

Sir,
In the past, carbapenems have been the main stays of the infectious disease community for serious infections because of their broad-spectrum activity and stability to hydrolysis by most of the β-lactamases, including extended spectrum β-lactamases (ESBLs).[1] However, in the last decade, outbreak of carbapenem-resistant Pseudomonas aeruginosa and Acinetobacter spp. due to metallo-β-lactamases (MBLs) have been reported from different regions. MBLs have spread to other species of gram-negative bacilli.[2] These MBLs belong to Ambler's class B and Bush group 3 classification of ESBL. They can hydrolyze all classes of β-lactams except aztreonam and their activity cannot be inhibited by β-lactam inhibitors.[3] The present study was undertaken considering the paucity of data on MBL producing nosocomial nil fermenter gram-negative isolates from Kumaun region.
A total of 44 nil fermenters consisting of 32 Pseudomonas spp. and 12 Acinetobacter spp. were screened for MBL production by double disk synergy test (DDST) as described by Lee et al.[4] and disk combination test (DCT) as described by Young et al.,[5] using ceftazidime (CAZ) and imipenem (IMP) with 0.5 M ethylenediaminetetraacetic acid (EDTA; 750 μg/disk).
CAZ-EDTA combined disk test and DDST detected 36.36% and 20.45% MBL producers, respectively. IMP-EDTA DCT detected 22.7%, while IMP-DDST detected 13.8% MBL producers [Table 1].
Table 1.
Comparison of methods of MBL production using CAZ and IMP disks

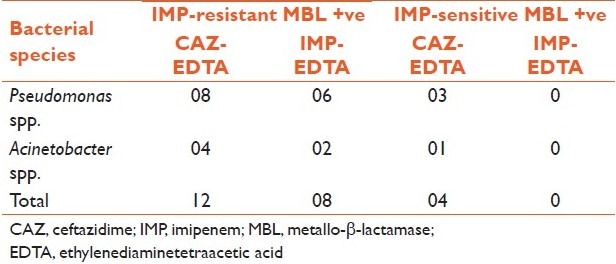
Of the 32 Pseudomonas spp., 22 were CAZ resistant and 8 were IMP resistant. Five isolates detected by DCT were negative by DDST. Of the 12 Acinetobacter spp., 6 were resistant to CAZ and 4 to IMP. Two isolates detected by CAZ-EDTA combination test were negative by DDST. Three Pseudomonas spp. and one Acinetobacter spp. sensitive to IMP were found to be MBL producer by CAZ-EDTA DCT [Table 2].
Table 2.
MBL production by IMP-sensitive and IMP-resistant isolates by using CAZ-EDTA and IMP-EDTA disk combination test
The clinical utility of carbapenem is under threat with emergence of acquired carbapenemases, particularly Ambler's class B MBLs.[1] The occurrence of an MBL-positive isolate in a hospital environment not only poses a therapeutic problem, but also is a serious concern for infection control management.[3]
In this study, 29.5% isolates were found to be MBL producers which is in agreement with the study by Hemlata et al.[6] CAZ-EDTA gave better results than IMP-EDTA similar to that reported in other studies from India.[6,7]
In this study, we also found three Pseudomonas spp. and one Acinetobacter spp., sensitive to IMP, to be MBL producers as detected by DCT. The correlation between carriage of MBL genes and carbapenem resistance is often imperfect. It is quite possible that the gene pool is more extensive than what we can detect and is either in a quiescent state or is not being detected, or both.[2] With the emergence of carbapenem-sensitive MBLs, screening only carbapenem-resistant isolates would miss MBL production in carbapenem-sensitive strains. Behra et al.[3] have recommended MBL screening for all CAZ-resistant isolates. Based on the findings of our study, we conclude that combination disk method is better than DDST. CAZ-EDTA combination disk could pick additional isolates of MBL producers as compared to IMP-EDTA disk. Hence, it could be used as a convenient method in the clinical microbiology laboratories. Though our sample size is low, microbiology laboratories must evaluate the various screening methods for detection of MBL in order to correctly report this important mechanism of antimicrobial resistance.
REFERENCES
- 1.Franklin C, Liolios L, Peleg AY. Phenotypic detection of carbapenem-susceptible metallo-ß-lactamase-producing gram-negative bacilli in the clinical laboratory. J Clin Microbiol. 2006;44:3139–44. doi: 10.1128/JCM.00879-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ikonomidis A, Tokatlidou D, Kristo D, Sofianou D, Tsakris A, Mantzana P, et al. Outbreaks in Distinct Region Due to a Single Klebseilla Pneumoniae clone carrying a blavim-1 Mettalo- β –lactamase gene. J Clin Microbiol. 2005;43:5344–7. doi: 10.1128/JCM.43.10.5344-5347.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Behera B, Mathur P, Das A, Kapil A, Sharma V. An evaluation of four different phenotypic techniques for detection of metallo-β-lactamase producing Pseudomonas aeruginosa. Indian J Med Microbiol. 2008;26:233–7. doi: 10.4103/0255-0857.39587. [DOI] [PubMed] [Google Scholar]
- 4.Lee K, Lim YS, Yong D, Yum JH, Chong Y. Evaluation of the Hodge test and the imipenem-EDTA double-disk synergy test for differentiating metallo-ß-lactamase-producing isolates of Pseudomonas spp. and Acinetobacter spp. J Clin Microbiol. 2003;41:4623–9. doi: 10.1128/JCM.41.10.4623-4629.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yong D, Lee K, Yum JH, Shin HB, Rossolini GM, Chong Y. Imipenem-EDTA disk method for differentiation of metallo-β-lactamases producing clinical isolates of Pseudomonas spp and Acinetobacter spp. J Clin Microbiol. 2002;40:3798–801. doi: 10.1128/JCM.40.10.3798-3801.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hemlata V, Sekhar U, Kamant V. Detection of métalo-β-lactamase producing Pseodomonas aeruginosa in hospitalizad patient. Indian J Med Res. 2005;122:148–52. [PubMed] [Google Scholar]
- 7.Mendiratta DK, Deotale V, Narang P. Mettalo- β -lactamase producing Pseudomonas aeroginosa in a hospital from a rural area. Indian J Med Res. 2005;121:1701–3. [PubMed] [Google Scholar]