

Abstract
Tested a theoretical model on the effects of social role identity, illness intrusion, and competence on psychological well-being among 109 low-income Latinas with arthritis. All six roles studied were rated as highly important identities. Sex-role nontraditionalism was associated with less importance of the homemaker, mother, and grandmother roles. Negative affect increased as a function of intrusions into valued identities. Having important role identities contributed to feelings of competence (i.e., self-esteem and self-efficacy), which in turn, contributed to psychological well-being. Competence also mediated the effects of pain, identity, and illness intrusions on psychological well-being. Results suggest competence processes play an important role in well-being.
Keywords: Latina/Hispanic women, arthritis, social role identities, competence, self-esteem, psychological adjustment
Although the majority of people living in poverty are white—about two thirds—women of color are disproportionately represented among the poor (U.S. Department of Commerce, Bureau of the Census, 1992). Single, “head-of-household” women face a greater risk of being poor than married women. In 1989, about half of households headed by Latinas (47.5%) and African-American women (46.5%) were poor, compared to one quarter of white female-headed households (25.4%) (Schmittroth, 1991). Despite these statistics, there is almost no psychosocial research on women of color with chronic diseases such as arthritis. Arthritis (which includes over 100 types of rheumatic diseases) is a chronic, disabling condition that affects more than 37 million Americans (NIAMS, 1993). Although adequate prevalence data on women of color are not available (Padilla & Perez, 1995), arthritis is the most prevalent chronic condition in women and individuals with family incomes of less than $20,000, and the leading cause of activity restriction among women (Callahan, 1996; U.S. Department of Health and Human Services, 1993).
Given the scarcity of research on Latinas facing both chronic illness and poverty, studies that help develop theoretical models and identify cultural strengths in coping with these multiple stressors are especially needed (Abraído-Lanza, Guier, & Revenson, 1996). With its emphasis on empowerment and diversity, community psychology should be at the forefront of this research endeavor. To that end, this study tests a theoretical model of the impact of arthritis on roles, outlining how culturally valued social role identities contribute to self-esteem, a sense of competence, and psychological well-being. The sample consisted of Latinas (half of whom were Puerto Rican) with limited socioeconomic status (SES) resources.
Latino Culture and Role Identities
Culture and socialization practices determine, to some extent, the value placed on social role identities. Latinos' identities are largely entwined in family roles. As Landrine (1992) noted, in Anglo cultures, persons are independent entities, separate and prior to community and family. In contrast, in Latino and other ethnic minority groups (e.g., African American and Asian American), family and community are primary over individuals. “Social-role selves do not have rights (to privacy, autonomy, and self-determination), but duties and obligations to perform their role well for the larger units … Consequently, the failure to perform one's role as wife, mother, father, husband, daughter, or son is a failure to be a person at all: Role failure or violation is the loss of the self” (p. 408; original italics removed).
As Latino culture prescribes traditional sex-role beliefs (Canino et al., 1987; Vazquez-Nuttall, Romero-Garcia, & De Leon, 1987), roles such as being a mother take particular prominence in how women define themselves (Hubbell, 1993; Sánchez-Ayéndez, 1988). Therefore, the inability to carry out gender-related role activities may be especially stressful. In a study of Mexican immigrant women, respondents who felt they would be unable to fulfill their roles as wives in their new unfamiliar environments were more likely to experience depression than women who did not express this belief (Salgado de Snyder, 1987).
Less research examines the contribution of nontraditional roles, such as paid work, to Latinas' identities and psychological well-being. Krause and Markides (1985) found that among Mexican American married women with traditional attitudes, work was associated with decreased positive affect; conversely, among those with nontraditional orientations, work was related to increased positive affect. Therefore, the effects of illness on work—as well as family roles—may be especially relevant for Latinas with arthritis.
Conceptual Model: Social Roles, Self-Esteem, Competence, and the Identity-Relevant Hypothesis
Identity theory suggests that by interfering with valued or important roles, rheumatic diseases threaten the self-concept, which ultimately leads to psychological distress. Social roles form the basis of the self-concept (Pearlin, 1983; Tajfel, 1981), but some roles are more central to identity than others (McCall & Simmons, 1966; Stryker & Serpe, 1982; Thoits, 1991). Relative to less important roles, valued identities have a stronger impact on self-esteem (Rosenberg, 1979), and individuals gain a sense of competence by performing these roles (White, 1987). Therefore, as Thoits (1991) and others (Brown & McGill, 1989; Oatley & Bolton, 1985) argue, events that disrupt important role identities, or “identity-relevant” stressful events, should be more detrimental to psychological well-being than “identity-irrelevant” events. Moreover, a decreased sense of mastery and self-esteem should mediate the effects of disrupted social roles on psychological well-being (Pearlin, 1983; Pearlin, Lieberman, Menaghan, & Mullan, 1981).
Because of pain and disability, arthritis interferes with homemaking (Allaire, 1992; Reisine, Goodenow, & Grady, 1987) and other roles, including paid work, religious activities, recreation, and social relations (e.g., Katz, 1995). The high rates of depression observed among arthritis samples may be due, in part, to the inability to perform valued activities (Katz & Yelin, 1994). Studies of people with rheumatoid arthritis report that satisfaction with the ability to perform important role activities predicts psychological adjustment (Blalock et al., 1992), that illness intrusions into these activities relate to depressive symptoms (Devins et al., 1992), and that a sense of competence mediates the relationship between arthritis illness stressors and psychological adjustment (Smith, Dobbins, & Wall-ston, 1991).
These theoretical models and findings suggest several pathways through which arthritis-induced role intrusions and social role identities contribute to psychological well-being. Figure 1 illustrates this conceptual model. It should be noted that identity processes occur against a cultural “backdrop.” As the value placed on roles reflects cultural norms, acculturation and nontraditional attitudes should relate to decreased importance of traditional roles (such as homemaker).
Fig. 1.
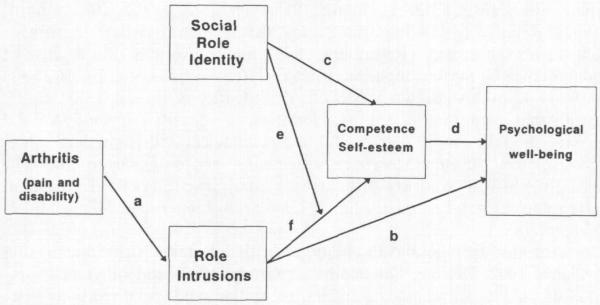
Conceptual model of the relationships between arthritis stressors, social role identities, role intrusions, competence, and psychological well-being.
Figure 1 shows that arthritis results in pain and disability, which may intrude upon the ability to perform social roles (Path a), and affect psychological adjustment (Path b). As important roles provide people with a sense of identity, competence, and self-esteem (Path c), which contribute to psychological well-being (Path d), intrusions that affect important roles should have a larger impact on psychological well-being than intrusions into less important identities. Thus, role importance moderates the effect of illness intrusion on psychological well-being (Path e) in part, by affecting self-esteem and a sense of competence (Path f). The purpose of this study was to test this model and its principal hypotheses.
METHOD
Procedure
Respondents were recruited from the Rheumatic Disease Clinic, a specialty clinic within the Ambulatory Care Center of the Hospital for Special Surgery in New York City, which serves a large Latino population. Eligibility criteria were age 18 years or older, Hispanic ethnicity (defined as individuals of Puerto Rican, Mexican, Cuban, South or Central American, or other Spanish culture or origin; Marín & Marín, 1991); and diagnosis of rheumatic disease. Respondents were recruited while waiting for their clinic appointments. The majority of respondents were approached by the investigator about participating in the study; a small number of respondents were referred to the study by their physicians. The study's purpose and procedures were explained using standard informed consent procedures. All patients who agreed to participate in the study were given a copy of the consent form to keep.
A total of 127 women were asked to participate in the study. Only nine women (7%) declined participation. Of the 118 women who agreed to participate in the study, nine interviews could not be scheduled for various reasons (e.g., schedule conflicts). Therefore, a total of 109 women participated in the study. This sample size yields sufficient statistical power (.80) to detect a medium effect size with an alpha level of .05, and eight independent variables in a regression equation (Cohen, 1992).
Data were collected by a structured face-to-face interview. Respondents were given the option of completing the interview in Spanish or English, either in their homes or at the hospital clinic. The majority (84.4%) of interviews were conducted in Spanish; most (70.6%) took place in respondents' homes. The average interview lasted 80 minutes. Respondents were paid $25 for their participation.
Sample Characteristics
Table I presents the sample characteristics of the 109 participants. About half (54.1%) of the sample had rheumatoid arthritis (RA). The average respondent had been ill for almost 14 years. Five respondents (4.6%) were confined mostly to a wheelchair or bed.
Table I.
Sample Characteristics (N = 109)
| n | % | M | SD | |
|---|---|---|---|---|
| Diagnosisa | ||||
| Rheumatoid arthritis | 59 | 54.1 | ||
| Lupus | 17 | 15.6 | ||
| Osteoarthritis | 17 | 15.6 | ||
| Scleroderma | 2 | 1.8 | ||
| Arteritis | 2 | 1.8 | ||
| Osteoporosis | 1 | 0.9 | ||
| Fibromyalgia | 1 | 0.9 | ||
| More than one type | 10 | 9.2 | ||
| Years of disease duration | 13.9 | 10.6 | ||
| Place of birth | ||||
| Puerto Rico | 45 | 41.9 | ||
| United Statesb | 13 | 11.9 | ||
| Dominican Republic | 13 | 11.9 | ||
| Cuba | 7 | 6.4 | ||
| Central America: | ||||
| Guatemala | 3 | 2.8 | ||
| El Salvador | 2 | 1.8 | ||
| South America: | ||||
| Columbia | 14 | 12.8 | ||
| Ecuador | 7 | 6.4 | ||
| Peru | 4 | 3.7 | ||
| Uruguay | 1 | 0.9 | ||
| Years residing in U.S.c | 27.9 | 10.8 | ||
| Age | 50.6 | 14.1 | ||
| Years of education | 8.9 | 4.0 | ||
| Employment status | ||||
| Disabled | 53 | 48.6 | ||
| Homemaker | 42 | 38.5 | ||
| Working part-time | 7 | 6.4 | ||
| Working full-time | 2 | 1.8 | ||
| Currently unemployed (i.e., seeking work) | 2 | 1.8 | ||
| Household income (per year) | ||||
| < $10,000 | 80 | 73.4 | ||
| $10,000–$19,999 | 17 | 15.6 | ||
| $20,000 or more | 11 | 10.1 | ||
| Marital status | ||||
| Married | 21 | 19.3 | ||
| Live with partner | 6 | 5.5 | ||
| Divorced | 34 | 31.2 | ||
| Separated | 26 | 23.9 | ||
| Widowed | 13 | 11.9 | ||
| Single (never married) | 9 | 8.3 | ||
| Have at least one child | 95 | 87.2 | ||
| No. of children | 2.4 | 1.8 | ||
| Have at least one child (age in years) | ||||
| 0–5 | 5 | 4.6 | ||
| 6–12 | 12 | 11.0 | ||
| 13–19 | 25 | 22.9 | ||
| 20 or more | 77 | 70.6 | ||
| No. of grandchildren | 3.7 | 5.9 | ||
| Have at least one grandchild | 57 | 52.3 | ||
| Have at least one grandchild (age in years) | ||||
| 0–5 | 40 | 36.7 | ||
| 6–12 | 33 | 30.3 | ||
| 13–19 | 22 | 20.2 | ||
| 20 or more | 15 | 13.8 |
Diagnosis data were self-reported.
Family country of origin for U.S.-born respondents: Puerto Rico (n = 11); Dominican Republic (n = 1); Ecuador (n = 1).
Years in U.S. for all respondents.
Most respondents (88%) were foreign-born. Half of the sample (51.4%) was Puerto Rican, most of whom were born on the island. The average respondent had been residing in the U.S. for 27.9 years, with a range of less than 1 year to 51 years. The average respondent was middle-aged (M = 50.6; range = 19–86 years), and had 9 years of education. Most participants were either currently unemployed due to disability (48.6%) or were homemakers (38.5%). Most had a household income of less than $10,000 per year (73.4%). Few respondents lived alone (21.1%); and most were not married, being either separated, divorced, or widowed. Most (87..2%) were mothers, and had at least one child over 20 years of age. Half of the respondents (52.3%) were grandmothers.
Measures
Instruments were administered in either Spanish or English. A double translation technique using two iterations with independent translators was employed, as recommended by Marín and Marín (1991).3
Arthritis Characteristics
Arthritis was operationalized by pain and functional disability, two commonly used indices of disease severity in arthritis research. Pain was measured by a 6-item instrument used in the Medical Outcome Study to assess frequency and intensity of pain over the past 4 weeks (Sherbourne, 1992) (e.g., "During the past 4 weeks, how often have you had pain?"; "How long did it usually last?"). The six items are summed, yielding scores that may range from 4 to 43, with high scores indicating more severe pain. The mean score in this study was 34.57 (SD = 6.83), indicating that the average respondent experienced relatively high levels of pain. Cronbach's α = .79 for the scale.
Disability was measured by the functional disability subscale of the Health Assessment Questionnaire (HAQ; Fries, Spitz, Kraines, & Holman, 1980). The HAQ shows excellent reliability and validity among arthritis populations (Liang, Larson, Cullen, & Schwartz, 1985), and adequate agreement with physician-rated disease status (Goodenow, Reisine, & Grady, 1990). It is composed of 24 items assessing mobility and ability to perform activities of daily living (e.g., eating, dressing), rated on a 4-point scale from 0 (without any difficulty) to 3 (unable to do). The mean is calculated to obtain a disability score. In this study, M = 1.85 (SD = 0.61), indicating that the average respondent performed activities with “much difficulty,” or a moderately high level of disability. The internal consistency reliability for the scale was .80.
Social Role Identities
Six role identities were selected for this study as they are common roles by which Latinas define themselves: homemaker, parent, grandparent, spouse, worker, and friend. The importance of each role and the degree to which illness interfered with role performance were measured by a number of instruments.
Role Identity Importance
The Identity Subscale of Luhtanen and Crocker's (1992) Collective Self-Esteem Scale assessed the importance of each role to the self-concept. The scale shows good psychometric properties in studies of Latinos (Ethier & Deaux, 1990, 1994). Respondents indicated the extent to which they agree with four statements for each role (e.g., “Overall, being a [homemaker, mother, grandmother, wife, worker, friend] has very much to do with how I feel about myself”). Although two items in the original scale are reverse-keyed, to avoid confusion, all statements were worded so that agreement indicated importance. For each role, a role identity score was obtained by averaging the four items. Internal consistency reliabilities for each role identity were: homemaker, .95; mother, .95; grandmother, .98; wife, .96; worker, .77; friend, .98. In addition, an average role identity score was calculated as the mean of all items.
Role Intrusion
Items assessing illness intrusion resembled those used in other studies of RA (Devins, Edworthy, Guthrie, & Martin, 1992). Respondents were asked, “How much has your illness affected or interfered with each of these areas of your life?,” and rated each relevant role (house-hold chores, parenting, grandparenting, marriage, work, friendships) on an 11-point scale from 0 (not at all) to 10 (extremely). A global illness intrusion score, averaging across all relevant roles, was calculated for each respondent.
Predictors of Role Importance
Sex-Role Nontraditionalism
The Index of Sex Role Orientation (ISRO; Dreyer, Woods, & James, 1981) assessed gender-role orientations. The ISRO shows adequate reliability and the ability to discriminate between feminist and traditional political/community groups (Dreyer et al., 1981). The scale's 16 items tap attitudes about women, work, childrearing, and the division of household labor. Scores are summed in the direction of nontraditionalism, yielding a possible range of 16 to 80. In this study, Cronbach's α = .82 (M = 53.41, SD = 9.89), indicating the average respondent held sex-role attitudes that were neutral-to-moderately nontraditional.
Acculturation
Acculturation was measured by Marín, Sabogal, Marín, Otero-Sabogal, and Pérez-Stable's (1987) 4-item scale, which assesses language use (e.g., “In which language do you usually think?”) on a scale ranging from 1 (only Spanish) to 5 (only English). Responses are summed; high scores indicate greater acculturation. The measure has been validated with a variety of Hispanic groups, demonstrates high reliability, and correlates with criteria such as length of residence in the U.S. (Marín et al., 1987). In this study, Cronbach's α = .89 (M = 7.47, SD = 4.27), indicating a relatively low level of acculturation. Length of residence in the U.S. was related to acculturation (r = .32, p < .001) but not to sex-role nontraditionalism (r = −.14, ns). The correlation between sex-role nontraditionalism and acculturation was .54 (p < .01).
Mediating Variables: Sense of Competence
Various measures of self-esteem and self-efficacy were used to assess the sense of competence. Self-esteem was measured by Rosenberg's (1965) 10-item scale. Scores range from 1 to 50; high scores indicate positive self-esteem. The scale has been used with RA samples (e.g., Fitzpatrick et al., 1988; Revenson & Felton, 1989) and Hispanics (e.g., Van Meek, 1992). In this study, the mean was 38.75 (SD = 6.61) and Cronbach's ω = .81.
Illness-Specific Self-Esteem was assessed by 6-itern scale taken from Felton and Revenson's (1984) study of people with chronic illnesses. Respondents indicate their extent of agreement with statements about illness-related self-esteem (e.g. “Despite my illness I feel worthy as a human being,” “My health makes me feel inadequate,” “Frail health makes one less of a person”), on a 5-point scale from (strongly agree) to (strongly disagree). Responses are summed; high scores represent high illness-specific self-esteem. In this study, M = 19.07 (SD = 4.95) and Cronbach's α = .75.
Self-Efficacy
Competence was also operationalized as general feelings of self-efficacy, or beliefs about performance capabilities. A self-efficacy measure for people with arthritis developed by Lorig, Chastain, Ung, Shoor, and Holman (1989) was used. The scale contains three subscales, two of which were used in the present study. The first subscale (6 items) measures the extent to which the respondent believes she is able to control pain and continue daily tasks (e.g., “How certain are you that you can continue most of your daily activities?”). The second subscale (7 items) assesses control over other symptoms such as fatigue (e.g., “How certain are you that you can regulate your activity so as to be active without aggravating your arthritis?”). The response format consists of a 10-point rating scale, with endpoints labeled very uncertain and very certain. Items within each subscale are summed; high scores reflect high self-efficacy. As the two subscales were highly correlated in this study (r = .79), they were combined to form a single self-efficacy score. Scores could range from 13 to 130. In this sample, the mean was 76.38 (SD = 29.17) and Cronbach's α = .93. Correlations between self-efficacy and the two self-esteem measures were .36 for global self-esteem, and .35 for illness-specific self-esteem (both ps < .0001). The correlation between global and illness-specific self-esteem was .67, p < .01. Although the correlation between the two esteem measures was fairly high, the overall pattern suggests that the three scales should be used separately to measure the construct of competence.
Psychological Well-Being
Psychological well-being and ill-being have different dimensions and correlates (Diener, 1984). Various measures were used to assess psychological well-being.
Depressive symptoms were measured with the Center for Epidemiologic Studies Depression scale (CES-D; Radloff, 1977), a 20-item measure that assesses symptoms of depression during the previous week. Items are summed yielding a possible range of 0 to 60; high scores indicate greater depression. The scale has been used extensively with arthritis samples (e.g., Goodenow et al., 1990; Revenson et al., 1991) and is highly reliable for this population (Blalock, DeVellis, Brown, & Wallston, 1989). Both the English and Spanish versions have been used with Hispanic samples with good reliability and validity (e.g., Salgado de Snyder, 1987; Stroup-Benham, Lawrence, & Treviño, 1992).
Psychological well-being was assessed with the Index of Affect, which was used in two large-scale national surveys (Andrews & Withey, 1976; Campbell, Converse, & Rogers, 1976). This 8-item semantic differential scale assesses feelings about life as a whole (e.g., boring-interesting, enjoyable-miserable) using a 7-point response format. Items are summed; high scores indicate positive affect. The scale correlates with other measures of well-being and shows good psychometric properties (Larsen, Diener, & Emmons, 1985).
The Positive and Negative Affect Scale (PANAS; Watson, Clark, & Tellegen, 1988) is a 20-item scale. Respondents rate how often they experienced 10 positive (e.g., “excited”) and 10 negative (e.g., “nervous”) feelings over the past week. Items within each scale are summed, with higher scores indicating greater positive or negative affect.
A confirmatory factor analysis on all four well-being measures revealed that a two-factor model of psychological well-being best fit the data, χ2(1, N = 109) = 0.50, p = .49; Goodness of Fit index = .98. The first factor could be described as a general positive affect factor, the second as negative affect. Based on this confirmatory factor analysis, two measures of psychological well-being were created. Positive Affect comprised the summed score of the Index of Affect and PANAS positive items, yielding scores with a possible range of 18 to 106. The mean of the sample was 69.00 (SD = 17.01). Negative Affect consists of the sum of the CES-D and PANAS negative affect items, yielding scores that could range from 10 to 110. The mean score was 45.32 (SD = 20.93). The two factors are correlated −.59 (p < .0001), suggesting that they are related, but tapping somewhat different dimensions of well-being.
RESULTS
It should be noted that, despite recognition of the heterogeneity of Latinas (Bernal & Enchautegui-de-Jesús, 1994), separate analyses by subgroups (e.g., Puerto Ricans, Cubans, etc.) could not be conducted due to sample size and statistical power limitations.
Descriptive Data
Role Identity and Illness Intrusion
Of the six roles studied (homemaker, mother, grandmother, wife, paid worker, and friend), all women in the sample (N = 109) held the home-maker and friend roles. Ninety-five women (87.2%) were mothers, 57 (52.3%) were grandmothers, and 27 (24.8%) were wives. Nine respondents (8.3%) who held the paid work role were either employed full-time (n = 2) or part-time (n = 7). Two others were currently seeking employment.
Of these six roles, the average number of roles held by respondents was 3.37 (SD = 0.69). Sixty-three women in the sample (57.8%) held three roles, and 35 women (32.1%) held four roles. A simple count of the number of roles held by respondents was not related to either positive (r = −.03) or negative affect (r = .11), although these correlations may be affected by low variance in the number of roles respondents held. Data described below suggest that it is not the number but quality (i.e., illness intrusion) and importance of roles to the self-concept that contributes to psychological well-being.
Table II presents descriptive statistics for the role identity and illness intrusion measures. All six roles received high ratings, indicating that on average, the roles chosen for study were central to women's identities. Although the friend role received a relatively high rating, many women expressed a general belief that good friends are “few and far between,” and stated that they had only one or two good friends. Table II also shows that the homemaker and work roles were most severely affected by rheumatic diseases.
Table II.
Mean Role Identity Importance and Illness Intrusion Ratings
| Role identitya |
Illness intrusionb |
||||
|---|---|---|---|---|---|
| Role | n | M | SD | M | SD |
| Homemaker | 109 | 5.95 | 1.40 | 7.21 | 2.66 |
| Mother | 95 | 6.83 | 0.45 | 3.40 | 4.02 |
| Grandmother | 57 | 6.71 | 0.79 | 3.30 | 4.07 |
| Wife | 27 | 6.66 | 0.85 | 4.48 | 3.72 |
| Worker | 9 | 6.19 | 0.65 | 5.50 | 2.95 |
| Friend | 109 | 5.92 | 1.54 | 3.43 | 3.95 |
Four-item scale; total scores range from 1 to 7.
Single-item scale; Likert-type responses range from 0 to 10 (10 = high intrusion).
Test of Model and Study Hypotheses
It was expected that sex-role orientation and acculturation relate to role identity importance. Table III shows the correlations of sex-role orientation, acculturation, and years residing in the U.S. with role identities. Sex-role orientation correlated with three of the six role identities: home-maker, mother, and grandmother. Nontraditional sex-role attitudes were related to decreased importance of these roles. Acculturation was correlated negatively with importance of the mother role. Neither sex-role orientation nor acculturation was correlated with the work, wife, or friend roles. Sex-role orientation was not related to either positive or negative affect (rs = .00 and −.07, ns, respectively), nor was acculturation (rs = −.13 and .09, ns).
Table III.
Correlations Among Sex-Role Orientation Nontraditionalism, Acculturation, Years in U.S., and Role Identity
| Role identity | Sex-role orientationa | Aculturation | Years in U.S. |
|---|---|---|---|
| Homemaker | −.28c | ` −.17 | .02 |
| Mother | −.33d | −.50d | −.12 |
| Grandmother | −.28c | −.05 | .05 |
| Wife | −.23 | −.16 | .03 |
| Worker | −.03 | −.41 | −.63 |
| Friend | .10 | .10 | −.10 |
High scores reflect a nontraditional sex-role orientation.
p < .05.
p < .01.
p < .001.
The principal paths in the conceptual model concern the effects of role identities and illness intrusions on psychological well-being (positive and negative affect). The model was tested with path analysis, using reduced form equations as outlined by Cohen and Cohen (1983). The procedure involves a series of hierarchical regression equations, in which each variable enters in order of causal priority. Interactions are tested with multiplicative (product) terms. Mediating effects are tested by examining indirect effects. At the final step of the equations, regression coefficients represent the direct effects of each predictor variable. An indirect effect of a variable via a specific mediator is calculated as the difference in the variable's coefficient before and after the mediator enters the equation (Cohen & Cohen, 1983, pp. 360–361).
Separate regression equations were computed for positive and negative affect as criterion variables. In both equations, pain and disability were entered as a set in the first step. Illness intrusion and role identity scores (averaged across roles) were entered as a set in the second step. An interaction term composed of the product of the (averaged) illness intrusion and role identity scores was entered on the third step.4 A significant interaction term would indicate a moderator effect. The three measures of competence (self-esteem, illness self-esteem, and self-efficacy) were entered as a set in the final step to examine whether competence mediates the effects of identity and intrusions on psychological well-being. Mediation effects of competence are shown by changes (differences) in regression coefficients of other variables at the final step, when competence variables enter the equation.
These equations yield path coefficients from predictor (pain, disability, illness intrusion, identity) and mediating variables to criterion variables (positive and negative affect). To complete the model, paths from predictor to mediating variables were calculated (see Baron & Kenny, 1986). To estimate these effects, the hierarchical analyses described above were repeated using the three measures of competence as outcomes.
Table IV presents the intercorrelation of variables in the path analyses. Table V shows the results of regression analyses predicting positive and negative affect, and Table VI presents analyses for competence variables. Figure 2 shows direct paths obtained from the final steps in Tables V and VI; and Figure 3 indirect effects calculated from the final step of Table V Only significant paths are illustrated to simplify the diagrams.
Table IV.
Intercorrelations Among Variables Used to Test the Conceptual Model
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Pain | — | |||||||
| 2. Disability | .54c | — | ||||||
| 3. Intrusion | .36c | .42c | — | |||||
| 4. Identity | .04 | .10 | .04 | — | ||||
| Proposed mediators | ||||||||
| 5. Self-esteem | −.16 | −.16 | −.34c | .26b | — | |||
| 6. Illness self-esteem | −.28b | −.29b | −.47c | .07 | .67c | — | ||
| 7. Self-efficacy | −.33c | −.21a | −.33c | .24b | .36c | .35c | — | |
| Psychological well-being | ||||||||
| 8. Positive affect | −.23a | −.09 | −.23a | .35c | .59c | .45c | .55c | — |
| 9. Negative affect | .40c | .18 | .30b | −.19 | −.55c | −.50c | −.58c | −.59c |
p < .05.
p < .01.
p < .001.
Table V.
Hierarchical Multiple Regression of Positive and Negative Affect on Role Identity, Illness Intrusion, and Their Interactiona
| Positive affect |
Negative affect |
|||||
|---|---|---|---|---|---|---|
| Δ R 2 | F | β | Δ R 2 | F | β | |
| Step 1 | .05 | 3.03b | .17 | 10.46d | ||
| Pain | − .26 b | .43 d | ||||
| Disability | .05 | − .06 | ||||
| Step 2 | .16 | 10.26d | .07 | 4.80c | ||
| Pain | −.21b | .39d | ||||
| Disability | .07 | − .10 | ||||
| Intrusion | − .20 d | .21b | ||||
| Identity | .36 d | − .19 b | ||||
| Step 3 | .01 | 0.76 | .03 | 3.92b | ||
| Pain | −.19 | .36d | ||||
| Disability | .07 | −.09 | ||||
| Intrusion | −.19 | .18 | ||||
| Identity | .36d | −.21b | ||||
| Identity × intrusion | − .08 | .18 b | ||||
| Step 4 | .30 | 19.74d | .26 | 18.33d | ||
| Pain | −.11 | .29c | ||||
| Disability | .09 | −.12 | ||||
| Intrusion | .03 | −.04 | ||||
| Identity | .15b | −.01 | ||||
| Identity × intrusion | .04 | .06 | ||||
| Self-esteem | .38 d | − .31 c | ||||
| Illness self-esteem | .09 | − .13 | ||||
| Self-efficacy | .36 d | − .34 d | ||||
| Total equation | R2 = .51, F = 13.00d | R2 = .27, F = 13.83d | ||||
Beta coefficients of new variables entered at each step (which correspond to the change in R2) appear in boldface. The final step contains coefficients for direct effects (illustrated in Figure 2). Indirect effects via competence mediators (self-esteem, illness self-esteem and self-efficacy) are calculated by subtracting the coefficient of a particular predictor from its coefficient at the previous step (Illustrated in Figure 4).
p < .05.
p < .01.
p < .001.
Table VI.
Hierarchical Multiple Regression of Competence Variables (Self-Efficacy, Self-Esteem, and Illness Self-Esteem) on Role Identity, Illness Intrusion, and Their Interaction
| Self-efficacy |
Self-esteem |
Illness self-esteem |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Δ R 2 | F | β at step | Δ R 2 | F | β at step | Δ R 2 | F | β at step | |
| Equation 1 | .11 | 6.62c | .03 | 1.79 | .11 | 6.18c | |||
| Pain | −.31c | −.10 | −.17 | ||||||
| Disability | −.05 | −.11 | −.20d | ||||||
| Equation 2 | .11 | 7.46d | .16 | 6.16d | .14 | 9.62d | |||
| Pain | −.25b | −.03 | −.09 | ||||||
| Disability | .00 | −.03 | −.08 | ||||||
| Intrusion | −.25c | −.32c | −.41d | ||||||
| Identity | .25c | .28c | .10 | ||||||
| Equation 3 | .05 | 7.49c | .01 | 0.75 | .00 | 0.66 | |||
| Pain | −.21b | −.02 | −.08 | ||||||
| Disability | −.01 | −.04 | −.08 | ||||||
| Intrusion | −.21b | −.31c | −.39d | ||||||
| Identity | .27d | .28c | .10 | ||||||
| Identity × intrusion | −.24c | .08 | −.07 | ||||||
| Total equation | R2 = .28, F = 7.83d | R2 = .20, F = 5.06d | R2 = .25, F = 6.84d | ||||||
p < .10.
p < .05.
p < .01.
p < .001.
Fig. 2.

Direct paths between predictor and mediating variables. Only significant paths are shown to simplify the diagram.
Fig. 3.

Indirect paths showing effects of pain, social role identity, and illness intrusion mediated via competence variables (self-efficacy, self-esteem, and illness self-esteem).
Positive Affect
Pain, role intrusion, and social role identities had significant effects on positive affect as they entered the equation (see Table V). At the final step, however, direct effects were found only for social role identities, such that important identities predicted greater positive affect (β = .15). Figure 2 also shows that important identities were related to increased self-efficacy (β = .27) and self-esteem (β = .28) (Table VI); and, in turn, greater self-esteem (β = .38) and self-efficacy (β = .36) contributed to positive affect. The interaction term was not significant, indicating that role identity does not moderate the effect of illness intrusion on positive affect. Step-to-step changes in the regression coefficients indicated that identity also had an indirect effect (β = .15) on positive affect via competence mediators (see Figure 3).
Negative Affect
Table V shows that pain, intrusion, and identity also had significant effects on negative affect as they entered the equation, but only pain (β = .29) had a significant direct effect (Figure 2). In addition, role intrusions were inversely related to the three measures of competence (Table VI); and in turn, greater self-efficacy (β = −.34) and self-esteem (β = −.31) were associated with lower negative affect.
The interaction term of illness intrusion-by-role identity was also a significant predictor of negative affect, and is illustrated in Figure 4.5 As hypothesized, negative affect increased sharply with greater illness intrusion into important role identities. Less important identities were related to higher negative affect, regardless of illness intrusion level.
Fig. 4.
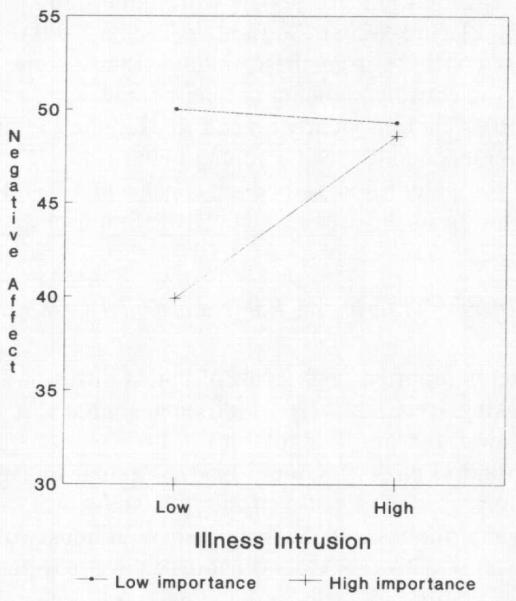
Interaction of role identity importance × illness intrusions.
With regard to indirect effects on negative affect, Figure 3 shows that competence variables mediated the effects of pain, the combined effects of intrusion-by-identity, and role identity. The effect of identity on negative affect was entirely indirect (−.20) via competence.
DISCUSSION
Several theoretical perspectives suggest that important identities contribute to self-esteem (e.g., McCall & Simmons, 1966; Rosenberg, 1979), but few empirical studies have found this effect. Findings from the path analyses support several propositions set forth by identity theory. Important identities were related to greater self-esteem and feelings of self-efficacy (Figure 1, Path c), which in turn, affected psychological well-being (Path d). Results also confirm the "identity-relevant" hypothesis (Thoits, 1991) that chronic illness should be most psychologically devastating when it interferes with important roles (Path e). Illness intrusions into valued role identities were accompanied by increased negative affect; for unimportant roles, negative affect did not vary across illness intrusion levels. Both the separate (main) and combined (interaction) effects of identity and illness intrusions on psychological well-being operated through competence and self-esteem processes (Path f). These findings are consistent with the mediating mechanisms proposed by role theorists (e.g., Pearlin, 1983; Pearlin et al., 1981), who hypothesize that a decreased sense of mastery and self-esteem mediate the relationship between identity disruptions and psychological well-being. The present findings also complement reports from prior arthritis studies that satisfaction with the performance of valued role tasks (Blalock et al., 1988) and a sense of competence (Smith et al., 1991) mediate the relationship between illness stressors and psychological adjustment. The ability to maintain a certain level of role functioning despite pain and physical limitations probably leads to a combined sense of accomplishment, self-worth, and self-efficacy over illness (Reisine & Fifield, 1988; Reisine, Grady, Goodenow & Fifield, 1989). Fulfilling role activities may be especially important for people with limited physical abilities (Heller, Thompson, Vlachos-Weber, Steffen, & Trueba, 1991).
One must conclude from these findings that a sense of competence is essential to subjective well-being among people with arthritis. As other researchers note, “There is clearly a need to examine the linkages between perceived competence and specific coping behaviors … to determine the activities that competent-feeling people engage in … to maintain their satisfaction with life in the face of adversity” (Smith et al., 1991, p. 1238).
Effect of Arthritis on Roles: Anecdotal Comments
Respondents reported high levels of illness intrusion into roles, especially homemaking (see Table II). Additional analyses of open-ended responses provided further insight about how women adapt to these intrusions (Abraído-Lanza & Guier, 1997). Women engaged in “identity guarding”: they preserved a sense of identity, self-worth, and competence by performing any role task, even if minimal. With housework, for example, they accommodated activities around chores they could perform, and took time to complete more physically demanding tasks. Wiener (1984) also observed this phenomenon, which she called “pacing,” in her qualitative study of (predominantly) women with RA. She concluded that as “activities are what lead one to view oneself as normal,” pacing is the means by which people with arthritis maintain a balance between the normal and “abnormal” selves (p. 94). Many participants equated homemaking with being active, and went to great lengths to perform household work, maintain the homemaker identity, and avoid feeling useless (inútil) and incompetent. These findings are consistent with reports that a sense of competence is one of the most rewarding aspects of the homemaker role (Kibria, Barnett, Baruch, Marshall, & Pleck, 1990), and that keeping up with housework helps maintain a competent self-image (Wiener, 1984). The fear of becoming useless is commonly reported in qualitative studies of people with chronic illnesses (e.g., Charmaz, 1983). The need to remain active prompted many women in this study to luchar (struggle) with the pain and role intrusions of arthritis (Abraído-Lanza et al., 1996), thereby enhancing feelings of self-efficacy, competence, and subjective well-being.
The mother identity appeared to serve a unique protective function. Concerns about their children's future inspired many women to face the disease with courage. The protective role of being a mother was epitomized in the case of one respondent, a single mother, who had contemplated suicide but decided not to end her life for fear of leaving her daughter alone. Another respondent's comments were more typical of how the mother role served a protective function. In spite of her illness, she drew upon her inner strength to fulfill the role, which proved to be especially rewarding and beneficial to psychological well-being,
Me hago la menle más fuerte, y se que los tengo que vestir, que los tengo que bañar, que los tengo que atender, y lo hago. Es una obligación que tengo, y tengo que responder por ellos … Me pongo a mirarlos, y cualquier cosita que hagan ellos, cualquier carrita o “monerito” que hagan, me hace tan contenta y me pone a pensar que yo cree esos niñnos, que vinieron de mi, y me hace sentir tan feliz … me olvido de mis problemas y mi dolor, y me concentro más en ellos. (I make my mind stronger, and I know that I have to dress [my children], that I have to bath them, that I have to take care of them, and I do it. It's an obligation that I have, and I have to honor it for them … I look at them, and whatever little thing they do, the cute little faces they make, the way they play and “monkey around”, and it makes me so happy and gets me thinking that I raised those children, they came from me, and it makes me feel so happy … I forget about my problems and my pain, and I concentrate more on them.)
These latter comments also illustrate that women looked at their children as products of their own resilience in adapting to arthritis. It was not uncommon for respondents, upon reflecting on their illness and life circumstances, to take great pride in reporting that despite living with the pain and limitations of arthritis and other stressors (e.g., neighborhood quality), their children were happy, drug-free, and had graduated from, or still attended school. Despite their illness, successful fulfillment of the mother role, gauged by how younger as well as adult children “turned out,” provided many women with a sense of competence, self-esteem, and psychological well-being.
These anecdotal reports are congruent with White's (1987) assertion that people need to feel competent in roles that are important to them. They also illustrate that women are not passive, but strive to fulfill roles despite their illness. Little research explores how the motivating force of remaining active and competent contributes to adjustment among Latinas (and other people) with arthritis (Abraído-Lanza et al., 1996). The high cultural value placed on both traditional and nontraditional roles may serve a particularly protective function among Latinas.
Limitations of the Study
The cross-sectional nature of the study does not allow for statements of causality. Moreover, illness-induced changes in identity over time could not be explored. Therefore, the study provides little empirical insight into possible changes in identity among Latinas with arthritis. Only sparse research exists on psychosocial processes when identities are threatened (Ethier & Deaux, 1990, 1994).
The term “Latina” in this study was used as a general category, but one half of the sample was Puerto Rican. There are sociodemographic differences among Hispanic groups in the United States, such as age, education, income, marital status, family constellation, and access to homeland resources and social networks (Bernal & Enchautegui-de-Jesús, 1994), which could potentially affect psychological adjustment to chronic illness. Analyses by subgroups, however, were not possible due to sample size restrictions.
Other issues concern the representativeness of the sample. The marital status distribution of the sample (31.2% divorced and 23.9% separated) differed from national statistics on Latinas aged over 18 (in 1988: 8.5% were divorced, 7.5% were separated; although percentages varied by Latino subgroup; Taeuber, 1991). The effects of arthritis on marital relationships (if any) are not well-researched, but studies suggest that arthritis does not cause divorce (Revenson, 1993). The marital status distribution more likely reflects national statistics on Latinas in poverty. Marital status relates to income. In 1989, nearly half (47.5%) of Hispanic female-headed households in the United States were below the poverty level (Schmittroth, 1991; see also Stroup-Benham et al., 1992). In this regard, the sample is representative of national statistics.
The low-income status of the sample results in a confound between SES and Hispanic ethnicity. This is a common problem in research on ethnic minorities (Gibson, 1989; Jackson, 1989), stemming from the high rates of poverty among ethnic minorities in the United States. Poverty contributes to morbidity and mortality (Adler et al., 1994; Callahan & Pincus, 1995) and reduced psychological well-being, marital continuity, and family functioning (Belle, 1990, 1982). Poverty also affects the ability to fulfill role obligations related to being a mother, provider, or spouse (Wolf, 1987, cited in Belle, 1990). The extent to which the stress of poverty affected variables in the present study cannot be estimated. The SES confound also raises issues of generalizability to other Hispanic (and non-Hispanic) samples of different SES levels. Arthritis stressors may be relatively minor compared to the larger social problems that people with limited economic resources encounter on a daily basis.
Directions for Future Research
The effects of multiple roles on psychological well-being are rarely studied among Latinas or women with arthritis, and require further study. More research is needed on the benefits of nontraditional roles for Latinas. With some notable exceptions (e.g., Amaro, Russo, & Johnson, 1987; Krause & Markides, 1985; Ross, Mirowsky, & Ulbrich, 1983), few studies focus on such roles. The current study contained only a small number of employed women, illustrating the severe effect of arthritis on paid work role. Among people with arthritis, unemployment rates due to disability are especially high (Yelin, 1992), and are compounded by physical job requirements (Yelin, Henke, & Epstein, 1986). The majority of women in this study had been employed as semiskilled or unskilled manual laborers (factory workers, housekeepers), which require manual dexterity and a high degree of physical labor. Moreover, several women mentioned that their previous jobs were not necessarily physically challenging, but they could not endure the demands of commuting. Negotiating the New York City mass transit system (subways, buses, or both), requires climbing stairs, “strap-hanging,” and standing for long, crowded commutes—all of which can be difficult especially for people with arthritis. For those with limited economic resources, less physically demanding, more expensive means of transportation (e.g., driving or taking privately run “express buses”) are not available alternatives. Despite the small number of employed workers in the sample, the paid work role was highly valued. These findings are striking, given that much prior research on Latinas' roles has focused on traditional social identities (e.g., being a mother). Non-Hispanic people with rheumatoid arthritis report that employment makes them feel better and increases self-esteem (Gaston-Johansson, Gustafsson, Felldin, & Sanne, 1990). Both current and former paid workers in this study expressed similar feelings. Although losing a valued identity is psychologically devastating in its own right, it is also important to consider what functions the identity served (Deaux, 1993, 1994). A lower income and standard of living result from work loss due to disability. As one depressed respondent noted, “I don't see anything positive about my illness, because I used to work, I'm not working anymore, so the income is not the same. I'm restricted completely in what I do.” Researchers have called for a more expanded view of how nontraditional roles, such as paid work, affect psychological well-being among Latinas (Amaro et al., 1987). More research is needed towards that goal, as well as understanding the contexts that limit paid work opportunities for Latinas with illness, and their socioeconomic ramifications.
Future research should also continue to explore culturally protective factors among people with chronic illnesses. The mother role was rated as particularly important, and served a protective function. Respondents indicated that their children kept them “going,” and evaluated their coping with arthritis in terms of their (young and adult) children's well-being. The importance of family roles among Latinos (Landrine, 1992), and sense of accomplishment in terms of offspring has been noted in other studies of Latinas (Sánchez-Ayéndez, 1988). The extent to which the role of mother contributes to resilience among women with illness remains an empirical question. Anecdotal accounts of women with AIDS, for example, suggest that finding appropriate guardians for their children is a primary concern. One wonders if concerns about their children's future and the desire to fulfill the mother role for as long as possible enhances resilience and quality of life among Latinas and other women with chronic and terminal illnesses. The development of models of resilience are especially appropriate (O'Leary & Ickovics, 1995). It is critical to understand how cultural values contribute to women's thriving despite “la lucha” (the struggle) that characterizes the experiences of Latinas (Zavala-Martínez, 1987).
Footnotes
This research was part of the author's dissertation, which was supported by grants from the Spring Foundation for Contemporary Research on Women; a Dissertation Grant from the Minority Fellowship Program of the American Psychological Association; a City University of New York President's Dissertation Year Award from the MAGNET program, and a Stanley Milgram Research Award. Support for conducting this research was also provided by a Summer Student Fellowship from the New York Chapter of the Arthritis Foundation, and a grant to the Spanish Arthritis Self-Management Program Evaluation study (K. Lorig, Principal Investigator), awarded by the National Center for Nursing Research (1R01 NR03146-01). Support for preparing this manuscript was provided by a Postdoctoral Research Fellowship from the Psychiatric Epidemiology Training program at Columbia University (MH 13043-23). Tracey A. Revenson provided invaluable feedback on this work. Acknowledgment of my gratitude for her mentorship is limited only by journal space limitations. I am also indebted to Allan Gibofsky for facilitating access to the research site. I thank Kay Deaux, Michelle Fine, Suzanne Ouellette, and Gary Winkel for earlier comments on this work; and Eleanor Ortiz and Beth Brofee Stark for their research assistance.
Scales were translated either by the Stanford Arthritis Center for the Spanish Arthritis Self-Management Program Evaluation study (SASMP; Lorig, 1993), or a team in New York City.
To avoid the multicollinearity problems that may arise when two continuous variables form an interaction term, deviation scores were created for the illness intinsion and role identity variables by subtracting the mean score from respondents' raw scores. In this procedure, known as centering, the interaction effect (i.e., the R2-change and associated significance test) is the same for raw and centered scores. However, the constant, unstandardized regression coefficients, and the main effects of the variables constituting the interaction change (Finney, Mitchell, Cronkite, & Moos, 1984).
The regression lines were plotted following procedures recommended by Cohen and Cohen (1983), using 1 standard deviation above and below the mean to represent high and low role identity scores, respectively.
REFERENCES
- Abraído-Lanza AF, Guier C. The influence of culture and class on health and psychological thriving. 1997. Manuscript in preparation. [Google Scholar]
- Abraído-Lanza AF, Guier C, Revenson TA. Coping and social support resources among Latinas with arthritis. Arthritis Care and Research. 1996;9:501–508. doi: 10.1002/art.1790090612. [DOI] [PubMed] [Google Scholar]
- Adler NE, Boyce T, Chesney MA, Cohen S, Folkman S, Kahn RL, Syme SL. Socioeconomic status and health. American Psychologist. 1994;49:15–24. doi: 10.1037//0003-066x.49.1.15. [DOI] [PubMed] [Google Scholar]
- Allaire SH. Employment and household work disability in women with rheumatoid arthritis. Journal of Applied Rehabilitation Counseling. 1992;23:44–51. [Google Scholar]
- Amaro H, Russo NF, Johnson J. Family and work predictors of psychological well-being among Hispanic women professionals. Psychology of Women Quarterly. 1987;11:505–521. [Google Scholar]
- Andrews F, Withey RS. Social indicators of well-being. Plenum Press; New York: 1976. [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator distinction in Social Psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Belle D. The impact of poverty on social networks and supports. Marriage and Family Review. 1982;5:89–103. [Google Scholar]
- Belle D. Poverty and women's mental health. American Psychologist. 1990;45:385–389. [Google Scholar]
- Bernal G, Enchautegui-de-Jesús N. Latinos and Latinas in community psychology: A review of the literature. American Journal of Community Psychology. 1994;22:531–557. doi: 10.1007/BF02506892. [DOI] [PubMed] [Google Scholar]
- Blalock SJ, DeVellis RF, Brown GK, Wallston KA. Validity of the Center for Epidemiologic Studies Depression Scale in arthritis populations. Arthritis and Rheumatism. 1989;32:991–997. doi: 10.1002/anr.1780320808. [DOI] [PubMed] [Google Scholar]
- Blalock SJ, DeVellis BM, DeVellis RF, Giorgino KB, Sauter SVH, Jordan JM, Keefe FJ, Mutran EJ. Psychological well-being among people with recently diagnosed rheumatoid arthritis. Arthritis and Rheumatism. 1992;35:1267–1272. doi: 10.1002/art.1780351105. [DOI] [PubMed] [Google Scholar]
- Brown JD, McGill KL. The cost of good fortune: When positive life events produce negative health consequences. Journal of Personality and Social Psychology. 1989;57:1103–1110. doi: 10.1037//0022-3514.57.6.1103. [DOI] [PubMed] [Google Scholar]
- Callahan LF. Arthritis as a women's health issue. Arthritis Care and Research. 1996;9:159–162. doi: 10.1002/1529-0131(199606)9:3<159::aid-anr1790090302>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- Callahan LF, Pincus T. Mortality in the rheumatic diseases. Arthritis Care and Research. 1995;8:229–241. doi: 10.1002/art.1790080406. [DOI] [PubMed] [Google Scholar]
- Campbell A, Converse PE, Rogers WL. The quality of American life. Russell Sage; New York: 1976. [Google Scholar]
- Canino GJ, Rubio-Stipec M, Shrout P, Bravo M, Stolberg R, Bird HR. Sex differences and depression in Puerto Rico. Psychology of Women Quarterly. 1987;11:443–459. [Google Scholar]
- Charmaz K. Loss of self: A fundamental form of suffering in the chronically ill. Sociology of Health and Illness. 1983;5:168–195. doi: 10.1111/1467-9566.ep10491512. [DOI] [PubMed] [Google Scholar]
- Cohen J. A power primer. Psychological Bulletin. 1992;112:155–159. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- Cohen J, Cohen P. Applied multiple regression and correlation analysis for the behavioral sciences. 2nd ed. Erlbaum; Hillsdale, NJ: 1983. [Google Scholar]
- Deaux K. Reconstructing social identity. Personality and Social Psychology Bulletin. 1993;19:4–12. [Google Scholar]
- Deaux K. Enacting social identity: Maintaining stability and dealing with change. The Graduate School, City University of New York; New York: 1994. Unpublished manuscript. [Google Scholar]
- Devins GM, Edworthy SM, Guthrie NG, Martin L. Illness intrusiveness in rheumatoid arthritis: Differential impact on depressive symptoms over the adult lifespan. Journal of Rheumatology. 1992;19:709–715. [PubMed] [Google Scholar]
- Diener E. Subjective well-being. Psychological Bulletin. 1984;95:542–575. [PubMed] [Google Scholar]
- Dreyer NA, Woods NF, James SA. ISRO: A scale to measure sex-role orientation. Sex Roles. 1981;7:173–182. [Google Scholar]
- Ethier K, Deaux K. Hispanics in ivy: Assessing identity and perceived threat. Sex Roles. 1990;22:427–440. [Google Scholar]
- Ethier K, Deaux K. Negotiating social identity in a changing context: Maintaining identification and responding to threat. Journal of Personality and Social Psychology. 1994;67:243–251. [Google Scholar]
- Felton BJ, Revenson TA. Coping with chronic illness: A study of illness controllability and the influence of coping strategies on psychological adjustment. Journal of Consulting and Clinical Psychology. 1984;52:343–353. doi: 10.1037//0022-006x.52.3.343. [DOI] [PubMed] [Google Scholar]
- Finney JW, Mitchell RE, Cronkite RC, Moos RH. Methodological issues in estimating main and interactive effects: Examples from coping/social support and stress field. Journal of Health and Social Behavior. 1984;25:85–98. [PubMed] [Google Scholar]
- Fitzpatrick R, Newman S, Lamb R, Shipley M. Social relationships and psychological well-being in rheumatoid arthritis. Social Science and Medicine. 1988;27:399–403. doi: 10.1016/0277-9536(88)90275-4. [DOI] [PubMed] [Google Scholar]
- Fries JF, Spitz P, Kraines RG, Holman H. Measurement of patient outcome in arthritis. Arthritis and Rheumatism. 1980;23:137–145. doi: 10.1002/art.1780230202. [DOI] [PubMed] [Google Scholar]
- Gaston-Johansson F, Gustafsson M, Felldin R, Sanne H. A comparative study of feelings, attitudes and behaviors of patients with fibromyalgia and rheumatoid arthritis. Social Science and Medicine. 1990;31:941–947. doi: 10.1016/0277-9536(90)90034-p. [DOI] [PubMed] [Google Scholar]
- Gibson RC. Minority aging research: Opportunity and challenge. Journal of Gerontology. 1989;44:S1–S2. doi: 10.1093/geronj/44.1.s2. [DOI] [PubMed] [Google Scholar]
- Goodenow C, Reisine ST, Grady KE. Quality of social support and associated social and psychological functioning in women with rheumatoid arthritis. Health Psychology. 1990;9:266–284. doi: 10.1037//0278-6133.9.3.266. [DOI] [PubMed] [Google Scholar]
- Heller K, Thompson MG, Vlachos-Weber I, Steffen AM, Trueba PE. Support interventions for older adults: Confidante relationships, perceived family support, and meaningful role activity. American Journal of Community Psychology. 1991;19:139–146. doi: 10.1007/BF00942262. [DOI] [PubMed] [Google Scholar]
- Hubbell LJ. Values under siege in Mexico: Strategies for sheltering traditional values from change. Journal of Anthropological Research. 1993;49:1–16. doi: 10.1086/jar.49.1.3630627. [DOI] [PubMed] [Google Scholar]
- Jackson JS. Race, ethnicity and psychological theory and research. Journal of Gerontology. 1989;44:P1–P2. doi: 10.1093/geronj/44.1.p1. [DOI] [PubMed] [Google Scholar]
- Katz PP, Yelin EH. Life activities of persons with rheumatoid arthritis with and without depressive symptoms. Arthritis Care and Research. 1994;7:69–77. doi: 10.1002/art.1790070205. [DOI] [PubMed] [Google Scholar]
- Kibria N, Barnett RC, Baruch GK, Marshall NL, Pleck JH. Homemaking-role quality and the psychological well-being and distress of employed women. Sex Roles. 1990;22:327–345. [Google Scholar]
- Krause N, Markides KS. Employment and psychological well-being in Mexican American women. Journal of Health and Social Behavior. 1985;26:15–26. [PubMed] [Google Scholar]
- Landrine H. Clinical implications of cultural differences: The referential versus the indexical self. Clinical Psychology Review. 1992;12:401–415. [Google Scholar]
- Larson RJ, Diener E, Emmons RA. An evaluation of subjective well-being measures. Social Indicators Research. 1985;17:1–17. [Google Scholar]
- Liang MH, Larson MG, Cullen KE, Schwartz JA. Comparative measurement efficiency and sensitivity of five health status instruments for arthritis research. Arthritis and Rheumatism. 1985;28:542–547. doi: 10.1002/art.1780280513. [DOI] [PubMed] [Google Scholar]
- Lorig KR. Spanish arthritis self-management program evaluation study. Stanford University Arthritis Center; Palo Alto, CA: 1993. [Google Scholar]
- Lorig K, Chastain R, Ung E, Shoor S, Holman H. Development and evaluation of a scale to measure the perceived self-efficacy in people with arthritis. Arthritis and Rheumatism. 1989;32:37–44. doi: 10.1002/anr.1780320107. [DOI] [PubMed] [Google Scholar]
- Luhtanen R, Crocker J. A collective self-esteem scale: Self-evaluation of one's social identity. Personality and Social Psychology Bulletin. 1992;18:302–318. [Google Scholar]
- Marín G, Marín BV. Research with Hispanics. Sage; Newbury Park, CA: 1991. [Google Scholar]
- Marín G, Sabogal F, Marín BV, Otero-Sabogal R, Perez-Stable EJ. Development of a short acculturation scale for Hispanics. Hispanic Journal of Behavioral Sciences. 1987;9:183–205. [Google Scholar]
- McCall GJ, Simmons JL. Identities and Interactions. Free Press; New York: 1966. [Google Scholar]
- NIAMS (National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health) Arthritis, rheumatic diseases, and related disorders: 1993 research highlights (NIH Publication No. 93-3413) Public Health Service of the Dept. of Health and Human Services; Washington, DC: 1993. [Google Scholar]
- Oatley K, Bolton W. A social-cognitive theory of depression in reaction to life events. Psychological Review. 1985;92:372–388. [PubMed] [Google Scholar]
- O'Leary VE, Ickovics JR. Resilience and thriving in response to challenge: An opportunity for a paradigm shift in women's health. Women s Health: Research on Gender Behavior and Policy. 1995;1:121–142. [PubMed] [Google Scholar]
- Padilla GV, Perez E. Minorities and arthritis. Arthritis Care and Research. 1995;8:251–256. doi: 10.1002/art.1790080408. [DOI] [PubMed] [Google Scholar]
- Pearlin LI. Role strains and personal stress. In: Kaplan JG, editor. Psychosocial stress: Trends in theory and research. Academic Press; New York: 1983. pp. 3–32. [Google Scholar]
- Peariin LI, Lieberman MA, Menaghan EG, Mullan JT. The stress process. Journal of Health and Social Behavior. 1981;22:337–356. [PubMed] [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Reisine ST, Fifield J. Defining disability for women and the problem of unpaid work. Psychology of Women Quarterly. 1988;12:401–415. [Google Scholar]
- Reisine ST, Goodenow C, Grady KE. The impact of rheumatoid arthritis on the homemaker. Social Science and Medicine. 1987;25:89–95. doi: 10.1016/0277-9536(87)90210-3. [DOI] [PubMed] [Google Scholar]
- Reisine ST, Grady KE, Goodenow C, Fifield J. Work disability among women with rheumatoid arthritis: The relative importance of disease, social, work, and family factors. Arthritis and Rheumatism. 1989;32:538–543. doi: 10.1002/anr.1780320505. [DOI] [PubMed] [Google Scholar]
- Revenson TA. The role of social support with rheumatic disease. In: Newman SP, Shipley M, editors. Baillière's clinical rheumatology: International practice and research. Vol. 7. Baillière Tindall; London: 1993. pp. 377–396. [DOI] [PubMed] [Google Scholar]
- Revenson TA, Felton BJ. Disability and coping as predictors of psychological adjustment to rheumatoid arthritis. Journal of Consulting and Clinical psychology. 1989;57:344–348. doi: 10.1037//0022-006x.57.3.344. [DOI] [PubMed] [Google Scholar]
- Revenson TA, Schiaffino KM, Majerovitz SD, Gibofsky A. Social support as a double-edged sword. The relation of positive and problematic support to depression among rheumatoid arthritis patients. Social Science and Medicine. 1991;33:807–813. doi: 10.1016/0277-9536(91)90385-p. [DOI] [PubMed] [Google Scholar]
- Rosenberg M. Society and the adolescent self-image. Princeton University Press; Princeton, NJ: 1965. [Google Scholar]
- Rosenberg M. Conceiving the Self. Basic Books; New York: 1979. [Google Scholar]
- Ross CE, Mirowsky J, Ulbrich P. Distress and the traditional female role: A comparison of Mexicans and Anglos. American Journal of Sociology. 1983;89:670–682. doi: 10.1086/227909. [DOI] [PubMed] [Google Scholar]
- Salgado de Snyder VN. Factors associated with acculturative stress and depressive symptomatology among married Mexican immigrant women. Psychology of Women Quarterly. 1987;11:475–488. [Google Scholar]
- Sánchez-Ayéndez M. Puerto Rican elderly women: The cultural dimension of social support networks. Women and Health. 1988;14:239–252. [PubMed] [Google Scholar]
- Schmittroth L. Statistical record of women worldwide. Gale Research; Detroit, MI: 1991. [Google Scholar]
- Sherbourne CD. Pain measures. In: Steward AL, Ware JE, editors. Measuring functioning and well-being: The medical outcomes study approach. Duke University Press; Durham, NC: 1992. [Google Scholar]
- Smith CA, Dobbins CJ, Wallston KA. The mediational role of perceived competence in psychological adjustment to rheumatoid arthritis. Journal of Applied Social Psychology. 1991;21:1218–1247. [Google Scholar]
- Stroup-Benham CA, Lawrence RH, Treviño FM. CES-D factor structure among Mexican American and Puerto Rican women from single- and couple-headed households. Hispanic Journal of Behavioral Sciences. 1992;14:310–326. [Google Scholar]
- Stryker S, Serpe RT. Commitment, identity salience, and role behavior. In: Ickes W, Knowles ES, editors. Personality, roles, and social behavior. Springer-Verlag; New York: 1982. [Google Scholar]
- Tajfel H. Human groups and social categories. Cambridge University Press; Cambridge, U.K.: 1981. [Google Scholar]
- Taeuber C. Statistical handbook on women in America. Oryx; Phoenix: 1991. [Google Scholar]
- Thoits PA. On merging identity theory and stress research. Social Psychology Quarterly. 1991;54:101–112. [Google Scholar]
- U.S. Department of Commerce, Bureau of the Census . Poverty in the United States: 1991 (Current Population Reports, Series P-60, No. 181) U.S. Government Printing Office; Washington, DC: Aug, 1992. [Google Scholar]
- U.S. Department of Health and Human Services . Prevalence of selected chronic conditions: United States. Feb, 1993. pp. 1986–1988. Series 10: Data from the National Health Interview Survey, No. 182. [Google Scholar]
- Van Meek LG. Stress, support, self-concepts and depression among women of Mexican descent. Paper presented at the 100th Annual convention of the American Psychological Association; Washington, D.C.. 1992. [Google Scholar]
- Vazquez-Nuttall EV, Romero-Garcia I, De Leon B. Sex roles and perceptions of femininity and masculinity of Hispanic women: A review of the literature. Psychology of Women Quarterly. 1987;11:409–425. [Google Scholar]
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS Scales. Journal of Personality and Social Psychology. 1988;54:1063–1070. doi: 10.1037//0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- White RW. Seeking the shape of personality: A memoir. Homestead; Marlborough, NH: 1987. [Google Scholar]
- Wiener CL. The burden of rheumatoid arthritis. In: Strauss AL, Corbin J, Fagerhaugh S, Glaser BG, Maines D, Suczek B, Wiener CL, editors. Chronic illness and the quality of life. C. V. Mosby; St. Louis, MO: 1984. pp. 88–98. [Google Scholar]
- Yelin EH. Arthritis: The cumulative impact of a common chronic condition. Arthritis and Rheumatism. 1992;35:489–497. [PubMed] [Google Scholar]
- Yelin EH, Henke CJ, Epstein WV. Work disability among persons with musculoskeletal conditions. Arthritis and Rheumatism. 1986;29:1322–1333. doi: 10.1002/art.1780291104. [DOI] [PubMed] [Google Scholar]
- Zavala-Martínez I. En la Lucha: The economic and socioemotional struggles of Puerto Rican Women. Women and Therapy. 1987;6:3–24. [Google Scholar]