

Abstract
Basal Cell Carcinoma (BCC) is almost exclusively seen in head-neck region with rare involvement of trunk and extremities. The tumour is commonly seen on nose, eyelids, at the inner canthus of eyes and behind the ears. Adenoid type of BCC is one of the rare histopathological types of BCC which has not found to have any site predilection. We report two cases of BCC occurring at an unusual site i.e., lower back and both of them showed adenoid type of BCC on histopathology. Morphologically they were pigmented and ulcerative type of BCC respectively.
Keywords: Adenoid basal cell carcinoma, rare histopathological variant, unusual location
Introduction
What was known?
Adenoid type of BCC is a rare histopathological variant which can morphologically present as pigmented and nonpigmented nodule or ulcer without predilection for any particular site.
Basal Cell carcinoma (BCC) constitutes 65% of epithelial tumours. It is more prevalent after the fourth decade of life and its peak incidence is at the 6th decade with male preponderance. It is exclusively seen on sun exposed and hair bearing skin especially of the face. About one-third of BCC occurs on sun protected area, suggesting factors other than solar exposure playing a role such as genetic susceptibility.[1] Adenoid type of BCC is a rare histopathological variant which can morphologically present as pigmented and nonpigmented nodule or ulcer without any site predilection.
Case Report
Two females aged 56 and 60 years, presented with asymptomatic ulcer and a painful dark colored lesion on the lumbosacral area since 10 and two months respectively.
In the first case, the lesion started as an asymptomatic raised lesion on a normal skin on the lower back evolving into a non-healing ulcer eventually over a period of 10 months. The second case noticed a painful black colored nodule on the lower back that gradually increased in size to form a large plaque within two months. There was no history of pre-existing skin condition, indigenous drug intake (containing arsenic), exposure to irradiation and trauma at the affected site prior to appearance of lesions in both these cases. Both the patients were residents of Mumbai which has not reported high content of arsenic in potable water. Family members of both the patients did not report similar skin condition.
The examination of the first case revealed a single irregular ulcer measuring about 3 × 4 cm in diameter over the sacral area overlying the natal cleft with rolled out indurated edges and sloping margins [Figure 1a]. The floor was formed by healthy granulation tissue and minimal slough with serosanguinous discharge. The ulcer was mobile and not adherent to the underlying structures. While in the second case, there was a single well defined circular blackish 3 × 2.5 cm sized plaque on the lower back in right paramedian position about 4cm above the natal cleft [Figure 1b]. There was no evidence of lymphadenopathy in both these cases.
Figure 1a.

Single, irregular ulcer of 3×4 cm, over sacral area with rolled out indurated edges and sloping margins. The floor shows healthy granulation tissue and serosanguinous discharge
Figure 1b.

Single circular plaque of 3×2.5 cm on lumbosacral area in right paramedian position. Overlying surface is irregular with brown black pigmentation
Laboratory investigations of both patients were normal except for anemia. X-Ray of lumbosacral region in both the cases did not reveal involvement of the underlying bones. There was no evidence of metastases in both the cases on radiological investigations.
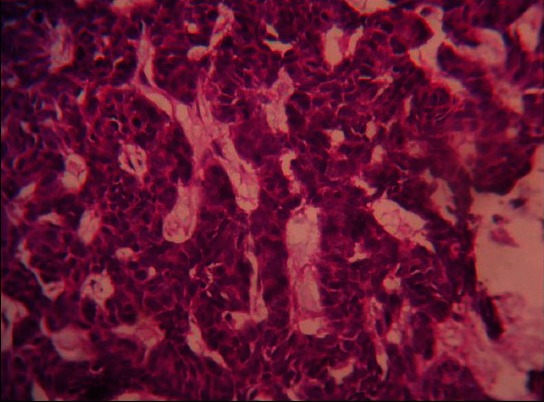
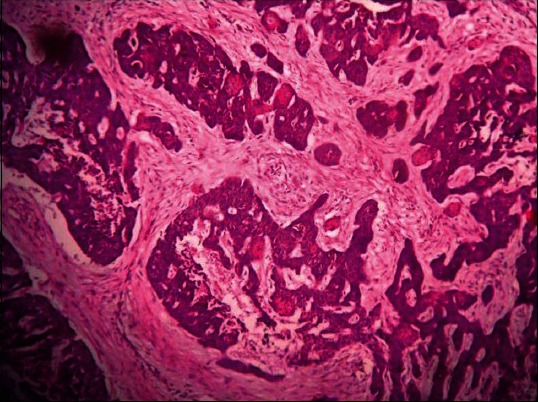
Biopsy from the lesion in both the cases revealed thinned out epidermis with masses of basaloid cells in the dermis and retracted spaces separating them from a strong stroma. The masses of basaloid cells showed palisading at the periphery. At places, the cells showed tubular differentiation with the lumina showing granular material. The cells arranged in intervening strands were suggestive of adenoid type of BCC [Figures 2a-c]. Pigmentary incontinence was marked in the second case.
Figure 2a.
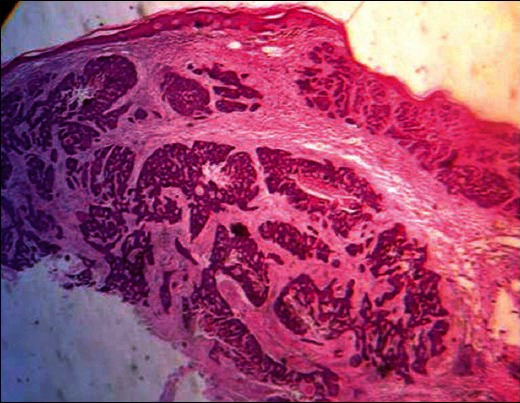
(H and E, ×40) Thinned out epidermis with masses of basaloid cells in the upper dermis, separated by stroma. Note the retraction spaces
Figure 2c.
(H and E, ×40) Tubular differentiation suggesting Adenoid type of basal cell carcinoma (BCC)
Figure 2b.
(H and E, ×40) The mid and lower dermis shows masses of tumor cells with tubular differentiation and granular material in the lumina, suggesting Adenoid type of basal cell carcinoma (BCC)
Discussion
BCC accounts for 65% of the epithelial tumours.[1] The role of solar exposure is well documented and contributes to its predilection for the head and neck region (around 75-86%).[2,3] Rest of the lesions appear on other areas and only 10% of all BCCs are located on the trunk.[4] There is paucity of literature on exact incidence of adenoid BCC but Bastiaens, et al. reported the incidence of 1.3%.[5] It is often regarded as a low grade malignancy compared to other subtypes like nodular and morpheic form which are of high grade.
The definition of an unusual site for BCC is not clear. Unusual location has been arbitrarily defined on the basis of percentage of incidence, an index referred to as anatomical incidence called the Relative Tumor Density (RTD) index, which considers the ratio between the proportion of tumour in a certain location and the proportion of the surface area on the same location and; the sites considered as such in the literature in agreement with the experts. These sites are breasts, periungual region,[6] palms, soles, glutei and intertriginous areas like axillae, groins, and genitals.[3,4] Niwa, et al. reported five cases of BCC at axillae, groins, foot and pinnae.[7]
The factors determining the anatomical distribution pattern of BCC are not clear. Sun exposure is suggested as the primary factor but these tumours are rarely seen on forearm, hands and lower limbs, despite significant sun exposure. Regarding possible association of tumour location with histological subtypes, some studies showed that unexposed areas like the trunk and the limbs display predominantly superficial type of BCC, while those on sun exposed areas show mainly nodular pattern. Scrivener, et al. found nose to be the common site for morpheaform BCC.[8] In Basal Cell Nevus Syndrome, the BCC lesions are also found on palms and soles. Betti, et al. reported 6 cases of nodular BCCs on the buttocks.[1] Adenoid BCC has been reported at various sites including axillae, back, leg, inner canthus of eye, chin and forehead and rarely even cervix and prostate. Both our cases and giant BCC reported by Fresini, et al. had same location on the back and all three revealed same histology of adenoid type of BCC [Table 1].[11]
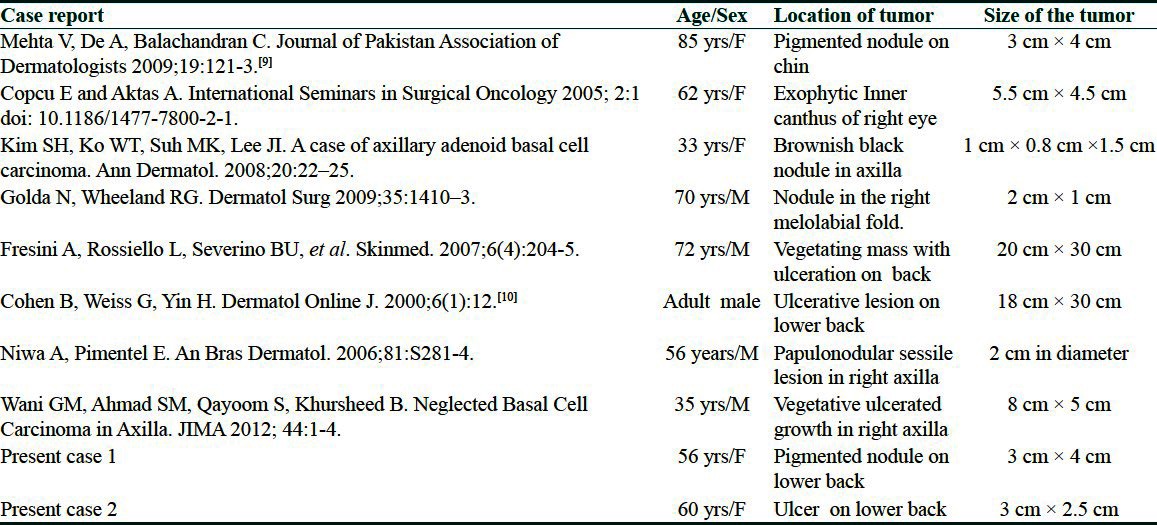
Table 1.
Clinical features of reported cases of adenoid type of basal cell carcinoma (BCC) on histopathology
Histopathology of this rare variant shows arrangement of cells in the intertwining strands and radially around islands of connective tissue, resulting in a tumour with a lace like pattern. The lumina may be filled with a colloidal substance or with an amorphous granular material, but the secretory activity of the cells lining the lumina cannot be delineated even with histochemical methods.
Management of adenoid type of BCC remains similar to other types of BCC.
What is new?
Very few cases of adenoid BCC have been reported. Present cases and review of reported cases adds the information that the adenoid type of BCC can have few unique features i.e. tendency to involve unexposed parts like back and axilla and larger size of the lesions.
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.Betti R, Bruscagin C, Inselvini E, Crosti C. Basal cell carcinomas of covered and unusual sites of the body. Int J Dermatol. 1997;36:503–5. doi: 10.1046/j.1365-4362.1997.00139.x. [DOI] [PubMed] [Google Scholar]
- 2.Roenigk RK, Ratz JL, Bailin PL, Wheeland RG. Trends in the presentation and treatment of basal cell carcinomas. J Dermatol Surg Oncol. 1986;12:860–5. doi: 10.1111/j.1524-4725.1986.tb01993.x. [DOI] [PubMed] [Google Scholar]
- 3.Nagendra Naidu DV, Rajakumar V. Perianal basal cell Carcinoma-An unusual site of occurrence. Indian J Dermatol. 2010;55:178–80. doi: 10.4103/0019-5154.62758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bogdanić B, Smud S, Bagatin D, Nola M, Mijatović D, Majerović M. Giant basal cell carcinoma of the back: A case report and review of the literature. Coll Antropol. 2009;33:315–8. [PubMed] [Google Scholar]
- 5.Bastiaens MT, Hoefnagel JJ, Bruijn JA, Westendorp RG, Vermeer BJ, Bavinck J. Differences in age, site distribution, and sex between nodular and superficial basal cell carcinomas indicate different types of tumors. J Invest Dermatol. 1998;110:880–4. doi: 10.1046/j.1523-1747.1998.00217.x. [DOI] [PubMed] [Google Scholar]
- 6.Bhagchandani L, Sanadi RE, Sattar S, Abbott RR. Basal cell carcinoma presenting as finger mass. A case report. Am J Clin Oncol. 1995;18:176–9. doi: 10.1097/00000421-199504000-00018. [DOI] [PubMed] [Google Scholar]
- 7.Niwa A, Pimentel E. Basal cell carcinoma in unusual locations. An Bras Dermatol. 2006;81:S281–4. [Google Scholar]
- 8.Scrivener Y, Grosshans E, Cribier B. Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br J Dermatol. 2002;147:41–7. doi: 10.1046/j.1365-2133.2002.04804.x. [DOI] [PubMed] [Google Scholar]
- 9.Mehta V, De A, Balachandran C. Painful hemorrhagic nodule on the chin. J Pak Assoc Dermatol. 2009;19:121–3. [Google Scholar]
- 10.Cohen B, Weiss G, Yin H. Basal cell carcinoma (BCC) causing spinal cord compression. Dermatol Online J. 2000;6:12. [PubMed] [Google Scholar]
- 11.Fresini A, Rossiello L, Severino BU, Del Prete M, Satriano RA. Giant basal cell carcinoma. Skinmed. 2007;6:204–5. doi: 10.1111/j.1540-9740.2007.06399.x. [DOI] [PubMed] [Google Scholar]