

Abstract
This study examined the effects of Korean red ginseng (KRG) on obese women and aimed to confirm that the effects of KRG on obesity differ dependently on a gene. Fifty obese women were recruited and randomized to receive KRG (n=24) or placebo (n=26) for 8 wk. Measurements of blood pressure, height, weight, waist circumference, waist-hip ratio (WHR), total fat mass, percentage of body fat, resting metabolic rate, basal body temperature, and daily food intake (FI), blood test (serum lipid, liver and renal function), Korean version of obesity-related quality of life scale (KOQOL), and a gene examination were performed. Comparisons of subjects before and after the administration of KRG revealed significant improvements of obesity in terms of weight, body mass index (BMI), WHR, FI, and KOQOL. However, in the comparison between KRG group and placebo group, only KOQOL was significantly different. KRG displayed significant efficacy on BMI and KOQOL in the CT genotype of the G protein beta 3 gene, but not in the CC genotype, on blood sugar test in the Trp64/Arg genotype of the beta 3 adrenergic receptor gene, but not in Trp64/ Trp genotype, on KOQOL in the DD genotype of the angiotensin I converting enzyme gene, but not in the ID and DD genotypes. The effects of KRG on obesity were confirmed to some extent. However, a distinct effect compared to placebo was not confirmed. KRG is more effective for improving the secondary issues of the quality of life derived from obesity rather than having direct effects on the obesity-related anthropometric assessment and blood test indices.
Keywords: Panax ginseng, Korean red ginseng, Obesity, Genetic polymorphism, Single nucleotide polymorphism
INTRODUCTION
Obesity is caused by the imbalance of energy metabolism. But it is not clear whether higher intake or lower consumption is more important. Consumed energy can be roughly divided into activity energy expenditure and resting energy expenditure (REE). Furthermore, REE can be subdivided into obligatory energy expenditure, which is absolutely necessary for life conservation, and adaptive thermogenesis, which is induced by cold exposure or food intake. In addition, REE can deviate by about 25% depending on an individual’s metabolism [1,2]. Also, since REE takes up the most part of the total energy consumption, even minor differences of REE can manifest as considerable metabolic changes in the long-term, which greatly affects weight control. Thus, reduced REE may be the greatest risk factor of obesity [3].
People with reduced REE easily become obese, even if they eat less than others do. Studies seeking to determine a genetic basis continue to be carried out. To examine the correlation between obesity and heredity, in the early stage, studies on twins, adoptees and genealogy had been carried out. The collective results to date indicate that 40% to 70% of the differences of the obesity-related phenotypes are affected by heredity [4]. Recently, with the development of molecular biological technology on genes, studies aimed at determining what genes determine energy metabolism are being actively carried out.
The occurrence of gene mutants in a single base pair with a frequency of over 1%, which is relatively common, is called gene polymorphism or single nucleotide polymorphism (SNP). Forty SNPs related to obesity have been identified in various studies [4]. Among them, beta 3 adrenergic receptor (ADRB3), G protein beta 3 (GNB3) and angiotensin I converting enzyme (ACE) are important genes that control REE.
Korean red ginseng (KRG) is steamed and dried ginseng [5]. KRG is effective for male impotence, prevention of relapse of stomach cancer, and possible treatment of human immunodeficiency virus-1 infection [6-8]. Also, KRG or ginseng has been proven to be very effective for improving obesity and abnormal metabolism in animal studies and clinical studies [9-12]. These effects of KRG and ginseng on the treatment of obesity can be thought to be greater in the obesity caused by reduced energy metabolism. However, there have been no pharmacogenomic studies using ginseng or KRG applied to obesity and no studies related to genotype.
Therefore, this study tried to examine the effects of KRG on obese women by administrating 6 g of powdered KRG three times a day for 8 weeks and to confirm that the effects of KRG on the improvement of obesity differed depending on the polymorphism of a gene(s) related to energy metabolism. It was assumed that if a mutation takes place in the energy metabolism-related ADRB3, GNB3, and ACE genes, the risk of the occurrence of obesity would increases and that the effects of KRG on the improvement of obesity that stimulates energy metabolism would increase.
MATERIALS AND METHODS
Study plan
This clinical study was a randomized, double-blind, placebo-controlled, single center clinical trial. It was carried out on 50 obese females in the Dongguk University Ilsan Oriental Hospital. Approval for the trial was granted by the Hospital’s Institutional Review Board (approval no. SR-15).
Subject recruitment
Through posters in the hospital and advertisements on local daily news, from October 2010 through February 2011, 69 volunteers were recruited and 50 persons were selected as the final subjects based on the following criteria for inclusion and exclusion (Table 1).
Table 1.
Study selection criteria
| Inclusion criteria | Exclusion criteria |
|---|---|
|
| |
| Subjects aged of 18-65 yr | Subjects with significant history or current presence of cardiovascular disease, hepatic and renal |
| BMI ≥25 kg/m2 | dysfunction, cancer |
| Weight stable individuals (≤±3 kg) in the preceding 3 mo | ALT, AST >2.5 times of normal range |
| Sedentary individuals | Creatinine >2.0 mg/dL |
| Otherwise healthy nonsmokers | Clinically significant abnormal electrocardiogram |
| Subjects signed informed consent forms | Patient on drugs that could have interfered with the conduct of the study |
| Known allergy or sensitivity to any of the medication | |
| Pregnant women | |
BMI, body mass index; ALT, aminotransferase; AST, aspartate aminotransferase.
Random assignment and double blind test
A randomization code was produced by a statistician, using the SAS system based on the block assignment method with a block size of 4. This randomization code was provided only to the persons in charge of the study in Korea Ginseng Corporation, and was blinded for the remainder of people concerned with the study until the termination of the study. In the order of the randomization code, the recruited patients were randomly assigned to the KRG group or the placebo group. KRG and placebo with randomization code on them were provided from Korea Ginseng Corporation and were distributed to the patients by the administrative pharmacist. To maintain the double blinding, the test medicine and the placebo were packed in the same shape capsule. To check the appropriateness of the blind test for the subjects, after the study, a self-questionnaire was carried out to ask whether they have taken real KRG or placebo.
Drug administration
The subjects assigned to the KRG group were required to take 12 capsules of 500 mg KRG (Jeong Gwan Jang; Korea Ginseng Corporation, Daejeon, Korea) for a total of 6 g extract, three times a day, while those assigned to the placebo group took a corn starch capsules of the same quantity and shape placebo. Drugs for 2 wk were provided at a single visit, and subjects were asked to revisit every second week for a total of 8 wk. The subjects were required to return leftover drugs in the next visit, through which their compliance to the administration was checked. Over 80% compliance was taken as the target of per protocol (PP) analysis. During the study period, the subjects were not restricted with their caloric intake and were allowed to eat meals as usual. However, an extreme diet that might affect the results such as binge eating or fasting was prohibited, and subjects were asked to maintain their normal activities, but were prohibited from beginning new exercise.
Effectiveness and safety evaluation item
Before drug administration, blood pressure (BP), height, weight, waist circumference (WC), waist-hip ratio (WHR), total fat mass (FM), percentage of body fat (BF%), resting metabolic rate (RMR), basal body temperature, daily food intake (FI), blood test (serum lipid, liver function, and renal function), and a gene examination were conducted. As well, a questionnaire concerning the oriental medical obesity pattern differentiation and the Korean-style questionnaire on the quality of life (KOQOL) were completed by each subject. Each subject was required to revisit once every second week. At each visit, their BP, weight, WC, WHR, basal body temperature, and daily food intake were checked. Additionally, at weeks 4 and 8, FM, BF%, and RMR were checked. At the end of the study at week 8, a blood test was conducted and each subject again completed the KOQOL questionnaire.
Blood pressure, heart rate
BP and pulse at the radial artery were measured after a more than 10 min rest upon every visit with a mercury sphygmomanometer while each subject was seated.
Anthropometric assessment
The height of each subject was measured once to the nearest 0.1 cm at the first visit. Weight was measured to the nearest 0.1 kg unit every second week while each subject was minimally clothed. WC was measured with each subject in an upright posture at the mid-section between the lowest costal margin and the iliac crest (3 cm up of the anterior superior iliac spine), according to World Health Organization methodology. WC measurements were made by the same skilled measurer to verify intra-examiner-variability and the mean of three consecutive measurements was determined without pressing the skin at the end of exhalation using the same tapeline. For body mass index (BMI, kg/m2), subjects were measured during each visit.
Bioelectrical impedance
Bioelectrical impedance was determined using Inbody 3.0 (Biospace, Seoul, Korea). Measurements were carried out at the first visit and at weeks 4 and 8. As the evaluation parameters, total fat and BF% were chosen.
Resting metabolic rate measurement
Using gas exchange measurement-type portable indirect calorimetry (MedGem; Healthtech, Golden, CO, USA), RMR was measured at the first visit and at weeks 4 and 8. All measurements were done after a 30 min rest.
Blood test
To exclude liver, kidney, and metabolic diseases before the start of clinical trials, alanine aminotransferase (ALT), aspartate aminotransferase (AST), blood urine nitrogen (BUN), creatinine, glucose, total cholesterol, high-density lipoprotein (HDL) cholesterol, and triglycerides were measured. ALT and AST results over 2.5 times the normal upper limit and creatinine value over 2.0 mg/dL were excluded and blood testing was carried out at week 8. Glucose and blood lipid tests were measured through an analysis of blood gathered after a 12- hour fast.
Basal body temperature
A mercury thermometer was distributed to the subjects, who were required to measure their armpit temperature for 10 min immediately after awakening. Each subject was phoned to enquire of the first measurement on the morning of their first clinic visit. Each reading was recorded by the skilled clinical research nurse. Temperature was measured again and recorded at the time of the first visit.
Daily food intake
The amount of food intake the day preceding each clinic visit was checked by a 24-hour dietary recall method using the Computer Aided Nutritional analysis program, version 3.0, developed by The Korean Nutrition Society.
Gene analysis
DNA was separated from the peripheral venous blood of each subject by a previously described method [13]. One milliliter of each blood sample was added to a 2 mL micro-tube and 25 μL of a solution of 1 mL NP-40 in TKM1 buffer was added to dissolve the blood cells. Following washing in TKM1 buffer and solution containing 160 μL TKM2 buffer and 10 μL 10% sodium dodecyl sulfate was added. Each sample was heated at 55℃ degree for 10 min and 6 M NaCl was added to precipitate protein. DNA was precipitated using 100% ethanol and washed with 70% ethanol. The extracted DNA was stored in Tris-EDTA buffer. Polymerase chain reaction (PCR) was conducted to amplify the GNB3, ADRB3, and ACE genes.
For GNB3 PCR, 30 ng of extracted DNA received SNP sense primer (5’-TGACCCACTTGCCACCCGTGC- 3’) and SNP anti-sense primer (5’-GCAGCAGCCAGGGCTGGC- 3’), DNA polymerase, and PCR reaction buffer. The DNA was denaturated at 94℃ for 10 min and PCR was carried out using the following conditions: 35 cycles at 94℃ for 60 s, 60℃ for 45 s, 72℃ for 60 s, and, finally, 72℃ for 10 min. Electrophoresis was done for 30 min using a dye crack reactor and the presence of an amplified band was ascertained. Since the T allele is 268 bp and the C allele is 152 and 116 bps, if a band appeared at 152 and 116 bps, it was classified as C/C type; if it appeared at 152, 116, and 268 bps, it was classified as the C/T type; and if it appeared at 268 bp, it was classified as the T/T type.
For ADRB3 PCR, electrophoresis was performed for 30 min mixing with sense primer (5’-CGCCCAATACCGCCAACAC- 3’) and anti-sense primer (5’-CCACCAGGAGTCCCATCACC- 3’) and DNA polymerase PCR buffer with 30 ng of the extracted DNA. Following PCR as described above, the product was digested with Mval restriction enzyme. If, upon electrophoresis, an amplified band was observed at 99 bp, it was classified as the Trp64/Trp allele, while presence of a band at 161 bp indicated an Arg64/Arg allele; if the band appeared at 99 bp, it was classifi ed into Trp64/Trp type; if it appeared at 99 and 161 bps, it was classified as Trp64/ Argg type; if it appeared at 161 bp, it was classified as Arg64/Arg type.
For ACE, using the separated DNA and ACE primer set (SNP sense primer: 5’-CTGGACACCACTCCCATCCTTTCT- 3’; antisense primer: 5’-GATGTGGCCATCACATTCGTCAGA- 3’), PCR was carried out. Following the 30 min electrophoresis, appearance of a band was ascertained. The D allele is 235 bp while for the I allele is 153 and 523 bp. Therefore, if the band appeared in 245 bp, it was classified into the D/D type; if it appeared at 235, 153, and 523 bp, it was classified as the D/I type; and if it appeared at 153 and 523 bp, it was classified as the I/I type.
Korean-style questionnaire on the quality of life evaluation
Subjects completed the KOQOL questionnaire developed in 2003 at baseline and the end of the study [14]. The KOQOL evaluation questionnaire consists of 15 questions in six areas (mental and social health, physical health, job and domestic duty, daily life, sexual relations, and food), which are known to be relatively simple but highly reliable and accurate.
Statistical analyses
All statistical analyses were carried out using SAS ver. 9.1 (SAS Inc., Cary, NC, USA). Data represent mean±standard deviation. Statistical analysis was made by PP analysis. Student’s t-test was carried out for the comparison of KRG and placebo group. A paired t-test was carried out for the comparison of values before and after the study. A p-value of less than 0.05 was considered statistically significant.
RESULTS
Research process
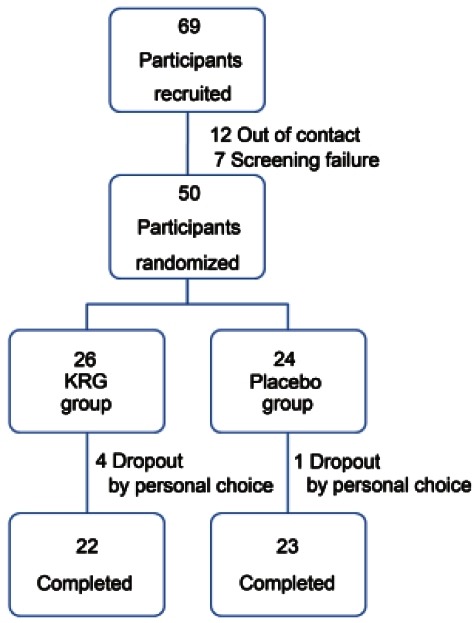
Sixty nine volunteers were recruited. Of these, 12 could not be contacted and seven were excluded upon screening. The remaining 50 subjects were randomly processed, and 26 subjects were assigned to the KRG group and 24 subjects to the placebo group. During the 8-week trial, 4 subjects were dropped out from KRG group and one was dropped out from the placebo group. Twenty two subjects in the KRG group and 23 in the placebo group completed the study (Fig. 1). Compliance with the study regimen by the subjects was 80%, so 45 subjects were selected for PP analysis.
Fig. 1. Flow chart of participants disposition. KRG, Korean red ginseng.
Comparison of characteristics of both groups before administration
Waist-hip circumference ratio of the placebo group was significantly greater than that of the KRG group (p=0.0222), while ALT of the placebo group was significantly greater than that of KRG group (p=0.0154). No other significant differences were evident between KRG and placebo groups (Table 2).
Table 2.
Demographics of participants
| Variables | No. | Red ginseng | No. | Placebo | p-value1) |
|---|---|---|---|---|---|
|
| |||||
| Age | 22 | 40.91±9.65 | 23 | 46.48±9.79 | 0.0613 |
| Height | 22 | 160.66±6.42 | 23 | 158.13±5.04 | 0.1467 |
| BW | 22 | 73.85±8.64 | 23 | 72.7±10.65 | 0.6957 |
| BMI | 22 | 28.62±2.68 | 23 | 28.99±3.25 | 0.6808 |
| RMR | 22 | 1,624.09±217.2 | 23 | 1,628.7±390.77 | 0.9611 |
| WC | 22 | 95.32±7.2 | 23 | 96.31±8.03 | 0.6659 |
| WHR | 22 | 0.92±0.04 | 23 | 0.95±0.05 | 0.0222* |
| BF% | 22 | 39.4±4.65 | 23 | 40.31±4.33 | 0.5030 |
| BFM | 22 | 29.27±6.06 | 23 | 29.51±6.79 | 0.9011 |
| FI | 22 | 1,836.77±603.67 | 23 | 1,939.48±397.08 | 0.5019 |
| BBT | 22 | 36.59±0.38 | 23 | 36.5±0.26 | 0.3750 |
| KOQOL | 22 | 38.82±5.72 | 23 | 35.04±8.36 | 0.0857 |
| BST | 22 | 105.91±11.48 | 23 | 108.7±15.24 | 0.4936 |
| TG | 22 | 119.95±55.18 | 22 | 136.59±98.33 | 0.4938 |
| HDL | 22 | 53.27±10.39 | 22 | 51.32±11.32 | 0.5539 |
| T-Chol | 22 | 190.09±35.38 | 23 | 195.04±34.02 | 0.6346 |
| BUN | 22 | 12.65±3.2 | 23 | 12.07±2.96 | 0.5273 |
| Cr | 22 | 0.66±0.1 | 23 | 0.66±0.09 | 0.9218 |
| AST | 22 | 20.05±5.58 | 23 | 25.65±12.07 | 0.0526 |
| ALT | 22 | 19.14±11.37 | 23 | 29.7±16.17 | 0.0154* |
| SBP | 22 | 122.18±9.46 | 23 | 123.61±9.91 | 0.6241 |
| DBP | 22 | 77.23±7.32 | 23 | 77.61±7.4 | 0.8629 |
| PR | 22 | 78.27±11.55 | 23 | 74.43±6.69 | 0.1841 |
| RR | 20 | 1.19±0.19 | 22 | 1.11±0.22 | 0.2620 |
Values are presented as mean±SD.
BW, body weight; BMI, body mass index; RMR, resting metabolic rate; WC, waist circumference; WHR, waist hip ratio; BF%, percentage of body fat; BFM, body fat mass; FI, food intake; BBT, basal body temperature; KOQOL, Korean obesity quality of life; BST, blood sugar test; TG, triglyceride; HDL, high density lipoprotein; T-Chol, total cholesterol; BUN, blood urine nitrogen; Cr, creatinine; AST, aspartate aminotransferase; ALT, aminotransferase; SBP, systolic blood pressure; DBP, diastolic blood pressure; PR, pulse rate; RR, RR interval.
1) p-value derived from Student’s t-test.
* p<0.05
Effects of Korean red ginseng on the improvement of obesity
After the trial, the weights of two subjects (9.09%) of the 22 in the KRG group were reduced over 5%, while none of the 23 placebo subjects displayed weight losses over 5%. The findings were not statistically significant (p=0.2333).
Notably, in the comparison between before and after the administration of KRG group, there were significant improvements of obesity in the items of body weight (p=0.0045), BMI (p=0.0352), WHR (p=0.0312), daily FI (p=0.0100), and KOQOL (p=0.004). However, in the comparison between KRG Group and placebo group only KOQOL was significantly different (Table 3).
Table 3.
Changes of parameters after intervention
| Variables | Red ginseng | Placebo | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| No. | Mean±SD | p-value1) | No. | Mean±SD | p-value2) | |
|
| ||||||
| ΔBW | 22 | -0.75±1.66 | 0.0445* | 23 | -0.73±1.58 | 0.9603 |
| ΔBMI | 22 | -0.3±0.63 | 0.0352* | 23 | -0.33±0.64 | 0.8745 |
| ΔRMR | 22 | 55.45±253.22 | 0.3160 | 23 | -4.35±231.77 | 0.4128 |
| ΔWC | 22 | -1±2.94 | 0.1239 | 23 | -4.19±13.09 | 0.2661 |
| ΔWHR | 22 | 0±0.01 | 0.0312* | 23 | 0±0.01 | 0.2217 |
| ΔBF% | 22 | -0.06±1.59 | 0.8527 | 23 | -0.6±0.9 | 0.1684 |
| ΔBFM | 22 | -0.41±1.45 | 0.1946 | 23 | -0.69±1.03 | 0.4678 |
| ΔFI | 22 | -386.73±640.88 | 0.0100* | 23 | -288.04±400.86 | 0.5418 |
| ΔBBT | 22 | -0.13±0.46 | 0.2114 | 22 | -0.15±0.44 | 0.8676 |
| ΔKOQOL | 22 | -5.18±5.79 | 0.0004* | 23 | -0.91±5.91 | 0.0186* |
| ΔBST | 22 | -7.27±17.16 | 0.0600 | 23 | -4.7±13.14 | 0.5735 |
| ΔTG | 22 | -10.45±76.11 | 0.5264 | 22 | -25.18±75.62 | 0.5232 |
| ΔHDL | 22 | 1.18±7.21 | 0.4505 | 22 | 2.14±9.67 | 0.7123 |
| ΔT-Chol | 22 | 4.91±33.43 | 0.4986 | 23 | -1.7±19.72 | 0.4278 |
| ΔSBP | 22 | -2.86±13.09 | 0.3164 | 23 | -1.43±10.57 | 0.6883 |
| ΔDBP | 22 | -3.86±10.75 | 0.1068 | 23 | -1.13±6.92 | 0.3142 |
| ΔPR | 22 | -1.05±12.2 | 0.6919 | 23 | -2.13±9.36 | 0.7388 |
| ΔRR | 19 | -0.01±0.2 | 0.8824 | 22 | 0.05±0.23 | 0.4472 |
BW, body weight; BMI, body mass index; RMR, resting metabolic rate; WC, waist circumference; WHR, waist hip ratio; BF%, percentage of body fat; BFM, body fat mass; FI, food intake; BBT, basal body temperature; KOQOL, Korean obesity quality of life; BST, blood sugar test; TG, triglyceride; HDL, high density lipoprotein; T-Chol, total cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; PR, pulse rate; RR, RR interval.
1) p-value derived from paired t-test between pre and post.
2) p-value derived from Student’s t-test between red ginseng group and placebo group.
*p<0.05.
Comparison of obesity indices by gene polymorphism type
For 48 persons on whom gene analysis had been made among the total of 50 persons, to see if obesity indices before drug administration differs depending on gene polymorphism, they were divided into one with and without gene mutation and compared and analyzed.
G protein beta 3
Six subjects were indicated to lack gene mutation (i.e., CC type), while 42 displayed a single mutation (39 CT type and three TT type). In the comparison between the two groups, subjects with gene mutation (CT+TT) displayed significantly higher BMI (p=0.027), BF% (p=0.001) and systolic BP (p=0.034) than subjects with no gene mutation (CC) (Table 4).
Table 4.
Comparison of baseline characteristics by GNB3 polymorphism
| CC | CT + TT | p-value1) | |||
|---|---|---|---|---|---|
|
|
|
||||
| No. | Mean±SD | No. | Mean±SD | ||
|
| |||||
| BW | 6 | 67.683±7.44 | 42 | 73.917±9.90 | 0.146 |
| BMI | 6 | 26.383±1.89 | 42 | 29.217±2.94 | 0.027* |
| RMR | 6 | 1,651.67±239.95 | 42 | 1,625.00±315.67 | 0.844 |
| WC | 6 | 91.13±5.96 | 42 | 96.61±7.89 | 0.110 |
| WHR | 6 | 0.9083±0.03 | 42 | 0.9424±0.05 | 0.122 |
| BF% | 6 | 37.217±1.38 | 42 | 40.557±4.55 | 0.001* |
| BFM | 6 | 25.167±2.49 | 42 | 30.176±6.55 | 0.072 |
| FI | 6 | 1,942.67±679.08 | 42 | 1,856.55±484.16 | 0.700 |
| BBT | 6 | 36.483±0.51 | 42 | 36.550±0.29 | 0.766 |
| KOQOL | 6 | 37.83±10.61 | 42 | 36.74±6.67 | 0.729 |
| BST | 6 | 100.50±5.32 | 42 | 108.43±13.73 | 0.171 |
| TG | 6 | 81.80±32.62 | 42 | 130.36±77.31 | 0.175 |
| HDL | 5 | 53.60±9.99 | 42 | 52.12±10.77 | 0.771 |
| T-Chol | 5 | 176.83±26.98 | 42 | 195.81±34.73 | 0.207 |
| SBP | 6 | 118.17±3.87 | 42 | 123.33±10.39 | 0.034* |
| DBP | 6 | 78.00±3.41 | 42 | 77.24±7.86 | 0.686 |
GNB3, G protein beta 3; BW, body weight; BMI, body mass index; RMR, resting metabolic rate; WC, waist circumference; WHR, waist hip ratio; BF%, percentage of body fat; BFM, body fat mass; FI, food intake; BBT, basal body temperature; KOQOL, Korean obesity quality of life; BST, blood sugar test; TG, triglyceride; HDL, high density lipoprotein; T-Chol, total cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure.
1) p-value derived from Student’s t-test between CC group and CT+TT group.
* p<0.05.
Beta 3 adrenergic receptor
Thirty three subjects were classified as lacking ADRBr gene mutation (Trp64/Trp) while 15 subjects harbored a mutation (10 in Trp64/Arg and five in Arg64/Arg). In the comparison between the two groups, subjects with gene mutation displayed significantly lower HDL than subjects lacking gene mutation (p=0.012) (Table 5).
Table 5.
Comparison of baseline characteristics by ADRB3 polymorphism
| Trp64/Trp | Trp64/Arg+Arg64/Arg | p-value1) | |||
|---|---|---|---|---|---|
|
|
|
||||
| No. | Mean±SD | No. | Mean±SD | ||
|
| |||||
| BW | 33 | 72.352±9.34 | 15 | 74.867±10.83 | 0.415 |
| BMI | 33 | 28.570±2.70 | 15 | 29.507±2.70 | 0.316 |
| RMR | 33 | 1,654.55±317.04 | 15 | 1,570.67±3.50 | 0.383 |
| WC | 33 | 94.93±6.76 | 15 | 98.12±317.04 | 0.263 |
| WHR | 33 | 0.9370±0.05 | 15 | 0.9407±278.81 | 0.816 |
| BF% | 33 | 39.691±4.15 | 15 | 41.127±6.76 | 0.301 |
| BFM | 33 | 28.870±6.00 | 15 | 31.047±9.72 | 0.279 |
| FI | 33 | 1,810.79±541.01 | 15 | 1,991.67±0.05 | 0.254 |
| BBT | 33 | 36.530±0.31 | 15 | 36.567±0.05 | 0.718 |
| KOQOL | 33 | 36.24±7.75 | 15 | 38.27±4.15 | 0.368 |
| BST | 33 | 107.61±14.02 | 15 | 107.07±4.96 | 0.897 |
| TG | 33 | 116.66±47.47 | 15 | 143.40±6.00 | 0.260 |
| HDL | 33 | 54.88±9.40 | 15 | 46.73±7.16 | 0.012* |
| T-Chol | 33 | 191.94±35.62 | 15 | 196.73±541.01 | 0.658 |
| SBP | 33 | 121.58±10.27 | 15 | 125.13±401.07 | 0.255 |
| DBP | 33 | 77.21±7.43 | 15 | 77.60±0.31 | 0.869 |
ADRB3, beta 3 adrenergic receptor; BW, body weight; BMI, body mass index; RMR, resting metabolic rate; WC, waist circumference; WHR, waist hip ratio; BF%, percentage of body fat; BFM, body fat mass; FI, food intake; BBT, basal body temperature; KOQOL, Korean obesity quality of life; BST, blood sugar test; TG, triglyceride; HDL, high density lipoprotein; T-Chol, total cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure.
1)p-value derived from Student’s t-test between Trp64/Trp group and Trp64/Arg + Arg64/Arg group.
*p<0.05.
Angiotensin I converting enzyme
Sixteen subjects lacked gene mutation (II), while 32 subjects did (22 in ID and 10 in DD). There was no significant difference in the comparison between the two groups (Table 6).
Table 6.
Comparison of baseline characteristics by ACE polymorphism
| II | ID+DD | p-value1) | |||
|---|---|---|---|---|---|
|
|
|
||||
| No. | Mean±SD | No. | Mean±SD | ||
|
| |||||
| BW | 16 | 72.050±9.81 | 32 | 75.313±9.65 | 0.281 |
| BMI | 16 | 28.541±2.81 | 32 | 29.506±3.25 | 0.293 |
| RMR | 16 | 1,610.31±308.47 | 32 | 1,664.38±305.11 | 0.568 |
| WC | 16 | 94.98±7.88 | 32 | 97.81±7.65 | 0.243 |
| WHR | 16 | 0.9344±0.05 | 32 | 0.9456±0.05 | 0.471 |
| BF% | 16 | 40.131±4.59 | 32 | 40.156±4.18 | 0.985 |
| BFM | 16 | 29.128±6.69 | 32 | 30.394±5.87 | 0.524 |
| FI | 16 | 1,817.53±525.77 | 32 | 1,966.88±458.11 | 0.339 |
| BBT | 16 | 36.506±0.30 | 32 | 36.613±0.36 | 0.281 |
| KOQOL | 16 | 36.88±7.17 | 32 | 36.88±7.29 | 1.000 |
| BST | 16 | 106.34±12.02 | 32 | 109.63±15.50 | 0.423 |
| TG | 16 | 121.48±86.50 | 32 | 132.38±47.71 | 0.643 |
| HDL | 16 | 52.65±11.01 | 32 | 51.56±10.05 | 0.744 |
| T-Chol | 16 | 190.59±35.64 | 32 | 199.13±31.45 | 0.421 |
| SBP | 16 | 121.88±11.34 | 32 | 124.31±6.30 | 0.344 |
| DBP | 16 | 77.41±7.03 | 32 | 77.19±8.42 | 0.925 |
ACE, angiotensin I converting enzyme; BW, body weight; BMI, body mass index; RMR, resting metabolic rate; WC, waist circumference; WHR, waist hip ratio; BF%, percentage of body fat; BFM, body fat mass; FI, food intake; BBT, basal body temperature; KOQOL, Korean obesity quality of life; BST, blood sugar test; TG, triglyceride; HDL, high density lipoprotein; T-Chol, total cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure.
1) p-value derived from Student’s t-test between II group and II + DD group.
Effects of Korean red ginseng on the improvement of obesity by gene polymorphism type
The gene sample of one subject of the 22 in the KRG group who completed the clinical study was lost. So, the differences of obesity indices between before and after were analyzed for 21 subjects.
G protein beta 3
Of the 21 subjects, three were CC type without mutation, 17 were CT type with homogenous mutation, and one was TT type with heterogenic mutation. As a result of analysis of obesity indices before and after the ad-ministration of KRG according to gene polymorphism type, BMI (p=0.0387) and KOQOL (p=0.0002) were associated with significant effects on the improvement of obesity in the CT type, while there was no significant effects in the CC type. Food intake was significantly reduced in the CC type (p=0.0100), and displayed a decreasing, but statistically insignificant, tendency in the CT type. Systolic BP was significantly increased in the CC type (p=0.0377), while it tended to be reduced in the CT type. WHR was significantly increased in the CT type (p=0.0144) (Table 7).
Table 7.
Changes of parameters after intervention by GNB3 genotype in Korean red ginseng group
| Genotype | Pre | Post | p-value1) | |
|---|---|---|---|---|
|
| ||||
| BW | CC (N=3) | 72.57±7.99 | 71.97±7.71 | 0.3479 |
| CT (N=17) | 74.94±8.91 | 74.1±8.32 | 0.0630 | |
| TT (N=1) | 62.3±. | 64±. | - | |
| BMI | CC (N=3) | 27.2±2.61 | 26.97±2.31 | 0.3688 |
| CT (N=17) | 29.16±2.66 | 28.81±2.72 | 0.0387* | |
| TT (N=1) | 26.1±. | 26.9±. | - | |
| RMR | CC (N=3) | 1,843.33±171.56 | 1,836.67±263.5 | 0.9340 |
| CT (N=17) | 1,615.88±199.66 | 1,671.18±236.85 | 0.4332 | |
| TT (N=1) | 1280± | 1430±. | - | |
| WC | CC (N=3) | 93.83±0.76 | 94.4±1.13 | 0.5803 |
| CT (N=17) | 96.31±7.86 | 95.08±6.75 | 0.1221 | |
| TT (N=1) | 89±. | 90.2± | - | |
| WHR | CC (N=3) | 0.9±0.03 | 0.9±0.04 | 0.4226 |
| CT (N=17) | 0.92±0.05 | 0.93±0.05 | 0.0144* | |
| TT (N=1) | 0.94±. | 0.94±. | - | |
| BF% | CC (N=3) | 36.33±1.45 | 36.33±2.78 | 1 |
| CT (N=17) | 40.16±4.82 | 40.09±4.73 | 0.8618 | |
| TT (N=1) | 41.6±. | 40.6±. | - | |
| BFM | CC (N=3) | 26.4±3.29 | 26.3±4.59 | 0.9067 |
| CT (N=17) | 30.31±6.45 | 29.8±5.96 | 0.2051 | |
| TT (N=1) | 25.9±. | 26±. | - | |
| FI | CC (N=3) | 2,431.33±389.71 | 1,545.33±544.58 | 0.0100* |
| CT (N=17) | 1,782.41±587.51 | 1,475±344.17 | 0.0781 | |
| TT (N=1) | 991±. | 1157±. | - | |
| BBT | CC (N=3) | 36.77±0.59 | 36.67±0.15 | 0.7418 |
| CT (N=17) | 36.61±0.33 | 36.41±0.29 | 0.0549 | |
| TT (N=1) | 36±. | 37±. | - | |
| KOQOL | CC (N=3) | 45.33±4.51 | 42.67±9.07 | 0.6813 |
| CT (N=17) | 37.71±5.35 | 31.59±6.99 | 0.0002* | |
| TT (N=1) | 43±. | 42±. | - | |
| BST | CC (N=3) | 100±6.56 | 91±13.53 | 0.5187 |
| CT (N=17) | 105.82±10.54 | 101.06±12.05 | 0.2309 | |
| TT (N=1) | 133±. | 90±. | - | |
| TG | CC (N=3) | 77±37.64 | 66.67±14.98 | 0.6221 |
| CT (N=17) | 116.88±45.62 | 105.35±73.97 | 0.5295 | |
| TT (N=1) | 157±. | 282±. | - | |
| HDL | CC (N=3) | 55.33±11.15 | 56.33±8.62 | 0.8600 |
| CT (N=17) | 53.47±11.05 | 54.88±12.43 | 0.4362 | |
| TT (N=1) | 50±. | 43±. | - | |
| T-Chol | CC (N=3) | 191.33±25.93 | 181±17.69 | 0.3191 |
| CT (N=17) | 184.29±33.55 | 190.59±54.58 | 0.4866 | |
| TT (N=1) | 268±. | 263±. | - | |
| BUN | CC (N=3) | 14.13±0.51 | 15.5±3.47 | 0.5120 |
| CT (N=17) | 12.46±3.47 | 12.15±3.02 | 0.6652 | |
| TT (N=1) | 9.5±. | 13.2±. | - | |
| Cr | CC (N=3) | 0.61±0.01 | 0.61±0.05 | 1 |
| CT (N=17) | 0.67±0.11 | 0.67±0.07 | 0.9330 | |
| TT (N=1) | 0.68±. | 0.75±. | - | |
| AST | CC (N=3) | 20±6.24 | 18.33±3.51 | 0.4226 |
| CT (N=17) | 20.41±5.79 | 17.65±4.68 | 0.0151* | |
| TT (N=1) | 14±. | 11±. | - | |
| ALT | CC (N=3) | 17±7 | 15±3.61 | 0.4380 |
| CT (N=17) | 20.29±12.46 | 16.18±6.85 | 0.0645 | |
| TT (N=1) | 11±. | 18±. | - | |
| SBP | CC (N=3) | 120±3.61 | 126.67±5.86 | 0.0377* |
| CT (N=17) | 122.47±9.68 | 117±10.6 | 0.1222 | |
| TT (N=1) | 110±. | 118±. | - | |
| DBP | CC (N=3) | 76.33±4.04 | 76.67±9.24 | 0.9678 |
| CT (N=17) | 77.29±8.18 | 72.94±10.18 | 0.1301 | |
| TT (N=1) | 75±. | 72±. | - | |
| PR | CC (N=3) | 84.67±11.93 | 86.33±10.21 | 0.6035 |
| CT (N=17) | 77.47±12.1 | 76.24±9.32 | 0.7158 | |
| TT (N=1) | 79±. | 72±. | - | |
| RR | CC (N=3) | 1.11±0.02 | 1.14±0.04 | 0.2222 |
| CT (N=17) | 1.2±0.22 | 1.18±0.06 | 0.7960 | |
| TT (N=1) | 1.26±. | 1.26±. | - | |
GNB3, G protein beta 3; BW, body weight; BMI, body mass index; RMR, resting metabolic rate; WC, waist circumference; WHR, waist hip ratio; BF%, percentage of body fat; BFM, body fat mass; FI, food intake; BBT, basal body temperature; KOQOL, Korean obesity quality of life; BST, blood sugar test; TG, triglyceride; HDL, high density lipoprotein; T-Chol, total cholesterol; BUN, blood urine nitrogen; Cr, creatinine; AST, aspartate aminotransferase; ALT, aminotransferase; SBP, systolic blood pressure; DBP, diastolic blood pressure; PR, pulse rate; RR, RR interval.
1) p-value derived from paired t-test between pre and post.
*p<0.05.
Beta 3 adrenergic receptor
Of the 21 subjects, 15 were Trp64/Trp type without mutation, five were Trp64/Arg type with heterogenic mutation, and one was Arg64/Arg type with homogenous mutation. KOQOL was associated with significant improvement of obesity in both Trp64/Arg and Trp64/Trp types (p=0.0090 and p=0.0096, respectively), while blood sugar test (BST) was significantly reduced (p=0.0375) in the Trp64/Arg type. However, there was no significant difference in the Trp64/Trp type. AST was significantly reduced (p=0.0280) in the Trp64/Trp type, while there was no significant change in the Trp64/Arg type (Table 8).
Table 8.
Changes of parameters after intervention by ADRB3 genotype in Korean red ginseng group
| Genotype | Pre | Post | p-value1) | |
|---|---|---|---|---|
|
| ||||
| BW | Arg64/Arg (N=1) | 85.9±. | 81.2±. | - |
| Trp64/Arg (N=5) | 73.54±12.46 | 72.94±11.42 | 0.3062 | |
| Trp64/Trp (N=15) | 73.35±7.5 | 72.91±7.28 | 0.2843 | |
| BMI | Arg64/Arg (N=1) | 27.1±. | 25.6±. | - |
| Trp64/Arg (N=5) | 29.54±4 | 29.32±3.73 | 0.3188 | |
| Trp64/Trp (N=15) | 28.58±2.3 | 28.36±2.28 | 0.2099 | |
| RMR | Arg64/Arg (N=1) | 1830±. | 2130±. | - |
| Trp64/Arg (N=5) | 1,578±253.81 | 1,696±206.95 | 0.2009 | |
| Trp64/Trp (N=15) | 1,637.33±214.99 | 1,649.33±236.75 | 0.8713 | |
| WC | Arg64/Arg (N=1) | 101±. | 96.5±. | - |
| Trp64/Arg (N=5) | 94.96±9.94 | 95.54±9.41 | 0.2871 | |
| Trp64/Trp (N=15) | 95.47±6.68 | 94.37±5.29 | 0.2058 | |
| WHR | Arg64/Arg (N=1) | 0.81±. | 0.81±. | - |
| Trp64/Arg (N=5) | 0.94±0.03 | 0.94±0.03 | 0.0705 | |
| Trp64/Trp (N=15) | 0.92±0.04 | 0.93±0.04 | 0.0552 | |
| BF% | Arg64/Arg (N=1) | 42.1±. | 40.3±. | - |
| Trp64/Arg (N=5) | 39.14±5.05 | 39.44±5.96 | 0.7095 | |
| Trp64/Trp (N=15) | 39.71±4.69 | 39.58±4.37 | 0.768 | |
| BFM | Arg64/Arg (N=1) | 36.1±. | 32.7±. | - |
| Trp64/Arg (N=5) | 29±7.57 | 28.96±7.48 | 0.9498 | |
| Trp64/Trp (N=15) | 29.28±5.76 | 28.93±5.44 | 0.3517 | |
| FI | Arg64/Arg (N=1) | 2077±. | 1013±. | - |
| Trp64/Arg (N=5) | 1,948.4±590.68 | 1,578.8±307.86 | 0.1831 | |
| Trp64/Trp (N=15) | 1,784.47±659.87 | 1,464.07±373.8 | 0.0985 | |
| BBT | Arg64/Arg (N=1) | 36.6±. | 36±. | - |
| Trp64/Arg (N=5) | 36.66±0.56 | 36.56±0.35 | 0.7654 | |
| Trp64/Trp (N=15) | 36.59±0.34 | 36.47±0.28 | 0.2969 | |
| KOQOL | Arg64/Arg (N=1) | 34±. | 30±. | - |
| Trp64/Arg (N=5) | 40.2±5.63 | 34.2±2.86 | 0.009* | |
| Trp64/Trp (N=15) | 39±6 | 33.73±9.58 | 0.0096* | |
| BST | Arg64/Arg (N=1) | 117±. | 91±. | - |
| Trp64/Arg (N=5) | 112.4±10.64 | 100.2±7.46 | 0.0375* | |
| Trp64/Trp (N=15) | 103.53±11.44 | 99.27±13.99 | 0.4081 | |
| TG | Arg64/Arg (N=1) | 99±. | 65±. | - |
| Trp64/Arg (N=5) | 131.2±26.26 | 150±116.57 | 0.7338 | |
| Trp64/Trp (N=15) | 108±51.56 | 97.2±63.66 | 0.4948 | |
| HDL | Arg64/Arg (N=1) | 53±. | 50±. | - |
| Trp64/Arg (N=5) | 45±6.48 | 44.4±9.15 | 0.7664 | |
| Trp64/Trp (N=15) | 56.47±10.57 | 58.2±11 | 0.4309 | |
| T-Chol | Arg64/Arg (N=1) | 179±. | 156±. | - |
| Trp64/Arg (N=5) | 208±36.41 | 197.8±35.54 | 0.2369 | |
| Trp64/Trp (N=15) | 183.73±36.22 | 193.4±58.06 | 0.3281 | |
| BUN | Arg64/Arg (N=1) | 10.5±. | 7.7±. | - |
| Trp64/Arg (N=5) | 13.12±2.47 | 13.64±3.79 | 0.6922 | |
| Trp64/Trp (N=15) | 12.51±3.59 | 12.69±2.83 | 0.8353 | |
| Cr | Arg64/Arg (N=1) | 0.56±. | 0.55±. | - |
| Trp64/Arg (N=5) | 0.67±0.08 | 0.68±0.06 | 0.7449 | |
| Trp64/Trp (N=15) | 0.66±0.11 | 0.67±0.07 | 0.7736 | |
| AST | Arg64/Arg (N=1) | 15±. | 17±. | - |
| Trp64/Arg (N=5) | 25.4±5.86 | 19.6±1.95 | 0.0594 | |
| Trp64/Trp (N=15) | 18.6±4.75 | 16.73±5.16 | 0.028* | |
| ALT | Arg64/Arg (N=1) | 17±. | 21±. | - |
| Trp64/Arg (N=5) | 28.4±13.15 | 20.8±3.27 | 0.1809 | |
| Trp64/Trp (N=15) | 16.53±10.21 | 14.2±6.28 | 0.2274 | |
| SBP | Arg64/Arg (N=1) | 124±. | 112±. | - |
| Trp64/Arg (N=5) | 121±8.31 | 120.2±11.84 | 0.9084 | |
| Trp64/Trp (N=15) | 121.53±9.98 | 118.27±10.31 | 0.3701 | |
| DBP | Arg64/Arg (N=1) | 76±. | 57±. | - |
| Trp64/Arg (N=5) | 75.6±7.64 | 69.2±6.72 | 0.3228 | |
| Trp64/Trp (N=15) | 77.6±7.84 | 75.93±9.38 | 0.5324 | |
| PR | Arg64/Arg (N=1) | 72±. | 92±. | - |
| Trp64/Arg (N=5) | 82.2±16.57 | 73.2±6.53 | 0.3268 | |
| Trp64/Trp (N=15) | 77.8±10.5 | 77.93±10.05 | 0.9532 | |
| RR | Arg64/Arg (N=1) | 1.07±. | 1.13±. | - |
| Trp64/Arg (N=5) | 1.11±0.04 | 1.17±0.07 | 0.2235 | |
| Trp64/Trp (N=15) | 1.23±0.23 | 1.18±0.06 | 0.5531 | |
ADRB3, beta 3 adrenergic receptor; BW, body weight; BMI, body mass index; RMR, resting metabolic rate; WC, waist circumference; WHR, waist hip ratio; BF%, percentage of body fat; BFM, body fat mass; FI, food intake; BBT, basal body temperature; KOQOL, Korean obesity quality of life; BST, blood sugar test; TG, triglyceride; HDL, high density lipoprotein; T-Chol, total cholesterol; BUN, blood urine nitrogen; Cr, creatinine; AST, aspartate aminotransferase; ALT, aminotransferase; SBP, systolic blood pressure; DBP, diastolic blood pressure; PR, pulse rate; RR, RR interval.
1) p-value derived from paired t-test between pre and post.
* p<0.05.
Angiotensin I converting enzyme
Seven subjects were II type without mutation of the 21 subjects, nine were ID type with heterogenic mutation and five were DD type with homogenous mutation. KOQOL for the DD type showed statistically significant effects on obesity improvement (p=0.0030), while in the II and ID types, only a decreasing tendency was detected. BST and AST were significantly reduced in II type (p=0.0227 and p=0.0218, respectively), while in the ID and DD types, only a decreasing tendency was detected (Table 9).
Table 9.
Changes of parameters after intervention by ACE genotype in Korean red ginseng group
| Genotype | Pre | Post | p-value1) | |
|---|---|---|---|---|
|
| ||||
| BW | DD (N=5) | 71.46±10.75 | 70.46±9.02 | 0.3518 |
| ID (N=9) | 74.78±7.11 | 74.12±7.18 | 0.3196 | |
| II (N=7) | 74.8±10.39 | 74.31±9.47 | 0.3292 | |
| BMI | DD (N=5) | 28.36±2.07 | 28.06±2.33 | 0.3965 |
| ID (N=9) | 29.23±2.17 | 29±2.33 | 0.3676 | |
| II (N=7) | 28.37±3.78 | 28.04±3.43 | 0.1689 | |
| RMR | DD (N=5) | 1,518±272.34 | 1,646±306.48 | 0.2096 |
| ID (N=9) | 1,611.11±231.32 | 1,683.33±221.47 | 0.4083 | |
| II (N=7) | 1,741.43±116.54 | 1,710±256.12 | 0.8039 | |
| WC | DD (N=5) | 91.7±6.08 | 91.46±4.35 | 0.8334 |
| ID (N=9) | 96.61±7.29 | 95.16±6.55 | 0.2101 | |
| II (N=7) | 97.11±7.92 | 96.59±6.53 | 0.6753 | |
| WHR | DD (N=5) | 0.91±0.06 | 0.92±0.06 | 0.0705 |
| ID (N=9) | 0.93±0.04 | 0.93±0.05 | 0.1950 | |
| II (N=7) | 0.91±0.04 | 0.92±0.0 | 0.1723 | |
| BF% | DD (N=5) | 39.5±3.57 | 39.32±4.57 | 0.8135 |
| ID (N=9) | 40.37±5.5 | 40.34±5.13 | 0.9733 | |
| II (N=7) | 38.94±4.41 | 38.79±4.22 | 0.7797 | |
| BFM | DD (N=5) | 28.28±5.3 | 27.64±4.41 | 0.4909 |
| ID (N=9) | 30.33±6.3 | 30.07±6.09 | 0.6142 | |
| II (N=7) | 29.41±7.02 | 28.96±6.56 | 0.3991 | |
| FI | DD (N=5) | 1,699.6±433.39 | 1,334.2±441.3 | 0.2112 |
| ID (N=9) | 1,838.44±715.71 | 1,400.33±387.43 | 0.1333 | |
| II (N=7) | 1,934.57±663.61 | 1,656.29±202.16 | 0.2695 | |
| BBT | DD (N=5) | 36.56±0.32 | 36.46±0.43 | 0.7594 |
| ID (N=9) | 36.57±0.33 | 36.47±0.3 | 0.5403 | |
| II (N=7) | 36.69±0.5 | 36.49±0.26 | 0.2023 | |
| KOQOL | DD (N=5) | 36±2.83 | 30.4±4.1 | 0.0030* |
| ID (N=9) | 39±6.69 | 34.44±9.25 | 0.0674 | |
| II (N=7) | 41.29±5.65 | 35±9.22 | 0.0641 | |
| BST | DD (N=5) | 107.4±10.01 | 102.4±9.86 | 0.5851 |
| ID (N=9) | 106.11±13.06 | 101.56±11.9 | 0.5496 | |
| II (N=7) | 105.71±12.42 | 93.57±14.08 | 0.0227* | |
| TG | DD (N=5) | 111.2±41.34 | 142.2±120.91 | 0.5608 |
| ID (N=9) | 108±45.84 | 93.89±77.14 | 0.5404 | |
| II (N=7) | 121±54.58 | 102.43±39.92 | 0.3742 | |
| HDL | DD (N=5) | 53±11.66 | 50.8±10.85 | 0.3694 |
| ID (N=9) | 55.22±9.68 | 58.78±13.62 | 0.2638 | |
| II (N=7) | 51.86±12.14 | 51.71±9.34 | 0.9526 | |
| T-Chol | DD (N=5) | 191.4±32.24 | 182±38.23 | 0.2555 |
| ID (N=9) | 188.44±41.36 | 207.44±71.16 | 0.2441 | |
| II (N=7) | 188.86±36.77 | 181.29±25.59 | 0.1898 | |
| BUN | DD (N=5) | 10.98±2.96 | 10.36±1.78 | 0.5931 |
| ID (N=9) | 11.58±1.95 | 11.94±2.18 | 0.7454 | |
| II (N=7) | 14.96±3.74 | 15.27±3.4 | 0.8129 | |
| Cr | DD (N=5) | 0.67±0.09 | 0.67±0.09 | 1.0000 |
| ID (N=9) | 0.62±0.08 | 0.64±0.06 | 0.2148 | |
| II (N=7) | 0.71±0.11 | 0.69±0.07 | 0.5296 | |
| AST | DD (N=5) | 23.8±6.53 | 17.6±3.97 | 0.0666 |
| ID (N=9) | 17.44±3.47 | 17.11±4.88 | 0.5943 | |
| II (N=7) | 20.71±6.47 | 17.71±5.22 | 0.0218* | |
| ALT | DD (N=5) | 27±14.2 | 19.6±5.03 | 0.1989 |
| ID (N=9) | 14±4.97 | 14.22±6.63 | 0.8695 | |
| II (N=7) | 20.86±13.63 | 16±6.3 | 0.2162 | |
| SBP | DD (N=5) | 121.2±7.79 | 120.4±8.26 | 0.8620 |
| ID (N=9) | 121.44±12.24 | 115.22±8.84 | 0.1947 | |
| II (N=7) | 121.86±6.28 | 121.14±13.18 | 0.9131 | |
| DBP | DD (N=5) | 77.6±5.03 | 71.4±8.32 | 0.2314 |
| ID (N=9) | 77.44±8.82 | 73.11±8.55 | 0.2146 | |
| II (N=7) | 76.14±7.95 | 75.29±12.63 | 0.8768 | |
| PR | DD (N=5) | 79±16.09 | 83.4±8.59 | 0.5296 |
| ID (N=9) | 72.44±7.06 | 73.22±8.32 | 0.8271 | |
| II (N=7) | 86.14±9.87 | 78.71±10.73 | 0.1764 | |
| RR | DD (N=5) | 1.14±0.06 | 1.18±0.07 | 0.1879 |
| ID (N=9) | 1.16±0.05 | 1.16±0.07 | 0.3559 | |
| II (N=7) | 1.26±0.35 | 1.19±0.05 | 0.6647 | |
ACE, angiotensin I converting enzyme; BW, body weight; BMI, body mass index; RMR, resting metabolic rate; WC, waist circumference; WHR, waist hip ratio; BF%, percentage of body fat; BFM, body fat mass; FI, food intake; BBT, basal body temperature; KOQOL, Korean obesity quality of life; BST, blood sugar test; TG, triglyceride; HDL, high density lipoprotein; T-Chol, total cholesterol; BUN, blood urine nitrogen; Cr, creatinine; AST, aspartate aminotransferase; ALT, aminotransferase; SBP, systolic blood pressure; DBP, diastolic blood pressure; PR, pulse rate; RR, RR interval.
1) p-value derived from paired t-test between pre and post.
* p<0.05.
Safety evaluation of Korean red ginseng
For the safety evaluation of KRG, blood tests on liver function and renal function were carried out before and after drug administration, and BP and heart rate were measured in every visit. In the blood tests for the evaluation of the liver and renal functions before and after KRG, AST was statistically significantly reduced (p=0.0033), while there was no significant difference in the rest, including BUN, creatinine, and ALT. Also, in the comparison with the placebo group, there was no significant difference. In the comparison of BP and heart rate before and after KRG administration, there was no significant difference between KRG group and placebo group (Table 10). To check adverse event of KRG intake, an interview-style medical examination was carried out every second week. During the 8 week study, there were no adverse events in the KRG and placebo groups.
Table 10.
Changes for safety outcome variables
| Variables | Red ginseng | Placebo | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| No. | Mean±SD | p-value1) | No. | Mean±SD | p-value2) | |
|
| ||||||
| BUN at baseline | 22 | 12.65±3.2 | 23 | 12.07±2.96 | 0.5273 | |
| Week 8 - baseline | 22 | 0.29±3.04 | 0.6627 | 23 | 1.79±3.49 | 0.1319 |
| Cr at baseline | 22 | 0.66±0.1 | 23 | 0.66±0.09 | 0.9218 | |
| Week 8 - baseline | 22 | 0±0.05 | 0.7217 | 23 | -0.02±0.05 | 0.1444 |
| AST at baseline | 22 | 20.05±5.58 | 23 | 25.65±12.07 | 0.0526 | |
| Week 8 - baseline | 22 | -2.68±3.8 | 0.0033* | 23 | -3.74±9.1 | 0.612 |
| ALT at baseline | 22 | 19.14±11.37 | 23 | 29.7±16.17 | 0.0154* | |
| Week 8 - baseline | 22 | -3.27±7.92 | 0.0663 | 23 | -5.3±8.42 | 0.4097 |
| SBP at baseline | 22 | 122.18±9.46 | 23 | 123.61±9.91 | 0.6241 | |
| Week 8 - baseline | 22 | -2.86±13.09 | 0.3164 | 23 | -1.43±10.57 | 0.6883 |
| DBP at baseline | 22 | 77.23±7.32 | 23 | 77.61±7.4 | 0.8629 | |
| Week 8 - baseline | 22 | -3.86±10.75 | 0.1068 | 23 | -1.13±6.92 | 0.3142 |
| PR at baseline | 22 | 78.27±11.55 | 23 | 74.43±6.69 | 0.1841 | |
| Week 8 - baseline | 22 | -1.05±12.2 | 0.6919 | 23 | -2.13±9.36 | 0.7388 |
BUN, blood urine nitrogen; Cr, creatinine; AST, aspartate aminotransferase; ALT, aminotransferase; SBP, systolic blood pressure; DBP, diastolic blood pressure; PR, pulse rate.
1) p-value derived from paired t-test between pre and post.
2) p-value derived from Student’s t-test between red ginseng group and placebo group.
*p<0.05.
Confirmation of the appropriateness of blind test for the subjects
To check the appropriateness of the blinding for the subjects after the clinical trials, a self-questionnaire was distributed to inquire on subjects’ perceptions of whether they received KRG or placebo. As a result, 18 (81.8%) of the 22 subjects who completed the test and who had been assigned to KRG group responded that they thought that they had taken the KRG, while four (18.2%) responded that they thought that they had taken the placebo. Of the 23 subjects who had completed the test and who had been assigned to placebo group, 16 (69.6%) responded that they had taken the KRG while seven (30.4%) responded that they thought that they had taken placebo.
DISCUSSION
The effects of KRG on the improvements of obesity and abnormal metabolism have been proven in several studies. KRG extract injected in mice with obesity caused by high fat diet prevented weight increase and increases in and subcutaneous fat and adipocyte size [15]. KRG saponin administered to mice with obesity caused by high fat diet reduced body weight, diet intake, body fat, and serum leptin density and controlled expression of neuropeptide Y in the hypothalamus [10]. Clinical studies have reported administration of KRG complex significantly influences weight and body fat losses compared to placebo and increased beta-adrenergic activity [16], that complex exercises and the injection of KRG complex reduces the percentage of body fat, weight, and serum lipid profile of obese women in their 20s [14,16], and that the risk factors of obesity, hypertension, and arteriosclerosis are restrained in people who consume ginseng for a long time (about 4-5 yr) compared to those who had not [17].
In this study, before and after administration, two subjects in the KRG group (9.09%) displayed >5% weight loss, while none of those in the placebo group displayed comparable weight loss. However, the difference was not statistically significant. In the KRG group, when obesity indices before and after drug administration were compared, weight, BMI, WHR, FI, KOQOL, and AST showed statistically significant decreases. However, except for KOQOL, there was no significant difference from those of the placebo group. Thus, the effects of KRG on the improvement of obesity were confirmed to some extent, although distinct effects on the improvement compared to placebo group were not confirmed.
The KOQOL evaluation is a method of evaluating the quality of life through a self-answered questionnaire consisting of 15 questions in six areas regarding mental and social health, physical health, job work and housekeeping, daily life, sexual relations, and food, which is known to be very reliable and relevant [14]. Unlike other indices of anthropometric assessment and blood test, since this quality of life evaluation is subjective, bias by placebo effects is very likely to occur. However, in the examination of the appropriateness of the blinding on the subject carried out after the test period in this study, it turned out to be maintained relatively well. Therefore, it can be interpreted that KRG is more effective for improving the secondary issues of the quality of life derived from obesity rather than has direct effects on the obesity-related anthropometric assessment and blood test indices.
However, existing studies on obesity related to KRG report significant effects on anthropometric assessment and blood test indices also. There are several reasons for the contradictory results in this study. The KRG powder capsule provided in this study was 500 mg, so consumption of a dose of 6 g required 12 capsules to be taken. This may have lowered compliance, lessening the effects of KRG on the improvement of obesity. However, as leftover drugs had to be returned, compliance could be checked. The compliance rate exceeded 80%. However, drug return was voluntary, so the actual compliance rate is unclear.
In the GNB3 gene, C825T gene polymorphism is related to obesity. The T allele of the GNB3 gene is associated with increased intra-cellular signal transduction and renin activity and has been implicated in diseases such as arterial hypertension and obesity [18]. Possession of the T allele increases the heart’s stroke volume and renal flow, which greatly increases the prevalence rate of hypertension and cardiovascular diseases [19]. BMI 25 is 2 to 3 times higher in people with T allele than in the C allele [17]. Domestic studies include reports of significant differences by GNB3 gene polymorphism in the improvements of Korean middle-aged women’s weight, triglycerides, HDL, insulin and HOMA index by aerobic exercises [20]. In contrast, in one study, GNB3 polymorphism did not have anything significant to do with the BP, obesity indices, serum lipid profile, and obesity-related protein for Korean middle-aged women [21].
This study confirmed that the BMI, BF%, and systolic BP pressure of subjects with GNB3 gene mutation (CT+TT) was significantly higher than that without the mutation (CC). This result is consistent with previous studies, in which the T allele increased the risk of obesity [17-19]. In the CT type with heterogenous mutation, systolic BP was significantly reduced by KRG, while in the mutation-free CC type there was no significant change. Moreover, in the latter, compared to CT type, although food intake was much more significantly reduced, there was a more significant change in the CT type for the above two items. Thus, the effects of KRG on the improvement of obesity were more pronounced for those whose energy metabolism was reduced by the presence of a GNB3 gene mutation.
The ADRB3 gene is expressed in fat tissues, which, in humans, mainly exists in brown fat tissues and in white adipose tissue after growth [22]. Its function has not been clearly proven yet. However, it is known to activate heat generation in the brown adipose tissue and to stimulate lipolysis in the white adipose tissue as a G protein-associated receptor, and this energy controlling function is known to be related to obesity [23,24]. If ADRB3 gene mutation is homogenous, there is low basal metabolism and high BMI, and it accelerates the age of onset of diabetes [25]. But, the phenotype of obesity differs depending on the race. In a study on Finnish men [26] and French men [27] ADRB3 gene polymorphism produced a significant increase of the risk of obesity or metabolic diseases in heterogeneous mutation as well as homogenous mutation. However, in a study on Mexican Americans [28], only homogenous mutation was associated with significantly increased risks of obesity or metabolic diseases. In Korea, a comparison of middle-aged women’s body constitution and serum lipid profile density after exercise treatment by ADRB3 gene polymorphism reported no significant difference [29], and in a comparative study on reactions to Orlistat drug administration by ADRB3 gene polymorphism mutation, weight, WC, and BMI tended to be reduced more than in non-mutation group, although the difference was statistically insiginificant [30].
In this study, the group with heterogeneous mutation of the ADRB3 gene (Trp64/Arg) had significantly lower HDL than that without mutation (Trp64/Trp), so the risk of metabolic diseases was increased when there was a gene mutation. However, the difference by genotype was not confirmed in the rest of the obesity indices. Since other related studies [29,30] have reported a lack of correlation between the mutation of ADRB3 gene and obesity response, it is conceivable that the association of ADRB3 gene polymorphism with obesity is weaker in Koreans than other races. Also, in this study, since there were only five subjects with the Arg64/Arg type of homogenous mutation, the difference by gene polymorphism might not been apparent in the obesity indices.
The ACE gene product is secreted from endotheliocytes in the kidney. It converts angiotensin I to angiotensin II, and reduces the vasodilator bradykinin, which is related to the density of ACE enzyme that plays an important role in controlling of the homeostasis of circulatory functions. If serum ACE level increases, blood vessel is contracted. And that elevates BP and the risks of myocardial infraction. Consequently coronary artery disease increase. If the ACE gene is deficient, the density of serum ACE level increases. It has been reported that people with II gene type display lower BP and higher endurance than people with DD gene type did, while the risk of cardiovascular diseases of those with DD gene type is increased [31]. Also, a study on type 2 diabetics in China reported that DD type was associated with higher triglycerides [32] and the serum ACE level of obese people was higher than that of those who were not [33]. The athletic ability of Koreans with the ACE gene type with the ID or DD mutation tends to be less and they are more likely to be obese [34-37]. This study, unlike existing study results, was not able to confirm the significant relationship between the ACE gene polymorphism and the obesity indices. Since this study set obesity patients as the target of study, already all samples were acquired from an obese subject. Accordingly, it is supposed that there was no difference of phenotype by gene polymorphism. When the effects of KRG on the improvement of obesity were compared to ACE gene polymorphism, there were significant effects on improvement by the evaluation on the KOQOL scale only in the DD type (homogeneous mutation), while a decreasing tendency only was found in the ID type (heterogeneous mutation) and the II type (without mutation). However, in the remainder of the obesity indices, it was not confirmed that the treatment effects of KRG differed depending on gene polymorphism.
The safety of KRG has been documented in a variety of studies. Also, since in this study there was no significant change in the comparison of blood tests (AST, ALT, BUN, and creatinine) before and after KRG administration, and there was no report of special adverse event during the 8-week clinical trials, the safety of the administration of KRG of 18 g a day (three times, 6 g each) for 8 wk could be reconfirmed.
A pharmacogenomic study tries to explain individual differences of drug reactions by genetic differences, of which importance has been relatively recently recognized and a field in which active studies are in progress. Pharmacogenomic studies not only make it more effective individualized custom treatment possible, by understanding the differences of drug reactions according to the genetic characteristics of individuals, but also predict adverse events of the drugs, so that they will be able to used more safely. In addition, such studies can enhance the success rate and shorten the time required through efficient clinical trials in developing new medicines. Also, through pharmacogenomic studies, the mechanisms of onset of some genetic diseases can be understood, so that they can be prevented. This study is also a kind of pharmacogenomic study, which tried to examine the differences of the effects of KRG on the improvement of obesity by gene mutation. This study has not clearly proved the differences in the effects of KRG on the improvement of obesity by gene. However, it has strengths of randomization, double blinding, and placebo control.
Acknowledgments
This work was supported by the 2010 grant from the Korean Society of Ginseng funded by Korea Ginseng Corporation.
References
- 1.Kim MS. Modulation factors of energy metabolism. Korean J Obes. 2000;9:6–11. [Google Scholar]
- 2.Hong SK. Energy balance and obesity. Korean J Obes. 2000;9:1–5. [Google Scholar]
- 3.Kim SJ, Shin SW, Kim HJ. Obesity from the view point of metabolic rate. J Korean Orient Assoc Stud Obes. 2003;3:95–105. [Google Scholar]
- 4.Beck SH. Obesity related gene variations. Korean J Obes. 2004;13:221–229. [Google Scholar]
- 5.Association of School of Herbology. Herbology. Younglim; Seoul: 2000. [Google Scholar]
- 6.Hong B, Ji YH, Hong JH, Nam KY, Ahn TY. A double-blind crossover study evaluating the efficacy of Korean red ginseng in patients with erectile dysfunction: a preliminary report. J Urol. 2002;168:2070–2073. doi: 10.1016/S0022-5347(05)64298-X. [DOI] [PubMed] [Google Scholar]
- 7.Suh SO, Kroh M, Kim NR, Joh YG, Cho MY. Effects of red ginseng upon postoperative immunity and survival in patients with stage III gastric cancer. Am J Chin Med. 2002;30:483–494. doi: 10.1142/S0192415X02000661. [DOI] [PubMed] [Google Scholar]
- 8.Sung H, Jung YS, Cho YK. Beneficial effects of a combination of Korean red ginseng and highly active antiretroviral therapy in human immunodeficiency virus type 1-infected patients. Clin Vaccine Immunol. 2009;16:1127–1131. doi: 10.1128/CVI.00013-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Park HJ, Lee JH, Lee SJ, Ham HS, Cho HJ, Lim CR, Yoo YB, Park KH. Effects of intaking of red ginseng products on correlationship between obesity and blood lipids. J Biomed Lab Sci. 2000;6:253–260. [Google Scholar]
- 10.Han YJ, Kim JH. Effect of crude saponin of Korea red ginseng on high fat diet-induced obese rats. J Korean Orient Med. 2006;27:1–13. [Google Scholar]
- 11.Kim SS, Kim JD, Kim H, Shin MS, Park CK, Park MH, Yang JW. The effects of red ginseng product and combined exercise on blood lipids and body composition of obese women in their twenties. J Ginseng Res. 2002;26:59–66. doi: 10.5142/JGR.2002.26.2.059. [DOI] [Google Scholar]
- 12.Seong JH, So NU, Jeon BH, Jang JC. Effect of white and red Panax ginseng extract on serum lipids level in high-fat-diet fed rats. J Ginseng Res. 2004;28:33–38. doi: 10.5142/JGR.2004.28.1.033. [DOI] [Google Scholar]
- 13.Oh SJ, Kim YS, Park CY, Kim SW, Yang IM, Kim JW, Choi YK, Paeng JR, Shin HD. Body fat decreasing mechanisms of red ginseng compound. Korean J Obes. 2000;9:209–218. [Google Scholar]
- 14.Park HS, Sung SW, Ou SW, Lee KY, Kim BS, Han JH, Kim SM, Lee HR, Yu BY, Lee KM, et al. Development of Korean version of obesity-related quality of life scale. Korean J Obes. 2003;12:280–293. [Google Scholar]
- 15.Kim SI, Kim YS, Jeon BS, Lim CH. Effect of ginseng on fat accumulation in the obese rats induced by high fat diet. Korean J Ginseng Sci. 1986;10:167–179. [Google Scholar]
- 16.Kim SS, Park HY, Byun YH, Hwang BG, Lee JH, Shim YJ, Park CK, Park MH, Yang JW. The effects on the blood lipid profiles and body fat by long term administration of red ginseng product. J Ginseng Res. 2002;26:63–73. [Google Scholar]
- 17.Ohshiro Y, Ueda K, Wakasaki H, Takasu N, Nanjo K. Analysis of 825C/T polymorphism of G proteinbeta3 subunit in obese/diabetic Japanese. Biochem Biophys Res Commun. 2001;286:678–680. doi: 10.1006/bbrc.2001.5450. [DOI] [PubMed] [Google Scholar]
- 18.Choi H, Bae HS, Hong MC, Shin HD, Shin MK. Study of gene-gene interaction within GNB3, ACE, ADRB3, ADRB2 among Korean female subject. Korean J Orient Med Physiol Pathol. 2004;18:1426–1436. [Google Scholar]
- 19.Zeltner R, Delles C, Schneider M, Siffert W, Schmieder RE. G-protein beta(3) subunit gene (GNB3) 825T allele is associated with enhanced renal perfusion in early hypertension. Hypertension. 2001;37:882–886. doi: 10.1161/01.hyp.37.3.882. [DOI] [PubMed] [Google Scholar]
- 20.Woo SG, Jung SH, Han TK. Effect of an aerobic exercise on obesity and metabolic syndrome markers across the GNB3 C825T genotype in obesity middle age women. J Korean Soc Living Environ Syst. 2008;15:392–399. [Google Scholar]
- 21.Kang HS, Lee JY, Han TK. Relationship of the GNB3 C825T gene polymorphism with the metabolic syndrome markers in mid-life women. Korean J Sport Sci. 2006;17:1–8. [Google Scholar]
- 22.Giacobino JP. Beta 3-adrenoceptor: an update. Eur J Endocrinol. 1995;132:377–385. doi: 10.1530/eje.0.1320377. [DOI] [PubMed] [Google Scholar]
- 23.Lowell BB, Flier JS. Brown adipose tissue, beta 3-adrenergic receptors, and obesity. Annu Rev Med. 1997;48:307–316. doi: 10.1146/annurev.med.48.1.307. [DOI] [PubMed] [Google Scholar]
- 24.Choi WH. Role of beta3 adrenreceptor. Korean J Obes. 2001;10:205–216. [Google Scholar]
- 25.Walston J, Silver K, Bogardus C, Knowler WC, Celi FS, Austin S, Manning B, Strosberg AD, Stern MP, Raben N, et al. Time of onset of non-insulin-dependent diabetes mellitus and genetic variation in the beta 3-adrenergicreceptor gene. N Engl J Med. 1995;333:343–347. doi: 10.1056/NEJM199508103330603. [DOI] [PubMed] [Google Scholar]
- 26.Widen E, Lehto M, Kanninen T, Walston J, Shuldiner AR, Groop LC. Association of a polymorphism in the beta 3-adrenergic-receptor gene with features of the insulin resistance syndrome in Finns. N Engl J Med. 1995;333:348–351. doi: 10.1056/NEJM199508103330603. [DOI] [PubMed] [Google Scholar]
- 27.Clement K, Vaisse C, Manning BS, Basdevant A, GuyGrand B, Ruiz J, Silver KD, Shuldiner AR, Froguel P, Strosberg AD. Genetic variation in the beta 3-adrenergic receptor and an increased capacity to gain weight in patients with morbid obesity. N Engl J Med. 1995;333:352–354. doi: 10.1056/NEJM199508103330605. [DOI] [PubMed] [Google Scholar]
- 28.Silver K, Mitchell BD, Walston J, Sorkin JD, Stern MP, Roth J, Shuldiner AR. TRP64ARG beta 3-adrenergic receptor and obesity in Mexican Americans. Hum Genet. 1997;101:306–311. doi: 10.1007/s004390050633. [DOI] [PubMed] [Google Scholar]
- 29.Cheon WK, Kim KJ. Association of mutation in the beta- 3 adrenergic receptor gene with obesity response to diet plus exercise intervention in middle-aged women. Korean J Exerc Nutr. 2007;11:41–48. [Google Scholar]
- 30.Seo YS, Kim DH, Lee IG, Lee GM, Kim YH. Effect of variants of the β-3 adrenergic receptor and the leptin receptor gene on weight loss. Korean J Obes. 2003;12:294–303. [Google Scholar]
- 31.Gayagay G, Yu B, Hambly B, Boston T, Hahn A, Celermajer DS, Trent RJ. Elite endurance athletes and the ACE I allele: the role of genes in athletic performance. Hum Genet. 1998;103:48–50. doi: 10.1007/s004390050781. [DOI] [PubMed] [Google Scholar]
- 32.Lee YJ, Tsai JC. ACE gene insertion/deletion polymorphism associated with 1998 World Health Organization definition of metabolic syndrome in Chinese type 2 diabetic patients. Diabetes Care. 2002;25:1002–1008. doi: 10.2337/diacare.25.6.1002. [DOI] [PubMed] [Google Scholar]
- 33.Cooper R, McFarlane-Anderson N, Bennett FI, Wilks R, Puras A, Tewksbury D, Ward R, Forrester T. ACE, angiotensinogen and obesity: a potential pathway leading to hypertension. J Hum Hypertens. 1997;11:107–111. doi: 10.1038/sj.jhh.1000391. [DOI] [PubMed] [Google Scholar]
- 34.Lee SJ, You JH, Lee JK. A study of characteristics on health-related physical fitness factors and blood variables according to ACE I/D polymorphism in mid-life obese women. Korean J Exerc Nutr. 2007;11:207–212. [Google Scholar]
- 35.Seo HN, Kim YJ, Moon SJ, Jeong JG. Effects of aerobic excercise on ACE and risk factors of cardiovascular system of middle-aged women according to the existence and nonexistence of metabolic syndrome. Korean J Sports Sci. 2010;19:1275–1286. [Google Scholar]
- 36.Ham YG. Effects of ACE gene polymorphism and dance sports on blood pressure. Korean J Exerc Nutr. 2008;12:133–137. [Google Scholar]
- 37.Jung SJ, Ahn NY, Hong CB, Park JH, Park JS, Kim KJ. Comparisons of body composition, physical fitness and combined exercise training mediate changes according to ACE I/D polymorphism in elementary students. Korean J Growth Dev. 2009;17:259–266. [Google Scholar]