

Abstract
Background:
The authors investigated the correlation of protan and tritan color vision with disease characteristics in Leber hereditary optic neuropathy (LHON). The authors also characterized the therapeutic potential of idebenone in protecting patients from developing dyschromatopsia in LHON.
Methods:
Color contrast data of 39 LHON patients participating in a randomized, double-blind placebo-controlled intervention study were evaluated. Patients reported disease onset <5 years before enrolment and were genetically confirmed. Protan and tritan color contrast sensitivity was measured using a computer graphics method in patients receiving idebenone (Catena; 900 mg/d; N = 28) or placebo (N = 11) for 6 months.
Results:
Mean age of patients was 28.1 years, 87.2% were men, 76.9% carried the m11778G>A mutation, and mean duration since onset was 2 years. Assessing protan and tritan color vision at baseline revealed a high degree of color confusion even in young patients (<25 years) and with a short history of disease (<1 year). Treatment with idebenone improved tritan color vision compared with placebo (P = 0.008 at week 24); a similar trend was seen for protan. The effect of idebenone was most prominent in patients with discordant visual acuity (interocular difference of logMAR >0.2). In this subgroup, the treatment effect at week 24 was 20.4% (P = 0.005) in favor of idebenone for the tritan color domain and 13.5% (P = 0.067) for the protan domain.
Conclusion:
This study confirms that protan and tritan color confusion is an early symptom in LHON. Treatment with idebenone can protect from loss of color vision, particularly in patients who are at imminent risk of further vision loss.
Leber hereditary optic neuropathy (LHON; MIM 535000) causes progressive and mostly irreversible loss of central vision in one eye, followed by a similar loss of vision in the fellow eye within days to months (1–3). The painless loss in central visual acuity (VA) is characterized by an enlarging centrocecal scotoma and loss of color vision. Dyschromatopsia in LHON has been described predominantly as red–green (protan) defect with concomitant loss of blue–yellow (tritan) color contrast sensitivity. Dyschromatopsia results from function loss primarily in small-caliber retinal ganglion cells constituting the papillomacular bundle of the retinal nerve fiber layer (RNFL) (4,5). The smallest fibers in the retina belonging to the parvocellular neurons and mediating red–green color vision are at highest risk of functional loss in LHON (6,7). Blue–yellow color vision predominantly is carried by the koniocellular pathway, which seems to be somewhat less affected by the disease (7), explaining the subtle differences in the development of protan and tritan color confusion in LHON patients.
LHON is caused in most patients by 1 of 3 primary pathogenic mutations of the mitochondrial DNA (mtDNA: m.11778G>A, m.14484T>C, m.3460G>A), all of which affect complex I (NADH–ubiquinone–oxidoreductase) of the mitochondrial respiratory chain (1,8,9). These mutations lead to a defect of ATP synthesis accompanied by increased oxidative stress causing retinal ganglion cell dysfunction and eventually loss (10,11). Patients with the m.14484T>C mutation generally tend to have milder disease progression with a 37%–71% chance of some degree of visual improvement, whereas patients with the m.11778G>A and m.3460G>A mutations have a worse prognosis with a much lower (approximately 4%) chance of spontaneous recovery (2,12,13).
The short-chain synthetic benzoquinone idebenone (2,3-dimethoxy-5-methyl-6-(10-hydroxydecyl)-1,4-benzoquinone) was recommended in a recent expert opinion as a potential treatment for LHON (3), based on isolated case reports (14–17) and a small retrospective open-labeled study (18). The therapeutic potential of idebenone in LHON has been further investigated by our group in a randomized, double-blind placebo-controlled study (the Rescue of Hereditary Optic Disease Outpatient Study [RHODOS] (19)) and independently in a retrospective study (20). These studies confirmed the therapeutic potential of idebenone in preventing loss of vision, particularly in patients with discordant interocular VA (i.e., one eye more severely affected than the other eye) and at imminent risk of further vision loss as well as by facilitating and accelerating recovery of VA.
In this study, we investigated the red–green (protan) and blue–yellow (tritan) color contrast sensitivity, which is affected early in the course of LHON, in a subgroup of LHON patients enrolled in the RHODOS study. The first objective was to further characterize color vision in LHON patients using the baseline data from the study, particularly investigating the degree of dyschromatopsia in relation to age, disease history, and VA. The second objective was to describe the therapeutic benefit of idebenone treatment on color vision during the 6-month treatment period of the RHODOS study by comparison of the idebenone-treated group with patients receiving placebo.
METHODS
Patients
We obtained color contrast sensitivity data in a subgroup of 39 LHON patients enrolled in a prospective, randomized, double-blind placebo-controlled study (RHODOS study; ClinicalTrials.gov identifier: NCT00747487). Patients harbored 1 of 3 primary mtDNA mutations (m.11778G>A, m.14484T>C, or m.3460G>A) and had vision loss caused by LHON within 5 years before study enrolment (19). The study had ethical and institutional review board approval, and all patients gave written informed consent. Patients were stratified by disease history (onset ≤1 year vs >1 year) and mtDNA mutation and randomized to receive idebenone (Catena; Santhera Pharmaceuticals) 900 mg/d (300 mg three times a day during meals) (N = 28) or placebo (N = 11) for 24 weeks.
Color Contrast and Visual Acuity Assessments
Color contrast sensitivity was measured in the Munich center of the RHODOS study at baseline and weeks 4, 12, and 24 using a computer graphics method specifically developed for the assessment of protan and tritan color vision (21). Isoluminant colored optotypes of 4° were generated on a calibrated monitor on a white background and viewed at a distance of 1 m. The color difference between the optotypes and the white background was repeatedly altered until the threshold of visibility was obtained. Random dynamic luminance noise was superimposed on the colored optotype to mask any luminance clues in recognizing the optotype, allowing reliable detection of the red–green (protan) and blue–yellow (tritan) color confusion levels. One hundred percent on the instrument's scale is the maximal color contrast achievable with the monitor's phosphors. Normal levels of color confusion were defined as ≤6% for protan and ≤8% for tritan (21).
VA was determined with an Early Treatment Diabetic Retinopathy Study (ETDRS) chart, and color contrast data were analyzed only for patients who provided valid VA data. Patients with “off-chart” VA and only able to count fingers, detect hand motion, or light perception were assigned logarithm of the minimum angle of resolution (logMAR) values 2.0 (count fingers), 2.3 (hand motion), and 2.6 (light perception), respectively (19).
Statistical Analyses
Data were analyzed using the mixed-model repeated measures method. Treatment assignment, visit, interaction between treatment assignment and visit, and prespecified stratification factors (disease onset and mtDNA mutation) were included as fixed factors, with baseline assessment as a covariate and subject as a random factor. Graphical data presentations were generated using TIBCO Spotfire 3.2.1 software. Fisher exact test was applied for responder analyses.
RESULTS
Color Contrast Sensitivity at Baseline
The mean age of patients for whom color contrast data were obtained was 28 ± 11 (mean ± SD) years (Table 1). The majority of patients were men (87.2%) and carried the m.11778G>A mutation (76.9%). The mean time since onset of vision loss was approximately 2 years (23.5 ± 17.2 months). The mean level of color confusion was >80% for both color domains, with the majority of eyes diagnosed with color confusion >90% (Fig. 1A, B), representing a considerable deficiency in color contrast perception in this patient cohort. Only very few eyes had normal color contrast sensitivity (2.6% for protan and 6.4% for tritan). Graphical presentation of protan against tritan color confusion for all eyes showed that a higher proportion of eyes that already reached >90% color confusion in the protan domain still had residual color perception in the tritan domain (Fig. 1C). In contrast, there were only very few eyes for which residual protan color contrast sensitivity was detectable when they reached >90% color confusion in the tritan domain.
TABLE 1.
Clinical characteristics of LHON patients

FIG. 1.

Distribution of color contrast sensitivities for Leber hereditary optic neuropathy patients at baseline of the Rescue of Hereditary Optic Disease Outpatient Study show markedly elevated color confusion for protan (A) and tritan (B) color domains. C. Correlation of protan and tritan color confusion levels for all eyes (data points are slightly jittered for clarity). Note that many eyes had color confusion of >90% in both color domains resulting in a dense cluster of data points at the upper right hand corner of the graph.
High degrees of color confusion were seen for both color domains across the entire age range (Fig. 2A, B) and even young patients up to the age of 20 years had eyes with color confusion of >90%. This is also reflected by the correlation between color vision and disease duration. Although the majority of eyes with less than 30% color confusion in both tritan and protan domains were found in patients with less than 3 years since the time of diagnosis, there were already a considerable proportion of eyes with >90% color confusion within the first year of diagnosis, reflecting rapid progression of the disease (Fig. 2C, D). Loss of red–green color sensitivity seemed to be more drastic with the majority of eyes either having color contrast confusion <30% or complete loss of protan color sensitivity (>90%), which is typically reached when eyes approach logMAR 1.4 (Fig. 2E). Loss of blue–yellow color vision appeared to be more gradual, with color confusion between 30% and 80% detected for eyes having a residual VA of logMAR ≥1.4 (Fig. 2F). Interestingly, there were eyes with remaining, albeit limited, color vision in the tritan domain for patients only able to read letters from the last line of the ETDRS chart or with “off-chart” vision.
FIG. 2.

Relationship between color contrast sensitivities and age (A, B), disease duration (C, D), and visual acuity (E, F) at baseline of the Rescue of Hereditary Optic Disease Outpatient Study. Each dot represents one eye. Data are shown for the protan (A, C, D) and tritan (B, D, F) color domains. Data points in all graphs are slightly jittered for clarity.
Efficacy of Idebenone on Color Vision in LHON Patients
The decline in protan color contrast sensitivity was larger in the placebo group compared with the group of patients treated with idebenone (estimated mean difference between groups: −6.1%, P = 0.057, for week 12 and −3.9%, P = 0.239, for week 24) (Table 2). In contrast, there was a significant improvement in the tritan color contrast sensitivity in the idebenone group at 12 weeks (estimated mean difference between groups: −14.5%, P = 0.004) and 24 weeks (estimated mean difference between groups: −13.6%; P = 0.008) (Table 3).
TABLE 2.
Change in protan color contrast sensitivity (%)
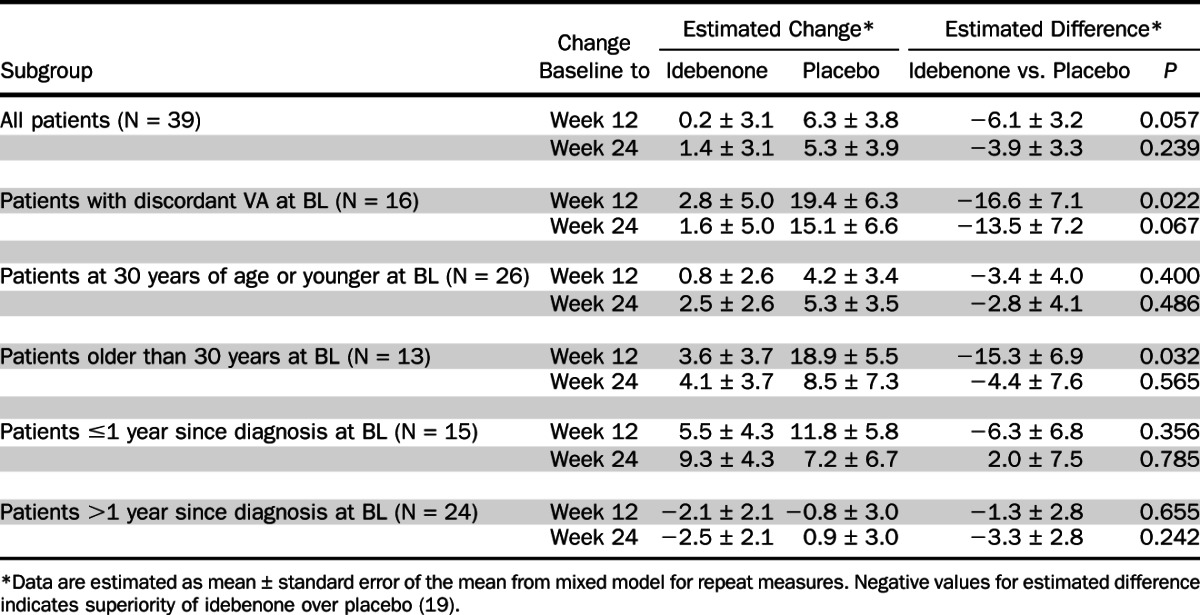
TABLE 3.
Change in tritan color contrast sensitivity (%)

Analyzing change in color vision for patients with discordant VA (defined as a difference of logMAR ≥0.2 corresponding to 2 lines on the ETDRS chart between eyes at baseline) revealed a larger difference in the change of both protan and tritan color contrast between placebo- and idebenone-treated patients at weeks 12 and 24, predominantly carried by a more profound worsening in the placebo group (Tables 2 and 3). For patients with discordant VA, there was good correlation between change in VA previously reported (19) and change in color contrast sensitivity from baseline to week 24 (correlation between change in VA and protan: R 2 = 0.532, P < 0.001; correlation between change in VA and tritan: R 2 = 0.358, P < 0.001).
Subgroup analysis showed that idebenone was particularly effective in improving tritan color vision in patients younger than 30 years. There was also better efficacy in patients with less than 1 year since diagnosis in the tritan domain, although this did not reach statistical significance, possibly because of the small number of patients in this subgroup. This trend in efficacy was not apparent for the protan color domain.
The changes in color vision between the idebenone- and placebo-treated patients also were evident by responder analyses. For both color domains, there was a higher proportion of patients with at least one eye improving in color contrast sensitivity for the idebenone group compared with the placebo group (eyes improving in color contrast sensitivity for protan: idebenone, 15 of 56 [27%] and placebo, 2 of 22 [9%], P = 0.127; for tritan: idebenone, 18 of 56 [32%] and placebo, 2 of 22 [9%], P = 0.043). Confining the analysis to patients with discordant VA showed that only idebenone-treated patients reported improved color vision (eyes improving in color contrast sensitivity for protan: idebenone, 8 of 24 [33%] and placebo, 0 of 8 [0%], P = 0.081; for tritan: idebenone, 10 of 24 [42%] and placebo, 0 of 8 [0%], P = 0.035). A similar pattern of greater benefit of idebenone over placebo also was seen for responder analyses requiring a minimum improvement of 5% or 10% in color contrast sensitivity for both protan and tritan domains (data not shown).
DISCUSSION
Impaired color vision is an early sign of visual impairment in LHON patients, often preceding loss of VA and also detectable in asymptomatic carriers of the disease (7,22). We analyzed data from acutely affected LHON patients enrolled in a prospective, randomized, and controlled intervention study to further characterize the relation of impaired red–green (protan) and blue–yellow (tritan) color vision with the patients' disease history. The majority of patients who reported symptom onset not longer than 5 years before the study had already developed considerable color confusion in both color domains. Specifically, substantial color confusion (>90%) was already seen in young patients (≤20 years of age) and in patients with short disease history (≤1 year). Taken together, these findings confirm previous observations that loss of color vision is an early pathological sign in LHON.
We recently reported the efficacy of idebenone in protecting and facilitating the recovery of VA in LHON patients participating in the placebo-controlled RHODOS study (19). In an independent retrospective study, Carelli et al (20) also reported efficacy of idebenone, particularly in recovery of vision.
The main objective of this study was to further characterize the therapeutic potential of idebenone to protect patients from developing dyschromatopsia. Idebenone is capable of shuttling electrons from the cytosol onto the complex III of the mitochondrial electron transport chain, thereby bypassing complex I, which is deficient in LHON patients (23). This is of great importance in LHON because of the high energy requirements of retinal ganglion cells and their axons, particularly for their unmyelinated sections (4,5).
The current study investigated the change in color vision in a subgroup of LHON patients enrolled in the RHODOS study. Compared with patients receiving placebo, those treated with idebenone experienced less impairment of protan color vision and a statistically significant improvement in tritan color vision. Of interest is our finding that idebenone was particularly effective in improving/preserving color vision in the subgroup of patients younger than 30 years and in recently diagnosed patients (<1 year since diagnosis). This finding likely reflects the known better potential for recovery in younger-onset LHON patients and the benefit of earlier treatment of the disease. The RHODOS study allowed enrollment of patients diagnosed as long as 5 years earlier, resulting in a mean time since disease onset of approximately 2 years. From the natural history of the disease, it can be expected that the majority of patients will already have optic atrophy and loss of retinal ganglion cells, resulting in a smaller likelihood of benefit, which may have diluted the overall therapeutic effect. Detecting efficacy of idebenone even in this heterogeneous LHON population is therefore remarkable.
Idebenone also appeared very effective in protection from loss of VA in patients with discordant interocular vision, defining patients at highest risk of further vision loss (19). This effect of idebenone in patients with discordant VA was also seen for both protan and tritan color vision.
The anatomical substrate underlying the preservation of color vision (and VA) in idebenone-treated patients might be stabilization of RNFL thickness. In untreated LHON patients, initial swelling of the RNFL is followed by atrophic thinning, particularly affecting the papillomacular bundle (24,25). This dynamic change in RNFL thickness in LHON patients possibly reflects the progressive metabolic crisis occurring in small-diameter retinal ganglion cells. Idebenone preserved the RNFL thickness in patients with a short disease history (i.e. <6 months from symptom onset) (19), which is reflected in better preserved VA and color vision. Patients receiving placebo experienced atrophy of the RNFL in the inferior and superior quadrants associated with vision loss and dyschromatopsia. These findings suggest that for maximal benefit, patients with LHON should be treated with idebenone early in their clinical course.
ACKNOWLEDGMENTS
The authors thank Nick Coppard and Günther Metz (both Santhera Pharmaceuticals) for help in the interpretation of the data, and Professor Geoffrey Arden for very valuable discussions on methods and results of this study. The authors are indebted to the patients who volunteered for this study and they also thank all doctors who have transferred patients into this trial.
Footnotes
Address correspondence to Thomas Klopstock, MD, Department of Neurology, Friedrich-Baur-Institute, Ludwig-Maximilians-University, 80336 Munich, Germany; E-mail: tklopsto@med.lmu.de
Supported by Santhera Pharmaceuticals (Liestal, Switzerland), the sponsor of the study, and by the German Ministry of Education and Research (BMBF, Bonn, Germany) grant number 01GM0862 to the German network for mitochondrial disorders (mitoNET).
Recruiting of patients was supported by use of the patient registry of the German network for mitochondrial disorders (mitoNET), which is funded by the German Ministry of Education and Research (BMBF, Bonn, Germany) grant number 01GM0862.
C. Rummey and T. Meier are regular employees of Santhera Pharmaceuticals (Liestal, Switzerland), the sponsor of the study. T. Klopstock received research support for this and other studies from Santhera Pharmaceuticals. He also has received research support from government entities (Deutsche Forschungsgemeinschaft, Bundesministerium für Bildung und Forschung, European Commission 7th Framework Programme) and from commercial entities (Santhera Pharmaceuticals; Actelion Pharmaceuticals, Ltd; H. Lundbeck A/S). T. Klopstock serves on scientific advisory boards for commercial entities (Santhera Pharmaceuticals; Actelion Pharmaceuticals, Ltd) and for nonprofit entities (Center for Rare Diseases, Bonn, Germany; Hoffnungsbaum e.V., Germany). He has received speaker honoraria and travel costs from commercial entities (Dr. Willmar Schwabe GmbH & Co. KG; Eisai Japan; Santhera Pharmaceuticals; Actelion Pharmaceuticals, Ltd) and performs consultancies for the Gerson Lehrman Group, USA.
REFERENCES
- 1. Yu-Wai-Man P, Griffiths PG, Chinnery PF. Mitochondrial optic neuropathies—disease mechanisms and therapeutic strategies. Prog Retin Eye Res. 2011; 30: 81– 114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Fraser JA, Biousse V, Newman NJ. The neuro-ophthalmology of mitochondrial disease. Surv Ophthalmol. 2010; 55: 299– 334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Sadun AA, La Morgia C, Carelli V. Leber's hereditary optic neuropathy. Curr Treat Options Neurol. 2011; 13: 109– 117 [DOI] [PubMed] [Google Scholar]
- 4. Carelli V, Ross-Cisneros FN, Sadun AA. Mitochondrial dysfunction as a cause of optic neuropathies. Prog Retin Eye Res. 2004; 23: 53– 89 [DOI] [PubMed] [Google Scholar]
- 5. Sadun AA, Win PH, Ross-Cisneros FN, Walker SO, Carelli V. Leber's hereditary optic neuropathy differentially affects smaller axons in the optic nerve. Trans Am Ophthalmol Soc. 2000; 98: 223– 232 [PMC free article] [PubMed] [Google Scholar]
- 6. Grigsby SS, Vingrys AJ, Benes SC, King-Smith PE. Correlation of chromatic, spatial, and temporal sensitivity in optic nerve disease. Invest Ophthalmol Vis Sci. 1991; 32: 3252– 3262 [PubMed] [Google Scholar]
- 7. Ventura DF, Gualtieri M, Oliveira AGF, Costa MF, Quiros P, Sadun F, de Negri AM, Salomao SR, Berezovsky A, Sherman J, Sadun AA, Valerio Carelli V. Male prevalence of acquired color vision defects in asymptomatic carriers of Leber's hereditary optic neuropathy. Invest Ophthalmol Vis Sci. 2007; 48: 2362– 2370 [DOI] [PubMed] [Google Scholar]
- 8. Harding AE, Sweeney MG, Govan GG, Riordan-Eva P. Pedigree analysis in Leber hereditary optic neuropathy families with a pathogenic mtDNA mutation. Am J Hum Genet. 1995; 57: 77– 86 [PMC free article] [PubMed] [Google Scholar]
- 9. Riordan-Eva P, Sanders MD, Govan GG, Sweeney MG, Da Costa J, Harding AE. The clinical features of Leber's hereditary optic neuropathy defined by the presence of a pathogenic mitochondrial DNA mutation. Brain. 1995; 118: 319– 337 [DOI] [PubMed] [Google Scholar]
- 10. Zanna C, Ghelli A, Porcelli AM, Martinuzzi A, Carelli V, Rugolo M. Caspase-independent death of Leber's hereditary optic neuropathy cybrids is driven by energetic failure and mediated by AIF and endonuclease G. Apoptosis. 2005; 10: 997– 1007 [DOI] [PubMed] [Google Scholar]
- 11. Baracca A, Solaini G, Sgarbi G, Lenaz G, Baruzzi A, Schapira AHV, Martinuzzi A, Carelli V. Severe impairment of complex I-driven adenosine triphosphate synthesis in Leber hereditary optic neuropathy cybrids. Arch Neurol. 2005; 62: 730– 736 [DOI] [PubMed] [Google Scholar]
- 12. Yu-Wai-Man P, Griffiths PG, Hudson G, Chinnery PF. Inherited mitochondrial optic neuropathies. J Med Genet. 2009; 46: 145– 158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Spruijt L, Kolbach DN, de Coo RF, Plomp A, Bauer NJ, Smeets HJ, De Die-Smulders C. Influence of mutation type on clinical expression of Leber hereditary optic neuropathy. Am J Ophthalmol. 2006; 141: 676– 682 [DOI] [PubMed] [Google Scholar]
- 14. Mashima Y, Hiida Y, Oguchi Y. Remission of Leber's hereditary optic neuropathy with idebenone. Lancet. 1992; 340: 368– 369 [DOI] [PubMed] [Google Scholar]
- 15. Carelli V, Barboni P, Zacchini A, Mancini R, Monari L, Cevoli S, Liguori R, Sensi M, Lugaresi E, Montagna P. Leber's hereditary optic neuropathy (LHON) with 14484/ND6 mutation in a North African patient. J Neurol Sci. 1998; 160: 183– 188 [DOI] [PubMed] [Google Scholar]
- 16. Carelli V, Valentino ML, Liguori R, Meletti S, Vetrugno R, Provini F, Mancardi GL, Bandini F, Baruzzi A, Montagna P. Leber's hereditary optic neuropathy (LHON/11778) with myoclonus: report of two cases. J Neurol Neurosurg Psychiatry. 2001; 71: 813– 816 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Cortelli P, Montagna P, Pierangeli G, Lodi R, Barboni P, Liguori R, Carelli V, Iotti S, Zaniol P, Lugaresi E, Barbiroli B. Clinical and brain bioenergetics improvement with idebenone in a patient with Leber's hereditary optic neuropathy: a clinical and 31P-MRS study. J Neurol Sci. 1997; 148: 25– 31 [DOI] [PubMed] [Google Scholar]
- 18. Mashima Y, Kigasawa K, Wakakura M, Yoshihisa O. Do idebenone and vitamin therapy shorten the time to achieve visual recovery in Leber hereditary optic neuropathy? J Neuroophthalmol. 2000; 20: 166– 170 [DOI] [PubMed] [Google Scholar]
- 19. Klopstock T, Yu-Wai-Man P, Dimitriadis K, Rouleau J, Heck S, Bailie M, Atawan A, Chattopadhyay S, Schubert M, Garip A, Kernt M, Petraki D, Rummey C, Leinonen M, Metz G, Griffiths PG, Meier T, Chinnery PF. A randomized placebo-controlled trial of idebenone in Leber's hereditary optic neuropathy. Brain. 2011; 134: 2677– 2686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Carelli V, La Morgia C, Valentino ML, Rizzo G, Carbonelli M, De Negri AM, Sadun F, Carta A, Guerriero S, Simonelli F, Sadun AA, Aggarwal D, Liguori R, Avoni P, Baruzzi A, Zeviani M, Montagna P, Barboni P. Idebenone treatment in Leber's hereditary optic neuropathy. Brain. 2011; 134: e188. [DOI] [PubMed] [Google Scholar]
- 21. Arden GB, Wolf JE. Colour vision testing as an aid to diagnosis and management of age related maculopathy. Br J Ophthalmol. 2004; 88: 1180– 1185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Quiros PA, Torres RJ, Salomao S, Berezovsky A, Carelli V, Sherman J, Sadun F, De Negri A, Belfort R, Sadun AA. Colour vision defects in asymptomatic carriers of the Leber's hereditary optic neuropathy (LHON) mtDNA 11778 mutation from a large Brazilian LHON pedigree: a case-control study. Br J Ophthalmol. 2006; 90: 150– 153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Haefeli RH, Erb M, Gemperli AC, Robay D, Courdier-Fruh I, Anklin C, Dallmann R, Gueven N. NQO1-dependent redox cycling of idebenone: effects on cellular redox potential and energy levels. PLoS One. 2011; 6: e17963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Barboni P, Savini G, Valentino ML, Montagna P, Cortelli P, De Negri AM, Sadun F, Bianchi S, Longanesi L, Zanini M, di Vivo A, Carelli V. Retinal nerve fiber layer evaluation by optical coherence tomography in Leber's hereditary optic neuropathy. Ophthalmology. 2005; 112: 120– 126 [DOI] [PubMed] [Google Scholar]
- 25. Barboni P, Carbonelli M, Savini G, do Ramos C, Carta A, Berezovsky A, Salomao SR, Carelli V, Sadun AA. Natural history of Leber's hereditary optic neuropathy: longitudinal analysis of the retinal nerve fiber layer by optical coherence tomography. Ophthalmology. 2010; 117: 623– 627 [DOI] [PubMed] [Google Scholar]