderline Personality Disorder. A guide to evidence–Based Practice. The Guilford Press; 2008. p. 219. [Google Scholar]
- 16.Kernberg OE. Borderline conditions and pathological narcissism. New York: Jason Aronson; 1975. [Google Scholar]
- 17.Lubin B, Larsen RM, Matarazzo JD, Seever M. Psychological test usage patterns in fine professional settling. American Psychologist. 1985;40:857–861. [Google Scholar]
- 18.Sadock B, Sadock VA. Synopsis of Psychiatry Behavioural Sciences. 10th ed 2007. [Google Scholar]
- 19.Young JE, Gluhoski VI. Scheme-Focused Diagnosis for Personality Disorder. In: F.W. Kaslow., editor. Hand Book of Relational Diagnosis and Dysfunctional Family Patterns. New York: Wiley; 1996. pp. 300–321. [Google Scholar]