

Abstract
Purpose
To evaluate the prevalence of bladder neck contracture (BNC) and its risk factors in patients undergoing radical prostatectomy in Korea.
Materials and Methods
We analyzed data from 488 patients with prostatic cancer who underwent radical prostatectomy performed by seven surgeons in seven hospitals, including 365 open radical prostatectomies (ORPs), 99 laparoscopic radical prostatectomies (LRPs), and 24 robot-assisted laparoscopic radical prostatectomies (RARPs). Patients with BNCs were compared with those without BNCs to identify the risk factors for BNC occurrence.
Results
Overall, BNCs occurred in 21 of 488 patients (4.3%): 17 patients (4.7%) who underwent ORP, 4 patients (4%) who underwent LRP, and no patients who underwent RARP. In the univariate analysis, men with BNCs had a longer length of time before drain removal (12 days vs. 6.8 days, p<0.001), which reflected urinary leakage through the vesicourethral anastomosis. In the multivariate analysis, the length of time before drain removal was the only predictor of BNC (odds ratio, 1.12; p=0.001). Intraoperative blood loss was higher in patients with BNC, but the difference was not statistically significant.
Conclusions
The most significant factor related to BNC occurrence after radical prostatectomy in our study was the length of time before drain removal, which reflects urinary leakage from the vesicourethral anastomosis. The proper formation of a watertight anastomosis to decrease urinary leakage may help to reduce the occurrence of BNC.
Keywords: Prostate neoplasms, Prostatectomy, Urinary bladder neck obstruction
INTRODUCTION
The prevalence of prostate cancer increases with age [1]. Fortunately, screening using prostate-specific antigen (PSA) and transrectal prostate biopsies enables the early diagnosis and treatment of prostate cancer. In addition, surgical treatments for localized prostate cancer are associated with safe and favorable outcomes [2], and the proactive surgical treatment of prostate cancer is encouraged worldwide.
The prevalence of bladder neck contracture (BNC), one of the most common complications of prostate cancer surgery, is reported to be variable. In the 1990s, its prevalence was as high as 30% [3], but the prevalence has been reduced to 2.0% to 5.0% through advancements in surgical techniques and the introduction of new surgical methods, including robot-assisted laparoscopic radical prostatectomy (RARP) and pure laparoscopic radical prostatectomy (LRP) [4-6]. However, even though the prevalence of BNC has been reduced dramatically, when it does occur, BNC markedly reduces the quality of life of patients, and endoscopic operative procedures such as transurethral bladder neck incisions must be performed in cases refractory to metal sound dilation [7].
Although several factors have been hypothesized to cause BNC, its etiology remains controversial. There are few studies of BNC in Asian populations, including Koreans. In this study, therefore, we aimed to identify the prevalence and risk factors of BNC after radical prostatectomy in Koreans.
MATERIALS AND METHODS
This study was conducted as a retrospective research study in 488 patients with prostate cancer who underwent radical prostatectomy at 7 different hospitals from January 2004 to December 2008. The patient data were collected for analysis from 7 hospitals with the approval of each hospital's Institutional Review Board.
In all patients undergoing open radical prostatectomy (ORP) through the retroperitoneal approach, vesicourethral anastomosis (VUA) was performed with six interrupted sutures. If any leakage was identified during saline injection through the Foley catheter, additional sutures were added. In patients undergoing LRP and RARP, a double-armed 3-0 monofilament suture was performed in a running fashion for VUA, and parachute reconstruction of the bladder neck was done without mucosal eversion. With saline irrigation, the anastomosis was confirmed to be watertight. The retroperitoneal approach was used in all RARP procedures, and LRP was performed through the retroperitoneal or transperitoneal approach.
Cystography was performed 14 to 21 days after the surgery, and when VUA healing was confirmed, the Foley catheter was removed. If the amount of fluid discharged through the drain was ≤30 mL/d, the anastomosis was considered healed and the Jackson-Pratt drain was removed.
During a follow-up visit, uroflowmetry and postvoiding residual urine measurement were performed in patients who complained of obstructive voiding symptoms. If a low maximum urinary flow rate or large amounts of residual urine were identified, diagnostic cystoscopy was performed. If it was challenging to advance the 18-Fr cystoscope into the bladder, the patient was diagnosed with BNC. Metal sound dilatation was performed to manage mild BNC. Patients who were refractory to sound dilatation were treated by means of a cold knife endoscopic incision.
Differentiated data were collected and analyzed in the four categories (Table 1).
TABLE 1.
Differentiated parameters for analysis
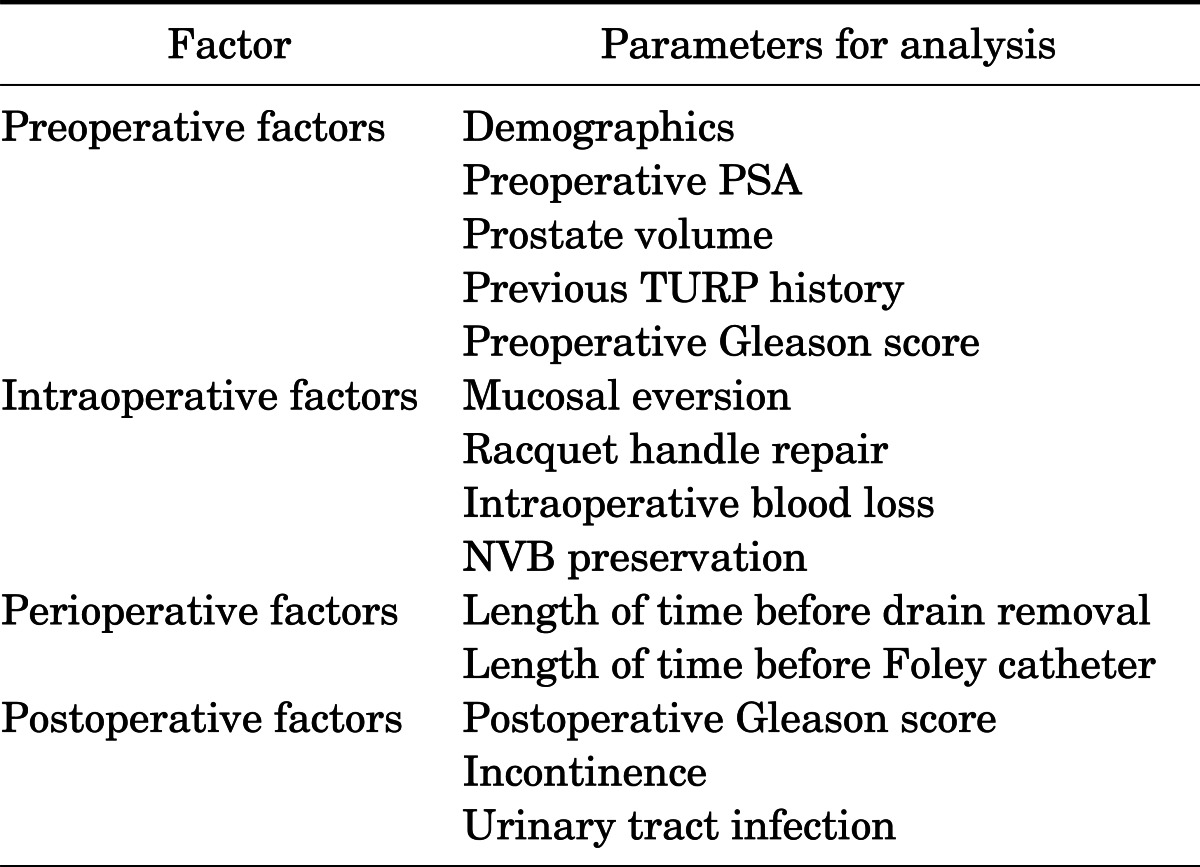
PSA, prostate-specific antigen; TURP, transurethral resection of prostate; NVB, neurovascular bundle.
1. Statistical analysis
Univariate analyses (Student's t-test, Mann-Whitney's U test, Fisher's exact test) were conducted for variables. Multiple logistic regression analyses by dummy variables were used to identify the effects of operative method, neurovascular bundle (NVB) preservation, racquet handle repair, mucosal eversion, intraoperative blood loss, and length of time before drain removal on the occurrence of BNC. Values of p<0.05 were considered statistically significant.
RESULTS
The patients' baseline data are presented in Table 2. No significant differences in baseline characteristics were found between patients treated by ORP, LRP, or RARP. The mean follow-up period was 32.4 months (range, 9 to 62 months).
TABLE 2.
Demographics and rate of occurrence of BNC of patients who underwent radical prostatectomy

Values are presented as number (%) or mean±standard deviation.
BNC, bladder neck contracture; ORP, open radical prostatectomy; LRP, laparoscopic radical prostatectomy; RARP, robot-assisted laparoscopic radical prostatectomy; PSA, prostate-specific antigen.
a:For the comparison between ORP and LRP and RARP.
A total of 488 patients participated in this study. BNC occurred in 21 patients (4.3%) in total: 17 patients (4.7%) who underwent ORP, 4 patients (4.0%) who underwent LRP, and 0 patients who underwent RARP. When the 21 patients with BNC were compared with the patients without BNC, the length of time before drain removal, which reflects postoperative urine leakage from the VUA, was significantly longer in the BNC group (12 days) than in the BNC-negative group (6.8 days). However, there were no significant differences in other variables (Table 3). The multivariate analysis also showed that the length of time before drain removal was the only predictor of BNC (odds ratio [OR], 1.12; p=0.001) (Table 4). The mean time after RP for BNC occurrence was 8.5±11.5 months (range, 1.7 to 48.7 months).
TABLE 3.
Univariate analysis of risk factors for BNC
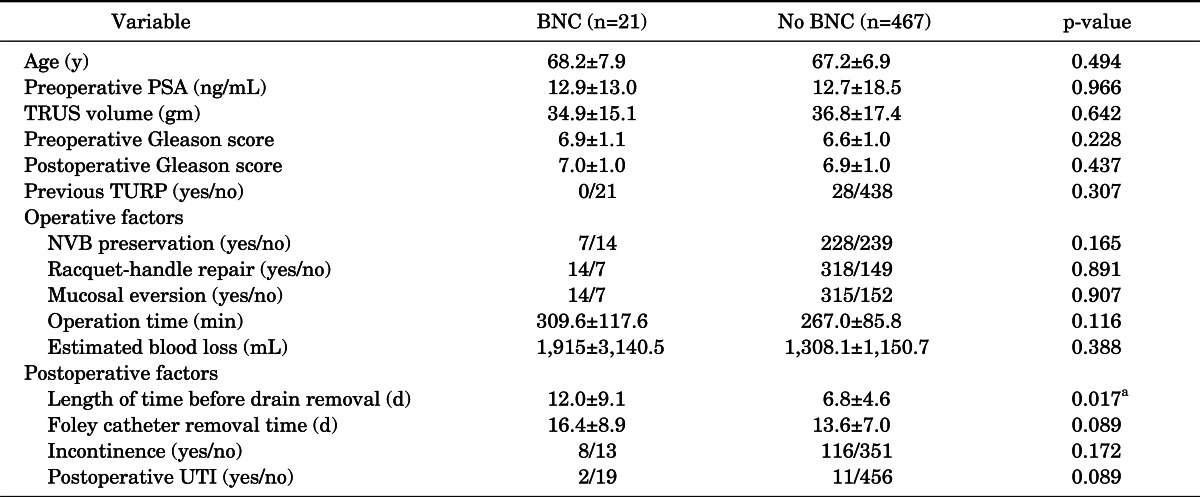
Values are presented as mean±standard deviation.
BNC, bladder neck contracture; PSA, prostate-specific antigen; TRUS, transrectal ultrasound; TURP, transurethral resection of prostate; NVB, neurovascular bundle; UTI, urinary tract infection.
a:p-value<0.05.
TABLE 4.
Multiple logistic regression analysis by dummy variables
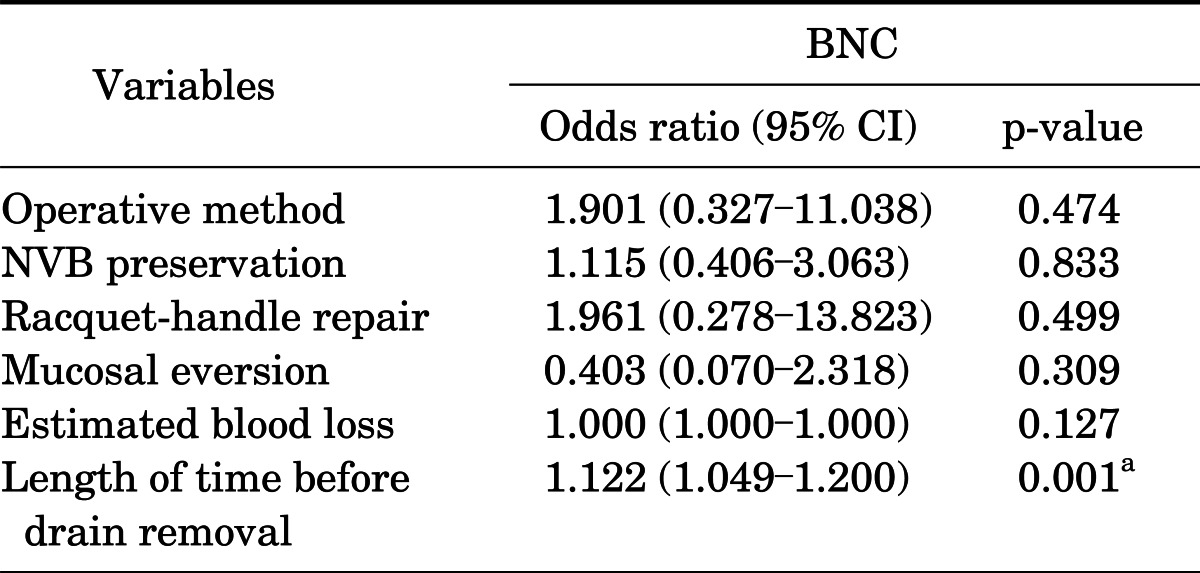
BNC, bladder neck contracture; CI, confidence interval; NVB, neurovascular bundle.
a:p-value<0.005.
In the patients who had undergone ORP, BNC occurred in 17 of 365 patients (4.7%). The length of time before drain removal was significantly longer in the BNC group (11.9 days) than in the BNC-negative group (6.7 days, p=0.017). The amount of intraoperative blood loss was 2,126 mL in the BNC group and 1,487 mL in the BNC-negative group, but the difference was not statistically significant (p=0.916). A total of 25 of 348 patients (7.2%) in the BNC-negative group had previously undergone TURP, whereas no patients in the BNC group had previously undergone TURP (p=0.618). The operative time in the BNC group was longer than in the BNC-negative group (273.6 minutes vs. 250.8 minutes), but the difference was not significant (p=0.308) (Table 4). The multivariate analysis indicated that the time before drain removal was the only parameter with effects on BNC occurrence (OR, 1.199; p<0.001).
In the patients who had undergone LRP or RARP, 4 of 99 patients (4.0%) who underwent LRP and 0 of 24 patients who underwent RARP had BNC. The length of time before drain removal was longer in the BNC group than in the BNC-negative group (12.3 days vs. 7.2 days, p=0.027). The operation time of the BNC group was also longer than that in the BNC-negative group (462.5 minutes vs. 314.3 minutes, p=0.003). However, according to the results of the multivariate analysis, operation time was the only significant predictor of BNC occurrence (OR, 1.013; p=0.017). BNC did not occur in the four patients who had previously undergone TURP (Table 5).
TABLE 5.
Univariate analysis of risk factors for BNC after radical prostatectomy depending on urgical method
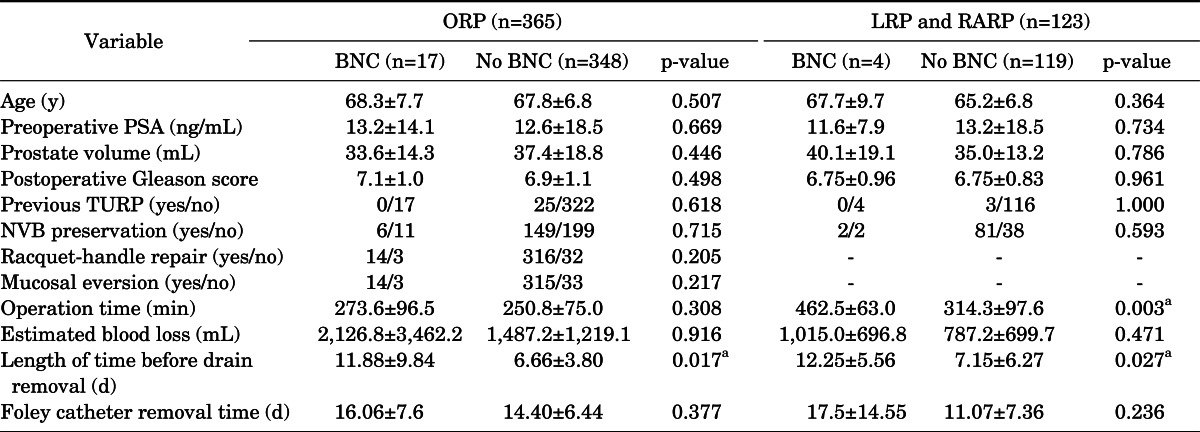
Values are presented as mean±standard deviation.
BNC, bladder neck contracture; ORP, open radical prostatectomy; LRP, laparoscopic radical prostatectomy; RARP, robot-assisted laparoscopic radical prostatectomy; PSA, prostate-specific antigen; TURP, transurethral resection of prostate; NVB, neurovascular bundle.
a:p-value<0.05, racquet-handle repair and mucosal eversion were not performed for any LRP or RARP.
DISCUSSION
In the present study, the rate of occurrence of BNC was 4.3%, and there was no significant difference in BNC occurrence between ORP and LRP patients. The rate of occurrence of BNC in patients undergoing ORP was similar to the results of studies conducted after 2000 [4,8,9], but the rate of occurrence in patients undergoing LRP was higher than in previous studies [10].
The length of time before drain removal, which reflects postoperative urine leakage from the VUA site, was a significant risk factor affecting the occurrence of BNC in all patients. Urinary leakage through the anastomotic gap delays healing of the suture site, while also causing BNC by inducing the proliferation of myofibroblast cells and wound contracture [11]. Several previous studies have also suggested urinary extravasation as a risk factor for BNC occurrence [12,13]. However, controversies remain. Huang and Lepor [14] reported that the degree of urinary extravasation on cystography was not related to BNC, and Hanson et al. [15] found that the amount of postoperative drain output is not associated with BNC occurrence . However, we thought that the length of time of urinary leakage may have a greater influence on wound contracture than extravasation degree on cystography or amount of leaked urine.
Significant intraoperative blood loss results in poor visualization of the surgical field, thus complicating mucosa-to-mucosa anastomosis of VUA. The presence of blood is also likely to cause BNC by inducing tissue inflammatory responses at the anastomosis site. Surya et al. [12] demonstrated that excessive intraoperative blood loss at the VUA increased BNC occurrence in a study of 156 patients undergoing RRP. Kostakopoulos et al. [13] showed that intraoperative blood loss greater than 1,000 mL was related to increased BNC. In the present study, the amount of intraoperative blood loss was greater than in previous studies, but the rate of BNC occurrence was similar. Although patients with BNC seemed to experience greater intraoperative blood loss, the difference was not statistically significant (p=0.387). We suggest that effort to guarantee direct visualization and additional sutures of the VUA, if needed, could improve watertight mucosal to mucosal anastomosis, which could then lessen the effect of excessive intraoperative blood loss.
Watertight VUA is the most important and the most challenging part of radical prostatectomy and is considered to be the most crucial factor predicting postoperative BNC. Technical modifications and efforts to ensure proper VUA have been introduced. According to a study that analyzed 4,132 cases performed by one surgeon from 1983 to 2007, the initial BNC occurrence rate was nearly 17% but was dramatically reduced over time as the surgeon became more experienced. The rate was as low as 1% for the final 500 cases. During the initial period, the surgeon had used only four sutures for VUA but later began to make five sutures at the 2, 4, 6, 8, and 10 o'clock positions in order to reduce anastomotic leak [16]. In another study, Orvieto et al. [17] showed that the rate of occurrence of BNC was 5.7% before 2000 and was reduced to 0.2% after 2000 among 977 cases when the following modifications were applied: 1) reconstruction of the bladder neck to a diameter of 28 French; 2) placement of a posterior (6 o'clock) vesicourethral suture during mild traction before placing this suture into the bladder, allowing inspection and, if necessary, replacement of any of the previously placed sutures; and 3) bladder displacement when tying the vesicourethral sutures, which allows the sutures to be tied under direct visual observation. In those studies, technical modification and efforts to complete proper watertight anastomosis of VUA resulted in reduced BNC occurrence. In the present study, an additional suture was added to the routine six sutures at the VUA site to reduce urinary leakage under direct visualization. Although it was not possible to analyze the effects of accumulation of experience or additional sutures on the reduction of urine leakage or the occurrence of BNC, we did observe that decreased urinary leakage at watertight VUA sites was related to reduced BNC occurrence.
In previous studies that compared ORP with LRP or RARP, the rate of occurrence of BNC from LRP or RARP was reported to be lower than that from ORP [8,9,18]. The magnification of visualization and excellent movement of the device inside the narrow pelvic cavity in LRP and RARP enables the surgeon to more easily and effectively conduct VUA, and the running suture technique for VUA could be helpful for decreasing the rate of urinary leakage. Rassweiler et al. [19] reported that postoperative cystography performed 7 days after surgery showed that 90% of patients had a watertight anastomosis, which was significantly higher than the 69.4% of patients who had watertight anastomosis after ORP. They also reported that it was possible to remove the catheter at 3 days postoperatively, in contrast with the 14 to 21 days after ORP. Nadu et al. [20] demonstrated that postoperative cystography at 2 to 4 days after LRP showed that 85% of patients had a watertight anastomosis, and that no anatomic strictures occurred in any patients. The possible explanation for the higher success rate of watertight VUA in the RARP and LRP groups is that a running anastomosis under better visualization may result in reduced urine extravasations.
In the present study, in the univariate and multivariate analyses of BNC occurrence, these operation methods were not significant as risk factors for BNC. The rate of occurrence of BNC was 3.6% in patients who underwent LRP or RARP (4.0% in patients who underwent LRP and 0% in patients who underwent RARP). BNC occurred in 1 of 18 patients (5.6%) who underwent LRP during the early experience of the surgeon, and the rate of occurrence gradually decreased over time, reaching 2.6% (1/37) in 2008 (p=0.572). In the 25 patients who had undergone RARP, despite surgeries performed by inexperienced surgeons, no BNC occurred.
According to a study by Msezane et al. [6], among 634 RARP cases, BNC occurred in 7 patients (1.1%) and the operation time was significantly longer in the BNC group than in the non-BNC group (283 minutes vs. 225 minutes). The authors suggested longer operative time with steep Trendelenburg position and pneumoperitoneal pressure of 14 to 20 mmHg could result in local tissue ischemia and subsequent BNC occurrence. In the present study, the patients who underwent LRP and those who underwent RARP showed differences in operation time as well as the length of time before drain removal. However, only the operation time was significantly different in the multivariate analysis. The number of LRP and RARP cases in the present study was too small to identify statistical significance for operation time. Furthermore, each surgeon performed cystography at different times, so we could not compare the length of time that it took for the anastomosis to become watertight after ORP, LRP, and RARP.
NVB preservation plays an important role in aiding the recovery of potency and continence after radical prostatectomies [21,22] and also prevents unnecessary removal of periurethral tissues that carry the blood supply to the VUA while dissecting the apex of the prostate for NVB preservation. Erickson et al. [16] analyzed 4,132 ORP cases performed from 1983 to 2007 and reported that during a mean follow-up period of 44 months, BNC occurred in 110 patients (2.5%). A lack of NVB preservation or surgery prior to 1992 were significant risk factors for BNC, and the prevalence of erectile dysfunction and incontinence was significantly higher in patients with BNC. In the present study, NVB preservation was achieved in 48.4% of all patients, and BNC occurred in 5.2% of patients without NVB preservation compared with 3% of those who had NVB preservation, but this difference was not statistically significant.
Our study did have several limitations. First, this study was performed retrospectively; thus, the rate of occurrence of BNC could be underestimated owing to undetected BNC. Second, we used the length of time before drain removal as a marker of urinary leakage, but fluid from the drain also contained blood, lymphatics, and peritoneal fluid, particularly in RARP and LRP. Thus, it was possible to overestimate VUA leakage. Surgeons tried to reduce this inaccuracy by estimating fluid creatinine levels and other blood profiles. In addition, because the number of LRP and RARP operations was small, and the number of patients with BNC was also low, it was difficult to analyze the rates of occurrence of BNC according to operative method.
CONCLUSIONS
Postradical prostatectomy BNC occurred in 4.3% of patients in the present study, and the most significant factor related to BNC occurrence was the length of time before drain removal, which in turn reflects urinary leakage from the anastomosis site. Urinary leakage can be prevented by elaborate and meticulous anastomosis of the bladder neck and urethra, thereby reducing the frequency of BNC.
Footnotes
The authors have nothing to disclose.
References
- 1.Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000: the global picture. Eur J Cancer. 2001;37(Suppl 8):S4–S66. doi: 10.1016/s0959-8049(01)00267-2. [DOI] [PubMed] [Google Scholar]
- 2.Joniau S, Hsu CY, Gontero P, Spahn M, Van Poppel H. Radical prostatectomy in very high-risk localized prostate cancer: long-term outcomes and outcome predictors. Scand J Urol Nephrol. 2012;46:164–171. doi: 10.3109/00365599.2011.637956. [DOI] [PubMed] [Google Scholar]
- 3.Tomschi W, Suster G, Holtl W. Bladder neck strictures after radical retropubic prostatectomy: still an unsolved problem. Br J Urol. 1998;81:823–826. doi: 10.1046/j.1464-410x.1998.00660.x. [DOI] [PubMed] [Google Scholar]
- 4.Roumeguere T, Bollens R, Vanden Bossche M, Rochet D, Bialek D, Hoffman P, et al. Radical prostatectomy: a prospective comparison of oncological and functional results between open and laparoscopic approaches. World J Urol. 2003;20:360–366. doi: 10.1007/s00345-002-0306-z. [DOI] [PubMed] [Google Scholar]
- 5.Remzi M, Klingler HC, Tinzl MV, Fong YK, Lodde M, Kiss B, et al. Morbidity of laparoscopic extraperitoneal versus transperitoneal radical prostatectomy verus open retropubic radical prostatectomy. Eur Urol. 2005;48:83–89. doi: 10.1016/j.eururo.2005.03.026. [DOI] [PubMed] [Google Scholar]
- 6.Msezane LP, Reynolds WS, Gofrit ON, Shalhav AL, Zagaja GP, Zorn KC. Bladder neck contracture after robot-assisted laparoscopic radical prostatectomy: evaluation of incidence and risk factors and impact on urinary function. J Endourol. 2008;22:97–104. [PubMed] [Google Scholar]
- 7.Breyer BN, McAninch JW. Management of recalcitrant bladder neck contracture after radical prostatectomy for prostate cancer: endoscopic and open surgery. J Urol. 2011;185:390–391. doi: 10.1016/j.juro.2010.11.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Touijer K, Eastham JA, Secin FP, Romero Otero J, Serio A, Stasi J, et al. Comprehensive prospective comparative analysis of outcomes between open and laparoscopic radical prostatectomy conducted in 2003 to 2005. J Urol. 2008;179:1811–1817. doi: 10.1016/j.juro.2008.01.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Krambeck AE, DiMarco DS, Rangel LJ, Bergstralh EJ, Myers RP, Blute ML, et al. Radical prostatectomy for prostatic adenocarcinoma: a matched comparison of open retropubic and robot-assisted techniques. BJU Int. 2009;103:448–453. doi: 10.1111/j.1464-410X.2008.08012.x. [DOI] [PubMed] [Google Scholar]
- 10.Hu JC, Nelson RA, Wilson TG, Kawachi MH, Ramin SA, Lau C, et al. Perioperative complications of laparoscopic and robotic assisted laparoscopic radical prostatectomy. J Urol. 2006;175:541–546. doi: 10.1016/S0022-5347(05)00156-4. [DOI] [PubMed] [Google Scholar]
- 11.Kumar V, Abbas AK, Fausto N, Robbins SL, Cotran RS. Tissue renewal and repair: regeneration, healing and fibrosis. In: Kumar V, Abbas AK, Fausto N, editors. Robbins and Cotran pathologic basis of disease. 7th ed. Philadelphia: Elsevier Saunders; 2005. pp. 111–115. [Google Scholar]
- 12.Surya BV, Provet J, Johanson KE, Brown J. Anastomotic strictures following radical prostatectomy: risk factors and management. J Urol. 1990;143:755–758. doi: 10.1016/s0022-5347(17)40082-6. [DOI] [PubMed] [Google Scholar]
- 13.Kostakopoulos A, Argiropoulos V, Protogerou V, Tekerlekis P, Melekos M. Vesicourethral anastomotic strictures after radical retropubic prostatectomy: the experience of a single institution. Urol Int. 2004;72:17–20. doi: 10.1159/000075267. [DOI] [PubMed] [Google Scholar]
- 14.Huang G, Lepor H. Factors predisposing to the development of anastomotic strictures in a single-surgeon series of radical retropubic prostatectomies. BJU Int. 2006;97:255–258. doi: 10.1111/j.1464-410X.2005.05908.x. [DOI] [PubMed] [Google Scholar]
- 15.Hanson GR, Odom E, Borden LS, Jr, Neil N, Corman JM. Post-operative drain output as a predictor of bladder neck contracture following radical prostatectomy. Int Urol Nephrol. 2008;40:351–354. doi: 10.1007/s11255-007-9239-1. [DOI] [PubMed] [Google Scholar]
- 16.Erickson BA, Meeks JJ, Roehl KA, Gonzalez CM, Catalona WJ. Bladder neck contracture after retropubic radical prostatectomy: incidence and risk factors from a large single-surgeon experience. BJU Int. 2009;104:1615–1619. doi: 10.1111/j.1464-410X.2009.08700.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Orvieto MA, Zorn KC, Gofrit ON, Anderson J, Zagaja GP, Brendler CB. Surgical modifications in bladder neck reconstruction and vesicourethral anastomosis during radical retropubic prostatectomy to reduce bladder neck contractures. Can J Urol. 2006;13:3353–3357. [PubMed] [Google Scholar]
- 18.Joseph JV, Vicente I, Madeb R, Erturk E, Patel HR. Robot-assisted vs pure laparoscopic radical prostatectomy: are there any differences? BJU Int. 2005;96:39–42. doi: 10.1111/j.1464-410X.2005.05563.x. [DOI] [PubMed] [Google Scholar]
- 19.Rassweiler J, Sentker L, Seemann O, Hatzinger M, Rumpelt HJ. Laparoscopic radical prostatectomy with the Heilbronn technique: an analysis of the first 180 cases. J Urol. 2001;166:2101–2108. [PubMed] [Google Scholar]
- 20.Nadu A, Salomon L, Hoznek A, Olsson LE, Saint F, de La Taille A, et al. Early removal of the catheter after laparoscopic radical prostatectomy. J Urol. 2001;166:1662–1664. [PubMed] [Google Scholar]
- 21.Sacco E, Prayer-Galetti T, Pinto F, Fracalanza S, Betto G, Pagano F, et al. Urinary incontinence after radical prostatectomy: incidence by definition, risk factors and temporal trend in a large series with a long-term follow-up. BJU Int. 2006;97:1234–1241. doi: 10.1111/j.1464-410X.2006.06185.x. [DOI] [PubMed] [Google Scholar]
- 22.Walsh PC. Anatomic radical prostatectomy: evolution of the surgical technique. J Urol. 1998;160(6 Pt 2):2418–2424. doi: 10.1097/00005392-199812020-00010. [DOI] [PubMed] [Google Scholar]