

Abstract
Background:
Emergency Medical Services (EMS) provides out-of-hospital acute medical care to different types of serious emergencies. The team of EMS includes paramedics, besides many other staff working in the pre-hospital setting. Although the paramedics are the first responders to the patient in emergency, they face several barriers, which interfere with their efficiency.
Aim:
However, the magnitude of these obstacles is not known, hence; it was found worthwhile to evaluate the depth of these difficulties.
Materials and Methods:
A questionnaire that included eight different commonly experienced barriers and four different variables of strength was framed. The questionnaire was served to 140 paramedics in three different regions (Jeddah, Riyadh, and Dammam) of Saudi Arabia.
Results:
The positive response obtained was statistically significant for traffic congestion (P<0.01; P<0.001), nuisance by bystanders and family members (P<0.001), lack of competence of doctors and the administration in the EMS routines (P<0.05; P<0.01; P<0.001), lack of trust and confidence (P<0.001) lack of independence (P<0.001), patient's resistance (P<0.001), Interference of legal issues and litigation proceedings (P<0.05; P<0.001), paramedic's impression on general public and the family of the patients (P<0.001).
Conclusions:
The authorities in the hospitals and EMS administration should improve the barriers which interfere with the efficiency of a paramedic and cause gross humiliation to the patients, and the Health authorities should impart proper education and training to the paramedics.
Keywords: Barriers, emergency medical services, efficiency, interference, paramedics
INTRODUCTION
Emergency Medical Services (EMS) provide out-of-hospital acute medical care to different types of serious emergencies, such as life-threatening allergic reactions, poisoning due to ingestion of drugs and chemicals, lethal venoms of snakes, accidents involving bones and skull fractures, brain injuries, respiratory failure, cardiopulmonary blockade, cardiac arrest, febrile seizures, drug overdose, burns and shocks and child abuse, in addition to transport of the patients to definitive care.[1,2] The team of EMS includes the emergency physicians who have additional expertise in EMS, the paramedics (including the technicians), firefighters, and ambulance employees. The levels of services available constitute three categories; Basic Life Support (BLS), Advanced Life Support (ALS), and care by traditional healthcare professionals (nurses and/or physicians) working in the pre-hospital setting and even while on ambulances.[3] While the physicians and nurses are rarely available for the pre-hospital emergency care, most of the exigencies are managed by paramedics, including technicians and the driver of the ambulance. A paramedic is a trained health professional who is the first responder to the patient in medical emergency. The paramedics provide out of hospital medical assessment, treatment, and care. There are varying levels of paramedic practice and the employing authority determines their allotment to a specific level of care.[4]
Although the paramedics are not medically qualified, they get adequate training in the tasks they have to carry out. Nevertheless, they face several barriers and obstacles in the discharge of their duties, in addition to humiliation and dishonor. There are many barriers and obstacles, including traffic congestion, nuisance by bystanders and family members, incompetence of doctors and the administration, lack of trust and confidence bestowed on them, lack of independence given, patient's resistance, interference of legal issues and litigation proceedings, impression of people, and the family of the patients about the paramedics. These obstacles interfere with the performance and efficiency of paramedics. In view of a paucity of literature on the subject, it was found worthwhile to investigate the views of the paramedics by constituting a questionnaire, in order to understand their working and finding means and ways to improve their environment.
MATERIALS AND METHODS
A questionnaire-based study was undertaken on the significance of paramedics and their experience on barriers and obstacles during the year 2011. The questionnaire was served by e-mail and/or post to 140 paramedics in three regions of Saudi Arabia, namely Jeddah, Dammam, and Riyadh. Those who responded to the questionnaire constituted the sample. Subsequent telephonic conversation with the respondents clarified any doubts on some terms used in the questionnaire. The questionnaire was framed to evaluate the interference of traffic congestion due to accidents, road repairs, signals, VIP movements, checking by the police for relevant residence permits, ids and car papers, which make the movements very difficult and interfere with the performance of EMS personnel including paramedics; delay (interruption) in the working of paramedics caused by bystanders on the street and family members in matter of road accidents, the scuffles and embarrassment (humiliation) that delays (interrupts) the working by the of paramedics; incompetence of doctors and the administration as the cause of failures of paramedics; lack of trust and confidence bestowed on paramedics by the staff in the higher level; lack of independence allowed in decision making by the paramedics; patient resistance as the cause of failures by paramedics; interference of legal issues and litigation proceedings with the efficiency of a paramedic; and impression of people and the family of the patients about the paramedics. The scores of response were estimated by the degree of intensity as the variables, 1: Never, 2: Rarely, 3: Most of the times and 4: Always. The responses were graded on a Likert scale[5] and the variables were statistically compared by the chi-square test.
RESULTS
A total of 140 paramedics answered the questionnaire on the survey of the experiences of paramedics, relating the barriers and obstacles which interfere with their performance, in addition to their significance. The traffic congestion due to accidents, road repairs, signals and VIP movements showed the variables ‘most of the times’ and ‘always’ were statistically significant (P<0.01; P<0.001) indicating most of the respondents confirm that such a traffic congestion interferes with the performance of their duties. On the second question relating to the delay in working of paramedics due to congregation of bystanders and the family members at the site of accident and the related scuffles and embarrassment, the respondent's opinion was found to be statistically significant (P<0.001) for the variable ‘always’. Another question regarding the opinion of paramedics if their inefficiency is related with the incompetence of doctors and administrators, there was lot of discordance in the opinion. The significance probabilities for different variables were ‘rarely’ (P<0.05), and ‘most of the times’ and ‘always’ (P<0.001). The result of this interrogation revealed that the inefficiency of paramedics is related with lack of competence of doctors and administrators in the EMS routines. The fourth question was on the trust bestowed on the working of paramedics by the higher ups in the EMS, in one tone, the answer was affirmative about the variable ‘never’ (P<0.001) [Table 1 and Figure 1].
Table 1.
Response to different questions by the respondents
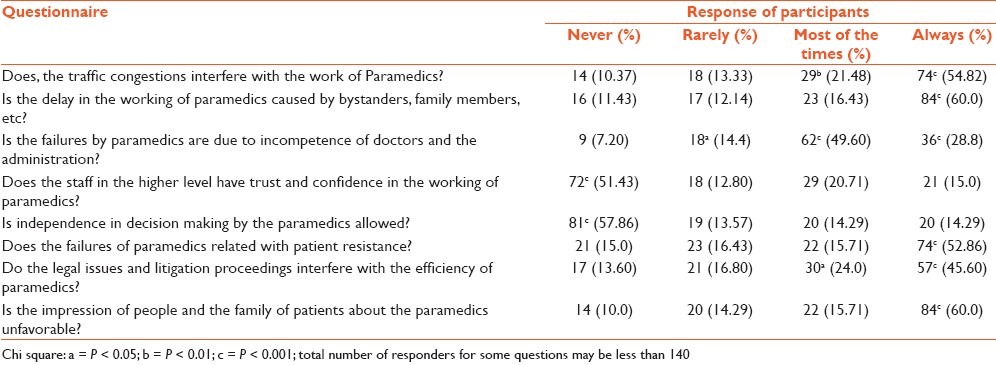
Figure 1.
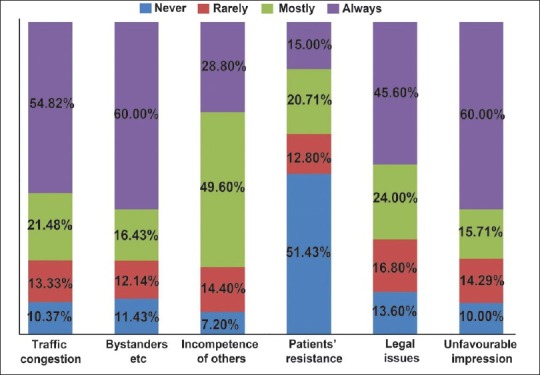
Barriers as inhibitors of effi ciency of paramedics in discharging their duties in Emergency Medical Services
Regarding decision making allowed to the paramedics, the respondents, again in one tone voted for the variable ‘never’ (P<0.001). On patience resistance as the basis for failures of paramedics, the highest response was for the variable ‘always’ (P<0.001). The legal issues and litigation proceedings faced by paramedics is also one of the consuming factors that block the efficiency of a paramedic. The response was low for the variable ‘most of the times’ (P<0.05) and high for the ‘always’ (P<0.001). The last question in the questionnaire was on the attitude of the general public and the family members of the patient, the highest response was for the variable ‘always’ (P<0.001), which indicated the impression about the paramedics is on the lowest ebb [Table 1 and Figure 1].
DISCUSSION
The task of a paramedic is to cover the distance between him and the emergent situation, however complicated, the track may be. This is always a very tedious expedition, full of hurdles. The answer to the question on traffic congestion as the means of barrier for the paramedic was affirmative, indicating that the traffic congestion interferes with the efficiency of a paramedic. Reports from most of the Asian countries (and now in some of the Arab countries), show that there are strikes, riots, insurgencies and street violence which cause road blocks and interfere with the working of the paramedics.[6] Nevertheless, in Saudi Arabia, the traffic congestion is overwhelmed with heavy traffic and congestion due to accidents, road repairs, signals, brunt of traffic regulations, VIP movements, points for the police vigilance to check relevant papers, which make the movements very difficult and interfere with the performance of EMS personnel including paramedics and also endanger the life of the patient.
The site of a road accident is often overcrowded with onlookers, bystanders, friends and relatives of the victim. This congregation is great cause of delay in the working of paramedics. The response relating this interrogation was positively expressed, indicating that smooth discharge of duties by the paramedics is difficult. Furthermore, this might cause suffocation and risk to the life of the victim, due to asphyxia-related hypoxia and hypercapnia.[7]
On the query of the relation between failures of paramedics and the efficiency of doctors and EMS administration, the respondents had a positive stance. Although the doctors are clinicians with sound knowledge in their subjects, but the EMS are a matter of training and experience in both basic and an advance life support procedures, in which the doctors may not be competent. Without a perfect training of BLS and ALS, nobody can be confident about the routines of EMS. Sometimes, the referring doctors are seldom competent to decide on need for emergencies, especially the ventilation support, added oxygen, chest X-ray, airway selection. Eich et al reported that life threatening emergencies are not routine procedures for physicians who are not specialized for the job and hence, they don’t feel confident and are fearful to handle such cases.[8] The physicians need adequate training before they are exposed to such emergencies. In a study on determination of the attitudes and barriers to an established Pediatric Medical Emergency Team system among nurses and doctors, azzopardi et al[5] found that most of the doctors (47%) and nurses (32%) in the team failed to recognize serious illness, as revealed by their unwillingness. Hence any instructions and/or suggestions from the higher ups might not serve good.
The data obtained on lack of trust and confidence bestowed on paramedics clearly reveals that the staff in the higher level does not trust the work of paramedics. The reason for this lack of trust might be they being non-clinicians are ignorant of the routines of patients in wards, ICUs and NICUs. Brodsky et al were skeptical of the performance of a paramedic (a non-clinician); even to identify the simple and/or complex febrile seizure.[9] In a report Ulsenheimer found that transfer of original medical responsibilities to cheaper non-medical ancillary staff in view of the enormous pressure of costs and limited financial resources, is legally objectionable and not proper.[10] Rajabali et al reported doubts concerning the ability of paramedics to provide pre-hospital management.[11] One group of emergency physicians expressed concern in paramedics’ inability to appropriately identify ST elevation myocardial infarction on ambiguous symptoms or ECG readings, resulting in valid cases to be overlooked.
Is never allowed to take independent decisions despite of his being technically sound. For example; small children and infants do not require stretchers or ambulances for transport from a pre-hospital scene to the emergency department, unless there is a need for the equipment inside a regular ambulance. Nevertheless, the paramedic is not given the independence to decide, since non-ambulance transport cannot compromise in the system.[12] In matter related to the lack of independent decision making by the paramedics, the response was significantly positive.
Resistance by patients is considered a major interference in the working of paramedics; like in matter of intubation required for respiratory failure, the resistance by patients, is a major barrier in the performance of a paramedic.[13] This parameter in the present study showed a positive response. Furthermore, paramedics are confronted with innumerable risks in delivering emergency care to children in the field. They should be perceptive of the legal issues to avoid unnecessary litigation. They should know how best to administer proper care to the children. However, better training and sophisticated pediatric equipment will help reduce the problems.[14] On the issues of legal and litigation proceedings that interfere with the efficiency of a paramedic, the response was significantly positive.
According to the version of the respondents, the impression of general public and the family members of the patients about the paramedics are on the lowest ebb. In a report on public attitude to EMS in Singapore, Ong et al found a great discomfort of general public with paramedics, both in the punctuality of ambulance timings and efficiency in the performance of ALS intervention.[15] Despite the responsibilities of a paramedic being more technical and involve much more than merely piloting the vehicle, the layman's term for them is an ambulance driver. This is due to inadequate popularity of the tasks taken up by the paramedics, which keeps the general public and most of parents, less informative.
To conclude it is suggested that the authorities in the hospitals and EMS administration should try to improve the barriers which interferes with the efficiency of a paramedic and the health authorities should impart proper education and training to the paramedics for proper delivery of EMS to the patients. The subject of EMS should be introduced in the medical curriculum and the position of a paramedic should be changed to a medical paramedic or a clinical paramedic. The EMS protocols should be taught as a postgraduate medical diploma to the medical graduates.
Limitations of the study
The study is based on the opinion of paramedics and there is no counter opinion from the other health professionals, including nurses and doctors, hence, it might reflect a biased estimate. Nevertheless, the study provides scope for a more extensive investigation involving the views of different health professionals on paramedics.
ACKNOWLEDGMENT
The author is indebted to the Administration of King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia for providing facilities and necessary encouragement at each and every step of this study.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Bigham BL, Buick JE, Brooks SC, Morrison M, Shojania KG, Morrison LJ. Patient safety in emergency medical services: A systematic review of the literature. Prehosp Emerg Care. 2012;16:20–35. doi: 10.3109/10903127.2011.621045. [DOI] [PubMed] [Google Scholar]
- 2.Hansen TB, Dupont G. Treatment of injuries in the county of Ringkobing: Refereal and transport of severe traffic accident traumas. Ugeskr Laeger. 1992;154:3045–7. [PubMed] [Google Scholar]
- 3.Weiss SJ, Hernandez R. Emergency medical services development in the state of Louisiana. J La State Med Soc. 1994;146:389–94. [PubMed] [Google Scholar]
- 4.Pointer JE. Experience and mentoring requirements for competence in new/inexperienced paramedics. Prehosp Emerg Care. 2001;5:379–83. doi: 10.1080/10903120190939544. [DOI] [PubMed] [Google Scholar]
- 5.Azzopardi P, Kinney S, Moulden A, Tibballs J. Attitudes and barriers to a Medical Emergency Team system at a tertiary paediatric hospital. Resuscitation. 2011;82:167–74. doi: 10.1016/j.resuscitation.2010.10.013. [DOI] [PubMed] [Google Scholar]
- 6.Weiss SJ, Couk J, Nobile M, Ernst AA, Johnson W. The effect of a curfew on pediatric out-of-hospital EMS responses. Prehosp Emerg Care. 1999;2:184–8. doi: 10.1080/10903129808958869. [DOI] [PubMed] [Google Scholar]
- 7.Lee RS, Hughes RL. Prediction of human crowd pressures. Accid Anal Prev. 2006;38:712–22. doi: 10.1016/j.aap.2006.01.001. [DOI] [PubMed] [Google Scholar]
- 8.Eich C, Roessler M, Timmermann A. Out-of-hospital pediatric emergencies: Perception and assessment by emergency physicians. Anaesthesist. 2009;58:876–83. doi: 10.1007/s00101-009-1603-3. [DOI] [PubMed] [Google Scholar]
- 9.Brodsky R, Merlin MA, Leva EG, Levy RS, Leva J, Shaible J. Do all pediatric patients who have a febrile seizure require transport by advanced life support? Pediatr Emerg Care. 2009;25:317–20. doi: 10.1097/PEC.0b013e3181a34192. [DOI] [PubMed] [Google Scholar]
- 10.Ulsenheimer K. Delegation of medical responsibilities to non-medical personnel options and limits from a legal viewpoint. Unfallchirurg. 2009;112:1004–9. doi: 10.1007/s00113-009-1667-1. [DOI] [PubMed] [Google Scholar]
- 11.Rajabali NA, Tsuyuki RT, Sookram S, Simpson SH, Welsh RC. Evaluating the views of paramedics, cardiologists, emergency department physicians and nurses on advanced pre-hospital management of acute ST elevation myocardial infarction. Can J Cardiol. 2009;25:e323–e8. doi: 10.1016/s0828-282x(09)70146-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sacchetti A, Carraccio C, Feder M. Pediatric EMS transport: Are we treating children in a system designed for adults only? Pediatr Emerg Care. 1992;8:4–8. doi: 10.1097/00006565-199202000-00003. [DOI] [PubMed] [Google Scholar]
- 13.Losek JD, Bonadio WA, Walsh-Kelly C, Hennes H, Smith DS, Glaeser PW. Pre-hospital pediatric endotracheal intubation performance review. Pediatr Emerg Care. 1989;5:1–4. doi: 10.1097/00006565-198903000-00001. [DOI] [PubMed] [Google Scholar]
- 14.Selbst SM. Medical/legal issues in pre-hospital pediatric emergency care. Pediatr Emerg Care. 1988;4:276–8. doi: 10.1097/00006565-198812000-00013. [DOI] [PubMed] [Google Scholar]
- 15.Ong ME, Ang PH, Chan YH, Yap S. Public attitudes to emergency medical services in Singapore: EMS day 2002. Singapore Med J. 2004;45:419–22. [PubMed] [Google Scholar]