

Abstract
Context:
Functional performance testing of athletes can determine physical limitations that may affect sporting activities. Optimal functional performance testing simulates the athlete’s activity.
Evidence Acquisition:
A Medline search from 1960 to 2012 was implemented with the keywords functional testing, functional impairment testing, and functional performance testing in the English language. Each author also undertook independent searches of article references.
Conclusion:
Functional performance tests can bridge the gap between general physical tests and full, unrestricted athletic activity.
Keywords: functional performance tests, physical performance, power
Safe execution of athletics requires multiple components of physical performance.41,48 Physical attributes required for high-level activities include muscular strength, power, endurance, flexibility, balance, proprioception, speed, agility, and functional movement patterns (Figure 1). When athletes are injured, these physical components are less than optimal.8 A safe and expedient return to full recreational or competitive sports requires a nearly complete return of these attributes. Each component can be measured using standardized clinical testing: manual muscle, endurance, and goniometry.
Figure 1.
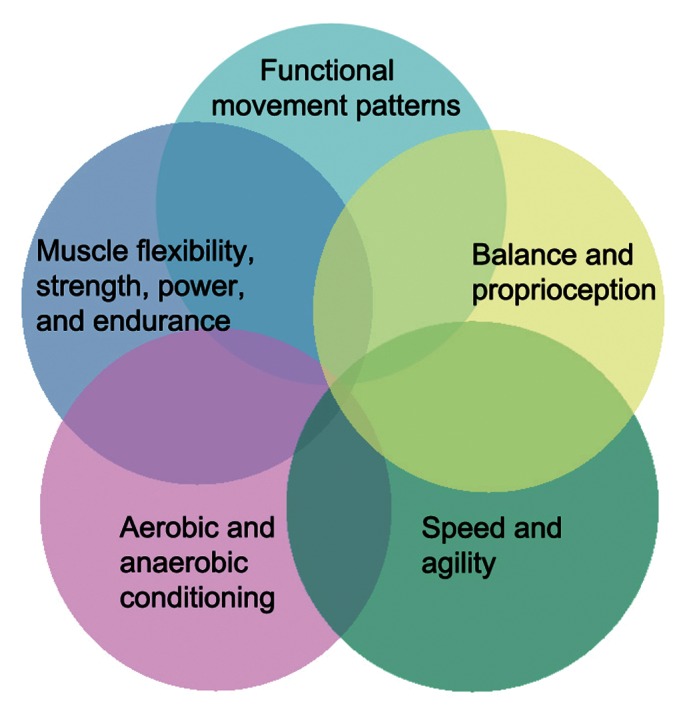
The essential components of functional testing. Reprinted with permission from Reiman and Manske.58
One of the most commonly lost physical attributes following injury is muscular power.58 Power is “the time rate of doing work,” and work is “the product of force exerted on an object and the distance the object moves in the direction in which force is exerted.”47 A powerful athlete generates force quickly.
Functional performance testing (FPT) may objectively measure progress and determine rehabilitation effectiveness as well as whether the athlete is safe to return to full sports participation.
Functional Performance Testing
A clear distinction must be made between clinical testing and FPT. FPT has multiple purposes. It can provide quantitative and qualitative information on specialized movements in sport, exercise, and occupations.58 Clinical testing is at the level of impairment, not the assessment of overall functional ability.59 It may involve anthropometric measurements of a knee joint effusion.
Test Administration
The best test of ability to return to sport is one that closely mimics that activity. For example, functional testing of a long jumper with a recently sprained ankle may involve a single-leg hop or double-leg jump test.11
Why Use Functional Performance Tests?
The controlled rehabilitation setting is ideal for FPT progression, allowing easier to harder tests.11,41-43 Inability to properly perform a single-leg hop may indicate poor static and dynamic balance, requiring impairment assessments (joint stability, strength, range of motion).
Selection of appropriate FPT requires careful consideration of safety, relevance, specificity, and practicality.58 FPT must be appropriate for the athlete’s condition, stage of injury, and abilities. In general, approximately 12 to 16 weeks is needed following soft tissue repairs before aggressive loading FPT to injured shoulders or knees.11 Therefore, a maximum single-leg hop test would not be appropriate 6 weeks following bone–patellar tendon–bone anterior cruciate ligament reconstruction.
Relevance should account for the injury, region, and sport. Closely related to relevance is specificity: muscle action, energy system, and velocity.
Sequence and Timing
In general, the most fatiguing (aerobic) FPT should be performed last, with the most explosive tests first.26,58 Aerobic or endurance exercises decrease isotonic and isokinetic muscle performance.1,39 Tests for power (vertical jump) require an energy system with a larger work-to-rest ratio.26 The phosphagen energy system is utilized in short-term, high-intensity activities.26 A work-to-rest ratio of 1:12 to 1:20 provides maximal effort using the phosphagen system of muscle recovery.26 A vertical jump takes only 2 to 3 seconds, but adequate rest is 24 to 36 seconds. A 1-mile run requires a shorter work-to-rest ratio but takes at least 4 to 5 minutes for complete recovery to occur.
Functional Testing Implementation
Before the performance of functional testing implementation, several activities should occur. Considerable debate exists as to which form of stretching is better—static or dynamic. To reduce the risk of injury, decrease postactivity muscle soreness, and create a warm-up effect before activity, some form of stretching, either static or dynamic, is recommended before maximal effort testing.
To decrease the risk of testing results improving owing to a learning effect, we recommend performance of a practice trial of functional tests. Practice sessions to familiarize athletes with the procedures aid in reproducibility and maximum effort.23,58,68,72
There are multiple ways to perform a single test. A single-leg hop for distance can be performed with hands on the hips, with hands clasped behind the back, or with hands and arms to gain momentum while hopping. Each method may allow the athlete to hop a different distance. A compensatory pattern may occur with FPT when the athlete exhibits a weakness. Using the single-leg hop, the athlete may flex excessively at the waist and hips during the eccentric phase preceding the actual hop in an effort to utilize the stronger gluteal muscles rather than the quadriceps muscles.55
Functional Performance Tests for Power
Rationale for Trunk Performance Tests
The most important trunk muscle (local and global muscles) function is providing dynamic stability.32,35 A lack of core strength and stability may predispose the athlete to injury.33 Trunk endurance is generally more important than strength for preventing low back pain. Balance of anterior, posterior, and lateral local and global trunk muscles is necessary to maintain neutral spine alignment necessary for dynamic stability.24
Trunk Power Tests
Backward Overhead Medicine Ball Throw
The athlete holds a medicine ball with arms straight in front of the body and, following a countermovement, flexes at the hips and knees before extending forcefully backward to throw the ball over the head (Figure 2). There is a strong correlation between the distance of the throw and the power index for a countermovement vertical jump (r = 0.91, P < 0.01).65 This test demonstrates high test-retest reliability (r = 0.996).65 Five to 6 trials before actual testing is best.15 The mean distance thrown by 40 intercollegiate football players was 10.41 ± 1.45 m (range, 8.17-13.85 m; test-retest reliability, 0.86).50 The absolute values were higher in male volleyball players (mean, 15.4 ± 1.1 m; range, 13.4-17.4 m) versus male wrestlers (mean, 14.2 ± 1.8 m; range, 12.2-18.8 m).65 The test results correlated with the countermovement vertical jump.65 This test is ideal to compare right to left. Ideally, right-to-left differences should be no greater than 10% to 15%.58
Figure 2.
Backward overhead medicine ball throw.
Sidearm Medicine Ball Throw
A functional test of trunk power is the sidearm medicine ball throw (Figure 3), which correlates with isometric trunk rotation torque (r = 0.60-0.74, P < 0.05-0.01) and 1-repetition maximum bench press (r = 0.68-0.73, P < 0.01).30 In elite tennis players, symmetric isokinetic trunk rotation strength correlated with trunk rotation throw based on a 2.7-kg medicine ball (r = 0.79-0.84, P < 0.01). Normative values for various groups are known.16,30
Figure 3.

Sidearm medicine ball throw.
Lower Extremity Power Tests
Power is work divided by time,47 making the velocity important. The vertical jump test can assess overall lower extremity power, bilaterally or unilaterally.
Vertical Jump
The vertical jump9,19,20,27,44,60,64 test can be done with a piece of chalk and a wall or the Vertec Vertical Jump System (Senoh, Columbus, Ohio) (Figure 4). The vertical jump test is considered a measure of explosive anaerobic power.12,66 To begin, the athlete stands with equal weight on both limbs while reaching as high as possible with a single arm. The athlete jumps or hops as high as possible (Figure 5). Taking a counterstep is the most reliable and valid field test for estimation of explosive leg power.40 The score is the distance between the first reach and the second.
Figure 4.

Starting position for vertical jump. Reprinted with permission from Reiman and Manske.58
Figure 5.
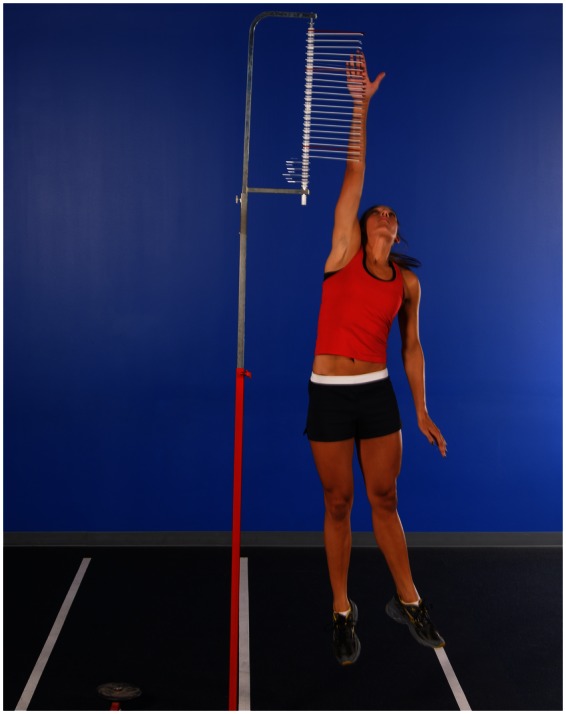
Maximum height of vertical jump. Reprinted with permission from Reiman and Manske.58
Power tests for the lower extremities should be kinematic chain tests rather than isolated tests of the hip, knee, or ankle. The vertical jump test is not an isolated assessment of knee function. The propulsive phase of vertical jump on a force plate shows that the hip contributes 40% of the total jump force; the knee, 24%; and the ankle, 36%.60 Arm swing consistently increases vertical jump height.27,40,64 Reliability of the vertical jump ranges between 0.93 and 0.99.9,19,44 In sequencing FPT, the vertical jump should be performed before standing long jump.
Vertical jump correlates well with maximal isometric peak force, 1-repetition maximum squat (recreationally trained men),46 kinematic data from ground reaction forces in eccentric and concentric phases (trained track athletes),20 knee extensor muscle strength at 40° and 90° (female athletes),62 and relative quadriceps strength (children 7-12 years old).28
Standing Long Jump
Regarding the standing long jump,13,20,43,44,69 because vertical and horizontal forces are active during takeoff and landing, this test may be more stressful than the vertical jump and should be tested later in rehabilitation. Test-retest reliability is between 0.95 and 0.96 (Figure 6).13,37,43,50,69
Figure 6.
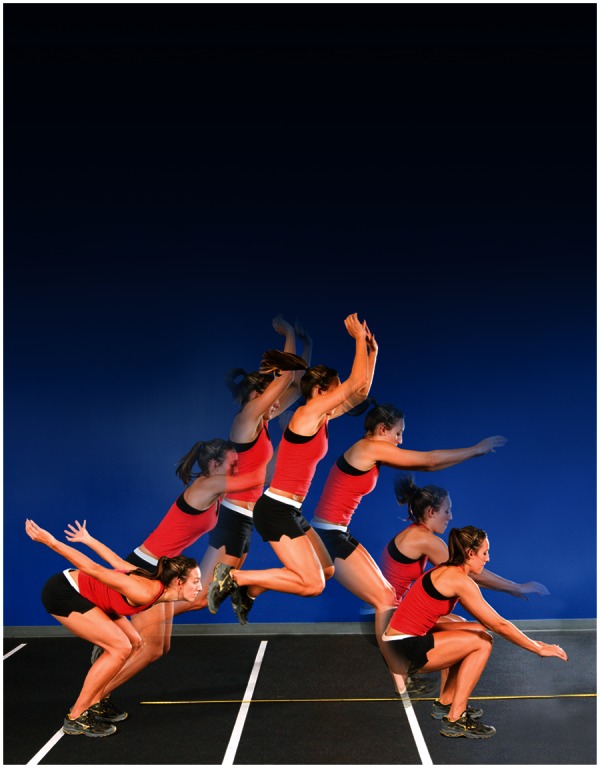
Horizontal jump for distance. Reprinted with permission from Reiman and Manske.58
Single-Leg Hop
For the single-leg hop,17,18,31,53,56,61,63,66,67,71 the score is the distance from the start to the location of the posterior heel of the landing leg (Figure 7).10 Healthy men (controls) did not differ in distance hopped, compared with the uninvolved limb of anterior cruciate ligament (ACL) patients at 13 and 54 weeks following reconstruction.56 This may be helpful because the uninvolved leg, regardless of limb dominance, can be utilized as a control when evaluating return to sports following cruciate reconstruction.56 Others have found significant differences observed between right and left limbs of athletes, suggesting that the uninjured limb cannot be used as a control.19,34,45,52,57 Regardless, the single-leg hop is simple and can be used in isolation or with a combination of quick field tests to determine knee function.17,18 Reliability for the single-leg hop test is 0.77 to 0.99.2-7,13,21,22,29,31,36,38,43,51,61,70
Figure 7.
Diagram of the single-leg hop test. Reprinted with permission from Reiman and Manske.58
Many ACL-deficient patients (42%) demonstrate abnormal limb symmetry in the single-leg hop31 (low sensitivity, 38%66 and 58%61). Recent evidence found that following ACL reconstruction, patients can exhibit impairments in the involved knee despite achieving clinically normal hop ratios. During takeoff, knee motion is 25% decreased, resulting in a 40% reduction in peak knee moment and 38% reduction in peak knee power on the involved side.54 Furthermore, during landing, knee motion was reduced by 18%, resulting in a reduction of peak power absorption by 43% on the involved side.54 Multiple factors may influence results. Balance and proprioception play important roles.63 A cluster of tests may increase test sensitivity (timed hop test).61 Combining the figure-of-8 hop, the up-down test, and the side-hop test with the single-leg hop will increase sensitivity to 82%.31 There are fair relationships of the scores of single-leg hop distance to concentric quadriceps peak torque and to scores of single-leg hop to concentric quadriceps work.14 There are moderate-to-good relationships between the single-leg hop distance and concentric quadriceps peak torque measurements for dominant and nondominant lower extremities.22,66
In the lower extremity, it can be clearly seen that each test has limitations. It is possible that a variety of tests may be needed to better determine function than any single test in isolation. Others agree that with a variety of hop tests, different hop qualities can be evaluated and, thereby, the opportunity to detect discrepancies in hop performance increases.25
Upper Extremity Power Test: Seated Shot-Put Throw
For the seated shot-put throw,49-51 to isolate the upper extremities, the athlete sits on the floor with the back against a wall (Figure 8). The score is the distance the shot is thrown. Reliability is 0.84 and 0.95 for the 10-lb shot and 0.98 for the 8-lb shot.49-51 The seated shot-put test correlates to power based on a percentage of 1-RM bench press. Loads of 30% and 60% were scored by the length of time it took to move the bench press bar through a 0.26-m distance. The test scores related to 30% (r = 0.67) and 60% (r = 0.75) bench press power in healthy college men.49 The minimal detectible change was 17 in (males) and 18 in (females).51 A 9% difference is expected between dominant and nondominant extremities in healthy, young, active participants.51
Figure 8.

Seated shot-put throw for distance.
Conclusion
Functional performance tests can help determine when an athlete can return to unrestricted activity. However, further research is desperately needed in this area to determine how adaptations during functional tests can be measured and quantified. Additionally, a lack of standardization exists, as little information is known about how various tests relate to one another and which tests are best to use in isolation or in combination as a means to assess a broad range of function. It is highly likely that performance-based function testing should utilize a wide range of assessments, including patient self- report questionnaires, assessment of psychological factors (eg, fear), and quality of movement during functional tests during assessment of return to function.
Footnotes
Robert Manske, DPT, and Michael Reiman, DPT, received roaylties from Human Kinetics for their book Functional Testing in Human Performance.
References
- 1. Abnernethy PJ. Influence of acute endurance activity on isokinetic strength. J Strength Cond Res. 1993;7:141-146 [Google Scholar]
- 2. Ageberg E, Zatterstrom R, Moritz U. Stabilimetry and one-leg hop test have high test-retest reliability. Scand J Med Sci Sports. 1998;8(4):198-202 [DOI] [PubMed] [Google Scholar]
- 3. Bandy WD, Rusche KR, Tekulve FY. Reliability and limb symmetry for five unilateral functional tests of the lower extremities. Isokin Exerc Sci. 1994;4:108-111 [Google Scholar]
- 4. Barber SD, Noyes FR, Mangine RE, McCloskey JW, Hartman W. Quantitative assessment of functional limitation in normal and anterior cruciate ligament deficient knees. Clin Orthop Relat Res. 1990;255:204-214 [PubMed] [Google Scholar]
- 5. Bolgla LA, Keskula DR. Reliability of lower extremity functional performance tests. J Orthop Sports Phys Ther. 1997;3:138-142 [DOI] [PubMed] [Google Scholar]
- 6. Booher LD, Hench KM, Worrell TW, Stikeleather J. Reliability of three single-leg hop tests. J Sport Rehabil. 1993;2:165-170 [Google Scholar]
- 7. Brosky JA, Nitz AJ, Malone TR, Caborn DNM, Rayens MK. Intrarater reliability of selected clinical outcome measures following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1999;29:39-48 [DOI] [PubMed] [Google Scholar]
- 8. Ceroni D, Martin XE, Farpour-Lampert NJ, Delhumeau C, Kaelin A. Assessment of muscular performance in teenagers after a lower extremity fracture. J Pediatr Orthop. 2010;30(8):807-812 [DOI] [PubMed] [Google Scholar]
- 9. Considine WJ, Sullivan WJ. Relationship of selected tests of leg strength and leg power in college men. Res Q. 1973;44:404-416 [PubMed] [Google Scholar]
- 10. Daniel D, Malcolm L, Stone ML, Perth H, Morgan J, Riehl B. Quantification of knee stability and function. Contemp Orthop. 1982;5:83-91 [Google Scholar]
- 11. Davies GJ, Zilmer DA. Functional progression of a patient through a rehabilitation program. Orthop Phys Ther Clin North Am. 2000;9:103-118 [Google Scholar]
- 12. Davis DS, Briscoe DA, Markowski CT, Saville SE, Taylor CJ. Physical characteristics that predict vertical jump performance in recreational male athletes. Phys Ther Sport. 2003;4:167-174 [Google Scholar]
- 13. DeCarlo MS, Sell KE. Normative data for range of motion and single-leg hop in high school athletes. J Sports Rehabil. 1997;6:246-255 [Google Scholar]
- 14. Delitto A, Irrgang JJ, Harner CD, Fu FH. Relationship of isokinetic quadriceps peak torque and work to one-legged hop and vertical jump in ACL reconstructed subjects [abstract]. Phys Ther. 1993;73:S85 [Google Scholar]
- 15. Duncan MJ, Al-Nakeeb Y. Influence of familiarization on a backward, overhead medicine ball explosive power test. Res Sports Med. 2005;13:345-352 [DOI] [PubMed] [Google Scholar]
- 16. Ellenbecker TS, Roetert EP. An isokinetic profile of trunk strength in elite tennis players. Med Sci Sports Exerc. 2004;36:1959-1963 [DOI] [PubMed] [Google Scholar]
- 17. Elliot J. Assessing muscle strength isokinetically. JAMA. 1978;240:2408-2412 [DOI] [PubMed] [Google Scholar]
- 18. Engstom B, Gornitzka J, Johansson C, Wredmark T. Knee function after anterior cruciate ligament ruptures treated conservatively. Int Orthop. 1993;17:208-213 [DOI] [PubMed] [Google Scholar]
- 19. Gioftsidou A, Ispirlidis I, Pafis G, Malliou P, Bikos C, Godalias G. Isokinetic strength training program for muscular imbalances in professional soccer players. Sports Sci Health. 2008;2:101-105 [Google Scholar]
- 20. Gonzalez-Badillo JJ, Marques MC. Relationship between kinematic factors and countermovement jump height in trained track and field athletes. J Strength Cond Res. 2010;24(12):3443-3447 [DOI] [PubMed] [Google Scholar]
- 21. Greenberger HB, Paterno MV. Relationship of knee extensor strength and hopping test performance in the assessment of lower extremity function. J Orthop Sports Phys Ther. 1995;22:202-206 [DOI] [PubMed] [Google Scholar]
- 22. Greenberger HB, Paterno MV. The test-retest reliability of a one-legged hop for distance in healthy young adults [abstract]. J Orthop Sports Phys Ther. 1994;1:S62 [Google Scholar]
- 23. Gremion G. Is stretching for sports performance still useful? A review of the literature. Rev Med Swisse. 2005;1(28):1830-1834 [PubMed] [Google Scholar]
- 24. Grenier SG, McGill SM. Quantification of lumbar stability by using 2 different abdominal activation strategies. Arch Phys Med Rehabil. 2007;88(1):54-62 [DOI] [PubMed] [Google Scholar]
- 25. Gustavsson A, Neeter C, Thomee P, et al. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg Spors Traumatol Arthrosc. 2006;14:778-788 [DOI] [PubMed] [Google Scholar]
- 26. Harman E, Pandorf C. Principles of test selection and administration. In: Baechle TR, Earle RW, eds. Essentials of Strength Training and Conditioning. 2nd ed. Champaign, IL: Human Kinetics; 2000 [Google Scholar]
- 27. Harmon E, Rosenstein M, Frykman PN, Rosentstein RM. The effects of arms and countermovement on vertical jumping. Med Sci Sports Exerc. 1990;22:825-833 [DOI] [PubMed] [Google Scholar]
- 28. Holm I, Fredriksen P, Fosdahl M, Vollestad N. A normative sample of isotonic and isokinetic muscle strength measurements in children 7 to 12 years of age. Acta Paediatr. 2008;97(5):602-607 [DOI] [PubMed] [Google Scholar]
- 29. Hu HS, Whitney SL, Irrgang J, Janosky J. Test-retest reliability of the one-legged vertical jump test and the one-legged standing hop test [abstract]. J Orthop Sports Phys Ther. 1992;15(1):S51 [Google Scholar]
- 30. Ikeda Y, Kijima K, Kawabata K, Fuchimoto T, Ito A. Relationship between side medicine-ball throw performance and physical ability for male and female athletes. Eur J Appl Physiol. 2007;99:47-55 [DOI] [PubMed] [Google Scholar]
- 31. Itoh H, Kurosaka M, Yoshiya S, Ichihashi N, Mizuno K. Evaluation of functional deficits determined by four different hop tests in patients with anterior cruciate ligament deficiency. Knee Surg Sports Traumatol Arthrosc. 1998;6:241-245 [DOI] [PubMed] [Google Scholar]
- 32. Jeffreys I. Developing a progressive core stability program. Strength Cond J. 2002;24(5):65-66 [Google Scholar]
- 33. Johnson BL, Nelson JK, eds. Practical Measurements for Evaluation in Physical Education. Minneapolis, MN: Burgess; 1979 [Google Scholar]
- 34. Jones PA, Bampouras TM. A comparison of isokinetic and functional methods of assessing bilateral strength imbalance. J Strength Cond Res. 2010;24(6):1553-1558 [DOI] [PubMed] [Google Scholar]
- 35. Kamaz M, Kiresi D, Oguz H, Emlik D, Levendogl F. CT measurement of trunk muscle areas in patients with chronic low back pain. Diagn Interv Radiol. 2007;13:144-148 [PubMed] [Google Scholar]
- 36. Keays SL, Bullock-Saxton J, Keays AC, Newcombe P. Muscle strength and function before and after anterior cruciate ligament reconstruction using semitendinosus and gracilis. Knee. 2001;8:229-234 [DOI] [PubMed] [Google Scholar]
- 37. Koch AJ, O’Bryant HS, Stone MS, et al. Effect of warm-up on the standing broad jump in trained and untrained men and women. J Strength Cond Res. 2003;17:710-714 [DOI] [PubMed] [Google Scholar]
- 38. Kramer JF, Nusca D, Fowler P, Webster-Bogaert S. Test-retest reliability of the one-leg hop test following ACL reconstruction. Clin J Sports Med. 1992;2(4):240-243 [Google Scholar]
- 39. Leveritt M, Abnernethy PJ. Acute effects of high-intensity endurance exercises on subsequent resistance activity. J Strength Cond Res. 1999; 13:47-51 [Google Scholar]
- 40. Luthanen P, Komi PV. Segmental contribution to forces in vertical jump. Eur J Appl Physiol. 1978;38:181-188 [DOI] [PubMed] [Google Scholar]
- 41. Manske RC, Davies GJ. A non-surgical approach to examination and treatment of the patellofemoral joint: part 1. Examination of the patellofemoral joint. Crit Rev Phys Rehabil Med. 2003;15:141-166 [Google Scholar]
- 42. Manske RC, Prohaska D, Livermore R. Anterior cruciate ligament reconstruction using the hamstring-gracilis tendon autograft. In: Manske RC, ed. Postsurgical Orthopedic and Sports Rehabilitation: Knee and Shoulder. St Louis, MO: Mosby; 2006:189-206 [Google Scholar]
- 43. Manske RC, Smith BS, Wyatt F. Test retest reliability of lower extremity functional tests after a closed kinetic chain isokinetic testing bout. J Sports Rehabil. 2003;12:119-132 [Google Scholar]
- 44. Markovic G, Dizdar D, Jukic I, Cardinale M. Reliability and factorial validity of squat and countermovement jump tests. J Strength Cond Res. 2004;27(6):602-608 [DOI] [PubMed] [Google Scholar]
- 45. Masuda K, Kikuhara N, Takahashi H, Yamanaka K. The relationship between muscle cross-sectional area and strength in various isokinetic movements among soccer players. J Sports Sci. 2003;21:851-858 [DOI] [PubMed] [Google Scholar]
- 46. McGuigan RM, Newton MH, Winchester JB, Nelson AG. Relationship between isometric and dynamic strength in recreationally trained men. J Strength Cond Res. 2010;24(9):2570-2573 [DOI] [PubMed] [Google Scholar]
- 47. Meriam J. Engineering Mechanics: Dynamics. Vol 2 New York, NY: Wiley; 1978 [Google Scholar]
- 48. Meyer GD, Faigenbaum AD, Chu DA, et al. Integrative training for children and adolescents: techniques and practices for reducing sports-related injuries and enhancing athletic performance. Phys Sportmed. 2011;39(1):74-84 [DOI] [PubMed] [Google Scholar]
- 49. Meyhew JL, Bemben MH, Rohrs DM, Ware J, Bemben DA. Seated shot put as a measure of upper body power in college males. J Human Mvmt Stud. 1991;21:137-148 [Google Scholar]
- 50. Meyhew JL, Bird M, Cole ML, et al. Comparison of the backward overhead medicine ball throw to power production in college football players. J Strength Cond Res. 2005;19(3):514-518 [DOI] [PubMed] [Google Scholar]
- 51. Negrete R, Hanney WJ, Kolber MJ, et al. Reliability, minimal detectable change, and normative values for tests of upper extremity function and power. J Strength Cond Res. 2010;24(12):3318-3325 [DOI] [PubMed] [Google Scholar]
- 52. Newton RU, Gerber A, Nimphius S, et al. Determination of functional strength imbalance of the lower extremities. J Strength Cond Res. 2006;20:971-977 [DOI] [PubMed] [Google Scholar]
- 53. Noyes FR, Barber SD, Mangine RE. Abnormal lower limb symmetry determined by functional hop tests after anterior cruciate ligament rupture. Am J Sports Med. 1991;19:513-518 [DOI] [PubMed] [Google Scholar]
- 54. Orishimo KF, Kremenic IJ, Mullaney MJ, McHugh MP, Nicholas SJ. Adaptations in single-leg hop biomechanics following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2010;18:1587-1593 [DOI] [PubMed] [Google Scholar]
- 55. Pandorf CE, Nindle BC, Montain SJ, et al. Reliability assessment of two military relevant occupational physical performance tests. Can J Appl Physiol. 2003;28:27-37 [DOI] [PubMed] [Google Scholar]
- 56. Petschnig R, Baron R, Albrecht M. The relationship between isokinetic quadriceps strength test and hop tests for distance and one-legged vertical jump test following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1998;28(1):23-31 [DOI] [PubMed] [Google Scholar]
- 57. Rahnama N, Lees A, Bambaecichi E. A comparison of muscle strength and flexibility between the preferred and non-preferred leg in English soccer players. Ergonomics. 2005;48:1568-1575 [DOI] [PubMed] [Google Scholar]
- 58. Reiman MP, Manske RC. Functional Testing in Human Performance. Champaign, IL: Human Kinetics; 2009 [Google Scholar]
- 59. Reiman MP, Manske RC. The assessment of function, part 1: How is it measured? A clinical perspective. J Man Manip Ther. 2011;19(2):91-99 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Robertson DG, Fleming D. Kinematics of standing broad and vertical jumping. Can J Sports Sci. 1987;12:19-23 [PubMed] [Google Scholar]
- 61. Ross MD, Langford B, Whelan PJ. Test-retest reliability of a single-leg horizontal hop test. J Strength Cond Res. 2002;16(4):617-622 [PubMed] [Google Scholar]
- 62. Rousanoglou EN, Gergiadis GV, Boudolos KD. Muscular strength and jumping performance relationships in young women athletes. J Strength Cond Res. 2008;22(4):1375-1378 [DOI] [PubMed] [Google Scholar]
- 63. Sekiya I, Muneta T, Ogiuchi T, Yagishita K, Yamamoto H. Significance of the single-legged hop test to the anterior cruciate ligament-reconstructed knee in relation to muscle strength and anterior laxity. Am J Sports Med. 1998;26:384-388 [DOI] [PubMed] [Google Scholar]
- 64. Shetty AB, Etnyre BR. Contribution of arm movement to the force components of a maximum vertical jump. J Orthop Sports Phys Ther. 1989;11:198-201 [DOI] [PubMed] [Google Scholar]
- 65. Stockbrugger BA, Haennel RG. Validity and reliability of a medicine ball explosive power test. J Strength Cond Res. 2001;15(4):431-438 [PubMed] [Google Scholar]
- 66. Swarup M, Irrgang JJ, Lephart S. Relationship of isokinetic quadriceps peak torque and work to one legged hop and vertical jump [abstract]. Phys Ther. 1992;72(6):S88 [Google Scholar]
- 67. Swearingen J, Lawrence E, Stevens J, Jackson C, Waggy C, Davis DS. Correlation of single leg vertical jump, single leg hop for distance, and single leg hop for time. Phys Ther Sport. 2011;12:194-198 [DOI] [PubMed] [Google Scholar]
- 68. Thacker SB, Gilchrist J, Stroup DF, Kimsey CD. The impact of stretching on sports injury risk: a systematic review of the literature. Med Sci Sports Exerc. 2004;36(3):371-378 [DOI] [PubMed] [Google Scholar]
- 69. Unger CL, Wooden MMJ. Effect of foot intrinsic muscle strength training on jump performance. J Strength Cond Res. 2000;14(4):373-378 [Google Scholar]
- 70. Vandermeulen D, Birmingham T, Forwell L. The test-retest reliability of a novel functional test: the lateral hop for distance. Physiotherapy Can. 2000;50(5):50-55 [Google Scholar]
- 71. Wiklander J, Lysholm J. Simple tests for surveying muscle strength and muscle stiffness in sportsmen. Int J Sports Med. 1987;8(1):50-54 [DOI] [PubMed] [Google Scholar]
- 72. Witvrouw E, Mahiew N, Danneels L, McNair P. Stretching and injury prevention: an obscure relationship. Sports Med. 2004;34(7):443-449 [DOI] [PubMed] [Google Scholar]