

Therapeutic angiogenesis, the treatment of tissue ischemia by promoting the proliferation of new blood vessels, has recently emerged as a promising therapy. This article discusses different physiological aspects of neovascularization, presents cells isolated from the blood and bone marrow with endothelial cell properties, and discusses isolation and cell culture strategies, phenotype, functional capabilities, and possible therapeutic applications of angiogenic cells obtained from adipose tissue.
Keywords: Angiogenesis, Adipose tissue, Endothelial cells, Cellular therapy, Mesenchymal stem cells
Abstract
Inadequate blood supply to tissues is a leading cause of morbidity and mortality today. Ischemic symptoms caused by obstruction of arterioles and capillaries are currently not treatable by vessel replacement or dilatation procedures. Therapeutic angiogenesis, the treatment of tissue ischemia by promoting the proliferation of new blood vessels, has recently emerged as one of the most promising therapies. Neovascularization is most often attempted by introduction of angiogenic cells from different sources. Emerging evidence suggests that adipose tissue (AT) is an excellent reservoir of autologous cells with angiogenic potential. AT yields two cell populations of importance for neovascularization: AT-derived mesenchymal stromal cells, which likely act predominantly as pericytes, and AT-derived endothelial cells (ECs). In this concise review we discuss different physiological aspects of neovascularization, briefly present cells isolated from the blood and bone marrow with EC properties, and then discuss isolation and cell culture strategies, phenotype, functional capabilities, and possible therapeutic applications of angiogenic cells obtained from AT.
Introduction
Inadequate blood supply to tissues is a leading cause of morbidity and mortality today. Narrowing of the vessels of the arterial tree may be caused by a range of diseases and environmental factors, with slightly different sets of etiological factors affecting large and medium-sized arteries and arterioles [1]. Obstructions of large and medium-sized arteries are frequently amenable to surgical or endovascular repair procedures. However, some of these procedures require the replacement of obstructed vessels with patent vessels obtained from other parts of the patient. The availability of redundant vessels is obviously limited. This has opened up a very active research field where the aim is to create arterial vessels by tissue engineering using biomaterials and autologous cells [2]. Further down the arterial tree, ischemic symptoms caused by obstruction of arterioles and capillaries are currently not treatable by replacement or dilatation procedures [3]. These symptoms most commonly occur in the limbs, where the disorder is called peripheral vascular disease (PVD), and in the heart, where arteriolar obstruction is one of the causes of refractory angina pectoris. Attempts to treat PVD using angiogenic factors such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), or hepatocyte growth factor (HGF) have been disappointing [4]. Over the past decade, researchers have turned to the use of cells in attempts to produce neovascularization of ischemic tissues [5, 6]. In this concise review we briefly describe the mechanisms involved in de novo blood vessel formation, summarize the results of clinical trials using cells to treat microvascular tissue ischemia, and then focus on adipose tissue as a source of cells with therapeutic angiogenic potential.
Neovascularization-De Novo Blood Vessel Formation
Formation of new blood vessels is a complex and integrated process that is not yet completely understood. It is important during embryological organogenesis, in the course of organ growth after birth, in the course of restoration of blood supply to ischemic tissues, and in the establishment of blood supply to tumors [5].
Neovascularization is the term used for the physiological processes of angiogenesis, vasculogenesis, and arteriogenesis, which represent different aspects of this complex process (Fig. 1). In angiogenesis, new microvessels are generated from pre-existing vasculature by the proliferation and migration of endothelial cells (ECs). These vessels play an important part in the repair mechanism of damaged tissues [5]. Hypoxia is an important stimulus for the expansion of the vascular bed, particularly through the effects of hypoxia-inducible factors (HIFs) [7]. HIFs upregulate angiogenic factors such as VEGF, which stimulate both physiological and pathological angiogenesis. Vasculogenesis, on the other hand, refers to the formation of blood vessels by the recruitment and differentiation of undifferentiated endothelial progenitor cells at the site of new vessel growth [5]. This process is regulated by growth factors such as VEGF, FGF, transforming growth factor, and angiopoietin-1 and by their receptors, including VEGF receptor 1 (VEGFR1/FLT1), VEGFR2 (KDR/FLK1), and Tie-2 [8]. Until recently, the term vasculogenesis was used only to describe blood vessel formation in the embryo. However, this process has now also been shown to contribute to adult blood vessel formation [9, 10]. Arteriogenesis involves the expansive growth of collateral arteries by sprouting of pre-existing vessels to form collateral bridges between arterial networks via the migration and proliferation of ECs and smooth muscle cells (SMCs) [5]. Although endothelial remodeling plays a major role both in angiogenesis and arteriogenesis, the two processes are separated by the involvement of SMCs.
Figure 1.

The processes of angiogenesis, vasculogenesis, and arteriogenesis. New microvessels are generated from pre-existing vasculature by the proliferation and migration of mature ECs in the classic process of new vessel growth, angiogenesis. Vasculogenesis involves participation of undifferentiated EPCs, which circulate to sites of new vessel growth, where they differentiate into mature ECs. Arteriogenesis involves the expansive growth of collateral arteries by sprouting of pre-existing vessels to form collateral bridges between arterial networks via the migration and proliferation of ECs and SMCs. Growth factors and cytokines released endogenously in response to tissue ischemia act to promote neovascularization. Abbreviations: Ang 1, angiopoietin-1; EC, endothelial cell; EPC, endothelial progenitor cell; FGF, fibroblast growth factor; HIF, hypoxia-inducible factor; SMC, smooth muscle cell; VEGF, vascular endothelial growth factor.
Endothelial Cells in Bone Marrow and Peripheral Blood
During embryogenesis, endothelial and hematopoietic lineages have common lineage precursors [11]. These common precursors, sometimes called hemangioblasts, are located in embryonic vessel walls at least through part of embryonic development [11]. The exact phenotype and anatomical localization of the latest stage of common hemoendothelial precursors are not known. In adult humans, hematopoiesis takes place in the bone marrow. This has been one of the strong arguments used to suggest that endothelial precursor cells (EPCs) would also be found in the bone marrow [12]. The phenotype of these cells was unknown until a population of EPCs was first isolated from human peripheral blood by Asahara et al. by magnetic bead selection based on the cell surface marker expression of CD34 and VEGFR2 [13]. Besides the surface marker-based selection approaches, cell culture and colony formation assays have been used to isolate and characterize EPCs [14]. The identification and characterization of those cells still remain challenging and controversial. The term EPCs describes a mixed cell population that consists of different progenitors. Through phenotypic analyses and functional studies it has been shown that some of these progenitors reside in the bone marrow [15]. EPCs adhere to matrix molecules such as fibronectin, take up acetylated low-density lipoprotein (LDL), and bind Ulex europaeus agglutinin-I lectin (UEA-1) [13]. In animal models of ischemia—both in mice and in rabbits—mobilization of EPCs can promote new blood vessel formation in injured areas, enhance perfusion, and lead to recovery of the ischemic tissue [16, 17]. Thus, EPCs incorporate into sites of active angiogenesis in vivo, indicating that they may also be useful for human therapeutic angiogenesis. Further investigation established that there are two distinct EPC populations with different growth characteristics, referred to as early- and late-outgrowth EPCs [18]. These cells are most frequently isolated from peripheral blood, and as the names imply, they proliferate at different time points in EPC culture assays on fibronectin or gelatin [14]. The early outgrowth EPCs have lower levels of the surface markers KDR and CD144 and produce more cytokines, but both populations form functional blood vessels upon subcutaneous implantation in Matrigel (BD Biosciences, San Diego, CA, http://www.bdbiosciences.com) plugs in immunodeficient rodents [14, 19]. Thus, they may constitute a useful source of cells for therapeutic transplantation into ischemic areas. However, they are found at extremely low precursor frequencies within human peripheral blood and require prolonged in vitro cell expansion in order to obtain the numbers required for cell therapy.
Recently a population of ECs with colony forming capabilities, endothelial colony forming cells (ECFCs), was isolated directly from unmanipulated human blood on the basis of attachment to uncoated plastic surfaces in a growth medium supplemented with pooled human platelet lysate [20]. These ECs were expandable to high numbers in cell factories. The cells expressed endothelial markers such as CD31, KDR, CD144, CD105, von Willebrand factor (vWF), and CD146 and took up DiI complex acetylated LDL, but in contrast with the early EPCs, they did not express the hematopoietic markers CD45 and CD14 [20]. The ECFCs formed vessels in Matrigel in vivo. The ECFCs are quite easily obtained from peripheral blood but require prolonged in vitro cell culture to obtain the numbers required for therapeutic neovascularization. However, as the culture system is fully humanized, the ECFCs may soon be candidates for therapeutic trials.
Adipose Tissue as a Source of Cells with Angiogenic Potential
Adult adipose tissue (AT) is one of the largest and most plastic tissues in the body. AT is the source of a range of hormones and cytokines, is a main reservoir of energy, and frequently goes through periods of expansion and shrinkage. Not surprisingly, AT is one of the most highly vascularized tissues in the body. A very close anatomical and physiological relationship has been demonstrated in AT between blood vessels, perivascular cells, and adipocyte precursor cells [21]. Mesenchymal stromal cells (MSCs) may differentiate to adipocytes and may be the earliest adipocyte precursor cells in AT. However, MSCs also have a role as perivascular cells, thus stabilizing new blood vessels [22, 23]. At the same time, the vasculature may have a causal role in the physiological functions of AT by controlling the number of microvessels and by remodeling existing vessels. Indeed, angiogenesis has been shown to be of great importance for the modulation of adipogenesis and obesity [24]. Thus, AT is an easily available, sometimes greatly superfluous tissue where new blood vessels are constantly being made in adult life.
The availability of ample amounts of tissue has generated a search for interesting and useful cell populations within AT. For this, variable amounts of liposuction material can be collected under local anesthesia by minimally invasive interference. After removal of blood from the liposuction material, the connective tissue keeping the remaining tissue together is digested using collagenase. Adipocytes, which make up the majority of the bulk of this tissue, are separated from other cells by gentle centrifugation. The pellet recovered from this centrifugation step is called the stromal vascular fraction (SVF) of AT. Analysis of SVF revealed that AT is a source of cells with multilineage differentiation potential [25, 26]. However, it soon became clear that SVF is, in fact, a heterogeneous population of cells. Several markers can be used to distinguish the populations contained within SVF, but the most useful may be CD31 and human leukocyte antigen (HLA) DR, which are molecules normally expressed on ECs. Upon phenotypic characterization of SVF, these molecules separate SVF cells into two populations: those coexpressing CD31 and HLA DR, approximately 20%–40% of the SVF, and those expressing neither of these [27]. After some weeks of in vitro culture, the plastic-adherent CD31− HLA DR− population expressed surface markers typical of MSCs [28]. These cells are frequently called adipose tissue-derived stem cells (ADSCs or ASCs), although we prefer to call them adipose tissue-derived mesenchymal stromal cells (AT-MSCs) to mark their ontogenetic relationship to bone marrow (BM) MSCs and at the same time distinguish them from other stem cells that may be found within the SVF. Transcription profiling analysis shows that the CD31+ HLA-DR+ cells within SVF overexpress transcripts associated with both arterial and venous endothelium and mostly resemble microvascular cells [27]. Under the culture conditions used in this study, which were optimized for MSC culture with Dulbecco's modified Eagle's medium/Ham's F-12 medium and no gelatin coat on the plastic surface, the CD31+ SVF cells did not proliferate in vitro. Later we successfully isolated and in vitro expanded CD31+ cells from AT using other cell culture conditions and showed that these were indeed bona fide ECs [29].
Neovascularization Potential of AT-MSCs
AT-MSCs may be obtained in high numbers from SVF by removal of CD31+ cells [27]. In fact, the frequency of MSCs within mononuclear cells from AT is at least 500-fold higher than in mononuclear cells from bone marrow [30], yielding sufficient numbers of uncultured AT-MSCs to allow phenotypic and molecular characterization. Comparisons of uncultured AT-MSCs with their culture-expanded offspring showed that plastic-adherent cell culture induced considerable differences in gene expression and surface molecules [27]. Most notable, perhaps, was the expression of CD34 by practically all the uncultured AT-MSCs. This molecule, which is also expressed at low levels by most ECs, was lost over the first few passages of plastic-adherent cell culture. Thus, culture-expanded adipose-derived stem cells appear as a relatively homogeneous population. They adhere to the definition of MSCs provided by the International Society for Cell Therapy based on their phenotype (CD73+, CD90+, CD105+, CD11b/CD14−, CD19/CD73b−, CD34−, CD45−, HLA DR−); their plastic-adherent properties; and their multipotent differentiation potential to adipogenic, chondrogenic, and osteogenic lineages [28]. Based on their differentiation capabilities, AT-MSCs are being used today for breast re-establishment and enlargement surgery and for tissue engineering of cartilage and bone. However, their role in therapeutic neovascularization procedures is still unclear [31].
The CD31− population of SVF expresses very much lower levels of mRNAs encoding EC molecules such as CD144, CD31, vWF, VEGFR2, and VEGFR1 than does the uncultured CD31+ subset of SVF [27]. At the same time, the CD31− cells secrete a range of soluble factors. Some, such as VEGF and HGF, are known to promote neovascularization [32]. Using the mouse ischemic hind limb model to determine the neovascularization potential, the stromal cell fraction of mouse and human SVF was found to improve angiogenesis mainly by the secretion of angiogenic growth factors [33]. Similar mechanisms were shown to act when rat AT-MSCs protected skin flaps against ischemia-reperfusion injury [34]. However, other investigators showed that injected AT-MSCs improved the ischemic score also by differentiation to CD31+ ECs within ischemic tissues [35–37]. Yet other studies failed to demonstrate the differentiation of adipose-derived cells toward the endothelial lineage [38], possibly because of differences in passage number and culture conditions. Then, in 2008, a number of studies appeared that suggested that MSC populations derive from blood vessel walls and that they may be identical to the pericytes [22, 39, 40]. A landmark paper by Crisan et al. described the in situ and in vitro links between MSCs and pericytes, identifying a population of CD146hiCD34−CD45−CD56− cells as pericytes in several tissues [22]. These cells also expressed the classic MSC markers CD44, CD73, CD90, and CD105 in vivo but did not express endothelial markers CD31, CD144, vWF, or UEA-1. Crisan et al. concluded that cultured perivascular cells from a variety of tissues exhibit a phenotype that is very similar to that of BM-MSCs [22]. Because of their role as pericytes in most tissues, MSCs were now suggested to have an important role in vasculogenesis by stabilizing the vasculature [22, 23, 40–42]. Through interaction with ECs [23], the MSCs are thus able to stimulate angiogenesis [35, 43]. In conclusion, most evidence today suggests that the main role of AT-MSCs in blood vessel biology may be as pericytes to secrete angiogenic factors and stabilize the interactions between ECs.
Endothelial Cells in Adipose Tissue
Based on cell surface expression of CD31 and HLA DR, intracellular expression of vWF, and very high expression of mRNAs typical of ECs, the CD31+ subset of SVF cells was considered to consist of ECs, most likely microvascular ECs [29]. Previously, several attempts had been made to isolate ECs from SVF using plastic attachment techniques and positive selection strategies [44–48]. We recently used a combination of negative and positive immunomagnetic isolation to derive a pure population of CD31+ cells from AT [29]. Depending on the amount of liposuction starting material, several tens of millions of uncultured ECs could be obtained. These cells were readily expandable on a gelatin coat with an endothelial culture medium supplemented with fetal bovine serum (FBS). Later, we replaced the FBS with human plasma supplemented with human platelet lysate (PLP). This has enabled us to culture the ECs directly on plastic surfaces, which means that the culture system is entirely humanized. These AT-ECs proliferate rapidly through at least 15–20 population doublings. Since the starting number of cells is already high, several hundred millions of ECs may be obtained after a relatively brief period of in vitro expansion. The AT-ECs form functional blood vessels in Matrigel following subcutaneous injection into immunodeficient mice. Interestingly, the vessel formation was more dense and robust when AT-ECs were combined with the AT-MSCs, suggesting that the MSCs adopt a supportive role similar to that of pericytes under these conditions [29].
Nevertheless, the identity of the AT-ECs still remains controversial. Since they express CD144 (vascular endothelial cadherin) and vWF but do not express CD133, CD45, or CD14, they are not likely to represent a population of early EPCs [49, 50]. Expression of genetic markers typical of both the arterial and the venous side of capillaries suggests that they may be microvascular endothelial cells (MVECs). However, it has been shown that MVECs strongly express CD141 [51], which was only weakly expressed or absent on AT-ECs. Based on their phenotype (CD34+CD133−vWF+CD144+VEGFR2+endothelial nitric oxide synthase+CD31+), AT-ECs most resemble late outgrowth EPCs or ECFCs [49, 50]. A population of ECFCs isolated from peripheral blood has recently been described [20]. The isolation procedure was different from that used to isolate EPCs [13], and the authors suggested that these cells most closely resemble microvascular cells. In collaboration with this group, we are now performing studies comparing the blood-derived ECFCs and the AT-ECs in terms of gene expression, phenotype, and vessel-forming functionality. This study should also help to clarify the somewhat confusing terminology used for human ECs.
Therapeutic Potential of Adipose Tissue-Derived Angiogenic Cells
AT, then, contains two populations of cells with different functionalities that may contribute to neovascularization: the bona fide ECs and AT-MSCs. These two nonoverlapping populations make up more than 60% of the SVF and may be isolated in large numbers from a relatively small amount of liposuction material. Some clinical studies are based on uncultured SVF [52]. The advantage is that isolation of SVF from liposuction material is a relatively rapid procedure, which in fact may be performed automatically in the operating room [53–55]. The disadvantages are the lower numbers of cells, a relatively uncontrolled mixture of cell populations, and the fact that the functionality of uncultured AT-ECs may be different from culture-expanded AT-ECs [29]. For isolation of pure populations of AT-MSCs and AT-ECs, negative immunomagnetic isolation procedures may be used for both [27, 29]. This leaves no immunomagnetic beads in the resulting cell population, a fact that should make the procedure acceptable for cells to be used for treatment of patients. Both cell populations are readily expandable during in vitro culture, and both may be cultured using human PLP, which makes the entire ex vivo expansion procedure free of xenogeneic proteins. Thus, the ex vivo isolation and culture procedure is likely to be acceptable to national regulatory authorities.
The availability of autologous ECs is likely to be crucially important both for the tissue engineering of arteries and for cell therapy for microvascular disease. Most ECs express HLA class II antigens [56]. Uncultured AT-ECs express HLA II molecules but lose these quickly from the surface upon cell culture [29]. Human AT-MSCs cultured in FBS express HLA II at the mRNA level but not on the surface [27]. However, according to our recent observation, when human PLP is used as a supplement, some of the AT-MSCs express HLA class II antigens. Both of these cell populations are likely to upregulate HLA class II molecules in an inflammatory environment. Thus, allogeneic angiogenic cells are likely to be rejected by an allospecific immune response directed toward their HLA class II molecules. The same may well be the fate for autologous angiogenic cells cultured in FBS, where xenogeneic antigens presented by autologous HLA class II molecules may induce an immune response. Autologous cells expanded in human medium supplements, however, are likely to be well tolerated in a transplantation situation.
However, there are still issues that need to be solved. One such issue is whether there are important phenotypic and functional differences in fat obtained from different sites [57]. The immunomodulatory property of AT-MSCs is also an important issue. It has been shown that AT-MSCs promote engraftment and prevent or treat severe graft-versus-host disease in allogeneic stem cell transplantation [58, 59]. Treatment with immunosuppressive cells might conceivably activate dormant infections or tumors, although results in this area are contradictory [60–63]. Also, in vitro culture of cells could activate transformation pathways and lead to tumor formation. MSCs are known to occasionally form tumors in mice [64], but neither tumors nor ectopic tissue formation following injections of MSCs in humans has been reported after more than 10 years of follow-up [64–66]. Clinical application of AT-MSCs may therefore be considered to be safe. The preclinical and clinical experience with cultured ECs is still limited [67]. Thus, additional studies are needed to fully elucidate the safety and reproducibility of the in vitro expanded AT-ECs.
Based on the ready availability of large numbers of autologous cells, AT-ECs are likely to be attractive EC candidates for scientists involved in tissue engineering of arterial vessels. However, very few clinical trials using cell-based approaches to tissue engineer blood vessels have so far been performed [68]. In contrast, a huge number of clinical trials of stem cell therapy have been performed in attempts to moderate the outcome of another arterial disease, acute myocardial infarction (AMI) [69, 70]. Most of these have used uncultured populations of autologous cells derived from the bone marrow. The results of these trials are so far that “stem/progenitor cell treatment was not associated with statistically significant changes in the incidence of mortality ([relative risk] 0.70, 95% CI 0.40–1.21) or morbidity (the latter measured by reinfarction, hospital readmission, restenosis and target vessel ravascularization)” [69]. It is possible that the treatment outcome could have been improved by injection of autologous cells with angiogenic potential. However, AT-ECs and AT-MSCs need to be cultured in vitro to obtain the number of cells likely to induce neovascularization. This takes several weeks, by which time the acute phase of AMI has passed, and a therapeutic opportunity may have been lost. Cell culture-expanded allogeneic angiogenic cells from AT could be provided to patients in the acute phase of AMI, but as described above, these cells are likely to be rejected by alloimmune responses. Finally, relatively large numbers of uncultured autologous SVF cells may be procured within hours in an acute AMI situation. Human clinical trials using these cells are known to be under way, but no results have yet been published [52].
Ischemic symptoms caused by obstruction of arterioles and capillaries are not accessible to replacement or dilatation procedures and are currently treatable only by cell-based strategies for neovascularization. In the heart, this illness is called refractory angina pectoris. A number of clinical trials have been performed in groups of patients with refractory angina (Table 1). Most of these trials have used mononuclear cells from bone marrow (BM-MNCs). These are uncultured cells in which the fraction of hematopoietic stem cells is less than 1%, and the fraction of EPCs is less than that. However, some recent studies have used cell culture-expanded MSCs (Table 1). All of these studies have reported beneficial effects, some even after long observation periods. The mechanism of the beneficial effect is uncertain. In fact, cells injected into the heart usually do not remain there very long; they migrate to the lung, spleen, and other organs [71]. Those cells that remain in the heart usually die or do not function. There may be several explanations for this. To survive, cells need the appropriate signals from their environment. This is particularly important for cells expanded in vitro adherent to molecules on plastic surfaces. These environmental signals may not be available in the myocardium. Also, cells injected into ischemic myocardium may find the microenvironment too hostile to promote survival. Recently we injected several different populations of human MSCs into the border zones of 1-week-old myocardial infarctions in immunodeficient rats [72]. They all induced surprisingly good functional improvement. At 4 weeks, only a small fraction of the injected cells could be recovered in the murine myocardium. This study and all other studies reporting beneficial effects of cells injected into ischemic hearts suggest that the benefit is mediated by paracrine factors [73]. A priori, a combination of autologous AT-ECs and AT-MSCs injected intramyocardially in patients with refractory angina should do better than any of the cells injected in studies published to date (Table 1), because the potential for direct contribution to neovascularization is considerably greater for these cells. To achieve this, however, the problem of the survival of cultured cells injected into myocardium needs to be solved.
Table 1.
Clinical trials of cell-based therapy in therapeutic angiogenesis for refractory angina
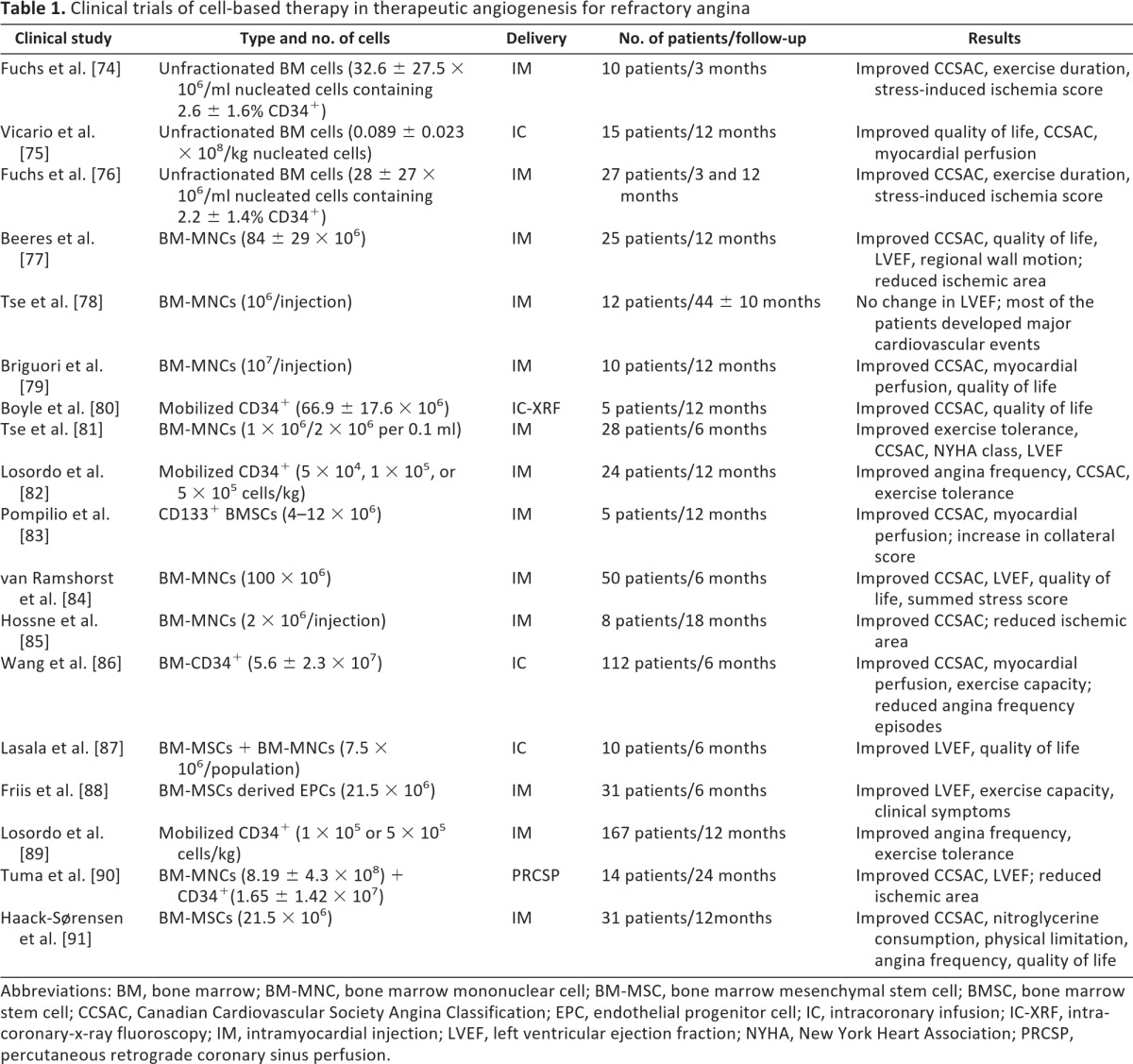
Abbreviations: BM, bone marrow; BM-MNC, bone marrow mononuclear cell; BM-MSC, bone marrow mesenchymal stem cell; BMSC, bone marrow stem cell; CCSAC, Canadian Cardiovascular Society Angina Classification; EPC, endothelial progenitor cell; IC, intracoronary infusion; IC-XRF, intra-coronary-x-ray fluoroscopy; IM, intramyocardial injection; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; PRCSP, percutaneous retrograde coronary sinus perfusion.
Also for critical limb ischemia that has not been amenable to dilatation procedures, a number of cell-based trials to establish neovascularization have been performed (Table 2). Again, the cells most commonly used have been BM-MNCs, and clinical improvement has also been recorded in these groups of patients. Naturally, direct proof of involvement of the injected cells in the establishment of new blood vessels is not available, but in several of these studies evidence of improved blood supply to the ischemic regions could be demonstrated. In a mouse model of hind limb ischemia, evidence supporting the survival and direct contribution to new blood vessel formation by injected human AT-MSCs has been published [35–37]. This would suggest that the likelihood of survival of injected angiogenic cells in limb tissues is better than in the myocardium. If so, injection of combinations of autologous AT-ECs and AT-MSCs is likely to give an even better clinical outcome than those reported in the studies cited in Table 2.
Table 2.
Clinical trials of cell-based therapy in therapeutic angiogenesis for critical limb/hand ischemia
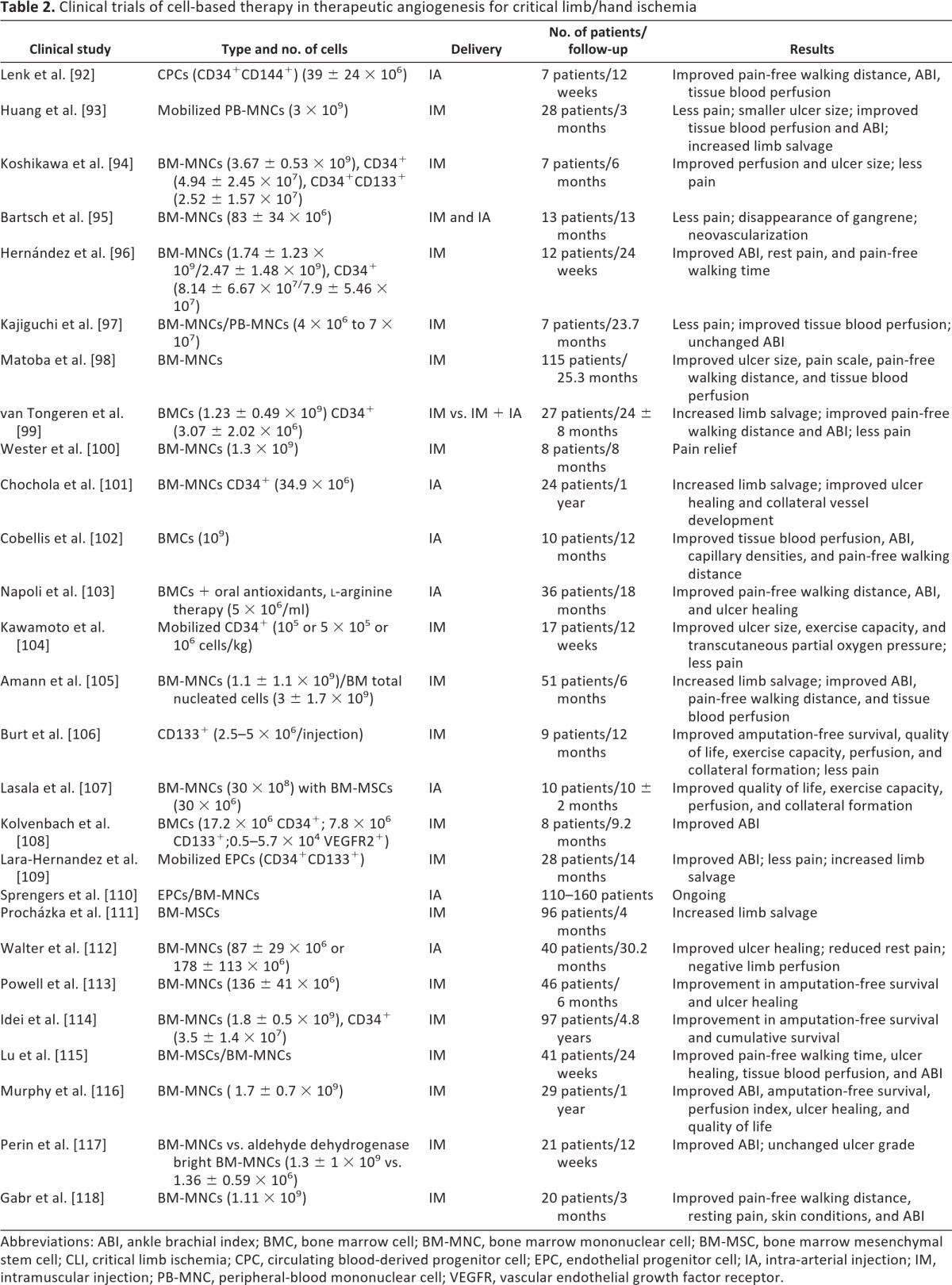
Abbreviations: ABI, ankle brachial index; BMC, bone marrow cell; BM-MNC, bone marrow mononuclear cell; BM-MSC, bone marrow mesenchymal stem cell; CLI, critical limb ischemia; CPC, circulating blood-derived progenitor cell; EPC, endothelial progenitor cell; IA, intra-arterial injection; IM, intramuscular injection; PB-MNC, peripheral-blood mononuclear cell; VEGFR, vascular endothelial growth factor receptor.
Conclusion
Traditional risk factors such as smoking, diabetes, hypercholesterolemia, hypertension, and age itself can lead to endothelial injury requiring repair of the vasculature. Surgical and catheter-based procedures are constantly improving the treatment options for many patients with tissue ischemia, but diseases mainly affecting arterioles and capillaries are likely to never be amenable to surgical or dilatation procedures. For these, cell-based therapeutic strategies will remain the best treatment options.
Two populations of cells with different functionalities exist in the SVF of AT that may contribute to neovascularization. Both may be used in the uncultured state, when the cell numbers will be lower but the cells are quickly available, and after in vitro expansion. Combinations of in vitro expanded AT-ECs and AT-MSCs yield robust vasculogenesis in Matrigel plugs injected into immunodeficient rodents, suggesting that these cells might also provide relief from ischemia in human clinical situations. However, several issues have to be addressed in order to get full therapeutic benefit from these cells. Most importantly, the cells must be seen to survive and directly contribute to new blood vessel formation. Another important issue is the mode of administration: should the cells be injected into the arterial tree supplying the ischemic area, or into the tissue actually exposed to ischemia? In addition, the role of supportive angiogenic cytokines and growth factors such as VEGF, FGF, HGF, and angiopoietin-1 remains unresolved. If one or more of these should be found to be beneficial, a decision has to be made whether the cytokines should be provided by supplemental injection or by genetically manipulating the injected cells.
The success of cell-based therapies depends on whether the engrafted cells differentiate into functional vascular cells and whether those cells can produce paracrine signals that encourage survival of the cells in the ischemic environment. Animal studies will be required to understand induced vasculogenesis in the suboptimal ischemic vascular environment and to ensure that treatment with angiogenic cells is safe. Issues such as nurturing the local environment and appropriate delivery methods are key issues that need to be resolved before successful regenerative therapies will be effective in patients.
Acknowledgments
This work was supported by research funding from the South-Eastern Norway Regional Health Authority.
Author Contributions
K.S.: conception and design, collection and/or assembly of data, manuscript writing; J.E.B.: conception and design, manuscript writing, financial support, final approval of manuscript.
Disclosure of Potential Conflicts of Interest
The authors indicate no potential conflicts of interest.
References
- 1.Weber C, Noels H. Atherosclerosis: Current pathogenesis and therapeutic options. Nat Med. 2011;17:1410–1422. doi: 10.1038/nm.2538. [DOI] [PubMed] [Google Scholar]
- 2.Nerem RM, Seliktar D. Vascular tissue engineering. Annu Rev Biomed Eng. 2001;3:225–243. doi: 10.1146/annurev.bioeng.3.1.225. [DOI] [PubMed] [Google Scholar]
- 3.Eltzschig HK, Eckle T. Ischemia and reperfusion—from mechanism to translation. Nat Med. 2011;17:1391–1401. doi: 10.1038/nm.2507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Collinson DJ, Donnelly R. Therapeutic angiogenesis in peripheral arterial disease: Can biotechnology produce an effective collateral circulation? Eur J Vasc Endovasc Surg. 2004;28:9–23. doi: 10.1016/j.ejvs.2004.03.021. [DOI] [PubMed] [Google Scholar]
- 5.Carmeliet P. Angiogenesis in health and disease. Nat Med. 2003;9:653–660. doi: 10.1038/nm0603-653. [DOI] [PubMed] [Google Scholar]
- 6.Freedman SB, Isner JM. Therapeutic angiogenesis for ischemic cardiovascular disease. J Mol Cell Cardiol. 2001;33:379–393. doi: 10.1006/jmcc.2000.1329. [DOI] [PubMed] [Google Scholar]
- 7.Pugh CW, Ratcliffe PJ. Regulation of angiogenesis by hypoxia: Role of the HIF system. Nat Med. 2003;9:677–684. doi: 10.1038/nm0603-677. [DOI] [PubMed] [Google Scholar]
- 8.Folkman J, D'Amore PA. Blood vessel formation: What is its molecular basis? Cell. 1996;87:1153–1155. doi: 10.1016/s0092-8674(00)81810-3. [DOI] [PubMed] [Google Scholar]
- 9.Drake CJ. Embryonic and adult vasculogenesis. Birth Defects Res C Embryo Today. 2003;69:73–82. doi: 10.1002/bdrc.10003. [DOI] [PubMed] [Google Scholar]
- 10.Eguchi M, Masuda H, Asahara T. Endothelial progenitor cells for postnatal vasculogenesis. Clin Exp Nephrol. 2007;11:18–25. doi: 10.1007/s10157-006-0448-1. [DOI] [PubMed] [Google Scholar]
- 11.Adamo L, Garcia-Cardena G. The vascular origin of hematopoietic cells. Dev Biol. 2012;362:1–10. doi: 10.1016/j.ydbio.2011.09.008. [DOI] [PubMed] [Google Scholar]
- 12.Asahara T, Masuda H, Takahashi T, et al. Bone marrow origin of endothelial progenitor cells responsible for postnatal vasculogenesis in physiological and pathological neovascularization. Circ Res. 1999;85:221–228. doi: 10.1161/01.res.85.3.221. [DOI] [PubMed] [Google Scholar]
- 13.Asahara T, Murohara T, Sullivan A, et al. Isolation of putative progenitor endothelial cells for angiogenesis. Science. 1997;275:964–967. doi: 10.1126/science.275.5302.964. [DOI] [PubMed] [Google Scholar]
- 14.Fadini GP, Losordo D, Dimmeler S. Critical reevaluation of endothelial progenitor cell phenotypes for therapeutic and diagnostic use. Circ Res. 2012;110:624–637. doi: 10.1161/CIRCRESAHA.111.243386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rafii S, Lyden D. Therapeutic stem and progenitor cell transplantation for organ vascularization and regeneration. Nat Med. 2003;9:702–712. doi: 10.1038/nm0603-702. [DOI] [PubMed] [Google Scholar]
- 16.Kalka C, Masuda H, Takahashi T, et al. Transplantation of ex vivo expanded endothelial progenitor cells for therapeutic neovascularization. Proc Natl Acad Sci USA. 2000;97:3422–3427. doi: 10.1073/pnas.070046397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Takahashi T, Kalka C, Masuda H, et al. Ischemia- and cytokine-induced mobilization of bone marrow-derived endothelial progenitor cells for neovascularization. Nat Med. 1999;5:434–438. doi: 10.1038/7434. [DOI] [PubMed] [Google Scholar]
- 18.Prater DN, Case J, Ingram DA, et al. Working hypothesis to redefine endothelial progenitor cells. Leukemia. 2007;21:1141–1149. doi: 10.1038/sj.leu.2404676. [DOI] [PubMed] [Google Scholar]
- 19.Hur J, Yoon CH, Kim HS, et al. Characterization of two types of endothelial progenitor cells and their different contributions to neovasculogenesis. Arterioscler Thromb Vasc Biol. 2004;24:288–293. doi: 10.1161/01.ATV.0000114236.77009.06. [DOI] [PubMed] [Google Scholar]
- 20.Reinisch A, Hofmann NA, Obenauf AC, et al. Humanized large-scale expanded endothelial colony-forming cells function in vitro and in vivo. Blood. 2009;113:6716–6725. doi: 10.1182/blood-2008-09-181362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lindroos B, Suuronen R, Miettinen S. The potential of adipose stem cells in regenerative medicine. Stem Cell Rev. 2011;7:269–291. doi: 10.1007/s12015-010-9193-7. [DOI] [PubMed] [Google Scholar]
- 22.Crisan M, Yap S, Casteilla L, et al. A perivascular origin for mesenchymal stem cells in multiple human organs. Cell Stem Cell. 2008;3:301–313. doi: 10.1016/j.stem.2008.07.003. [DOI] [PubMed] [Google Scholar]
- 23.Traktuev DO, Merfeld-Clauss S, Li J, et al. A population of multipotent CD34-positive adipose stromal cells share pericyte and mesenchymal surface markers, reside in a periendothelial location, and stabilize endothelial networks. Circ Res. 2008;102:77–85. doi: 10.1161/CIRCRESAHA.107.159475. [DOI] [PubMed] [Google Scholar]
- 24.Cao Y. Angiogenesis modulates adipogenesis and obesity. J Clin Invest. 2007;117:2362–2368. doi: 10.1172/JCI32239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zuk PA, Zhu M, Mizuno H, et al. Multilineage cells from human adipose tissue: Implications for cell-based therapies. Tissue Eng. 2001;7:211–228. doi: 10.1089/107632701300062859. [DOI] [PubMed] [Google Scholar]
- 26.Zuk PA, Zhu M, Ashjian P, et al. Human adipose tissue is a source of multipotent stem cells. Mol Biol Cell. 2002;13:4279–4295. doi: 10.1091/mbc.E02-02-0105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Boquest AC, Shahdadfar A, Fronsdal K, et al. Isolation and transcription profiling of purified uncultured human stromal stem cells: Alteration of gene expression after in vitro cell culture. Mol Biol Cell. 2005;16:1131–1141. doi: 10.1091/mbc.E04-10-0949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8:315–317. doi: 10.1080/14653240600855905. [DOI] [PubMed] [Google Scholar]
- 29.Szöke K, Beckstrom KJ, Brinchmann JE. Human adipose tissue as a source of cells with angiogenic potential. Cell Transplant. 2012;21:235–250. doi: 10.3727/096368911X580518. [DOI] [PubMed] [Google Scholar]
- 30.Fraser JK, Wulur I, Alfonso Z, et al. Fat tissue: An underappreciated source of stem cells for biotechnology. Trends Biotechnol. 2006;24:150–154. doi: 10.1016/j.tibtech.2006.01.010. [DOI] [PubMed] [Google Scholar]
- 31.Ouma GO, Jonas RA, Usman MH, et al. Targets and delivery methods for therapeutic angiogenesis in peripheral artery disease. Vasc Med. 2012;17:174–192. doi: 10.1177/1358863X12438270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rehman J, Traktuev D, Li J, et al. Secretion of angiogenic and antiapoptotic factors by human adipose stromal cells. Circulation. 2004;109:1292–1298. doi: 10.1161/01.CIR.0000121425.42966.F1. [DOI] [PubMed] [Google Scholar]
- 33.Nakagami H, Maeda K, Morishita R, et al. Novel autologous cell therapy in ischemic limb disease through growth factor secretion by cultured adipose tissue-derived stromal cells. Arterioscler Thromb Vasc Biol. 2005;25:2542–2547. doi: 10.1161/01.ATV.0000190701.92007.6d. [DOI] [PubMed] [Google Scholar]
- 34.Reichenberger MA, Heimer S, Schaefer A, et al. Adipose derived stem cells protect skin flaps against ischemia-reperfusion injury. Stem Cell Rev. 2012;8:854–862. doi: 10.1007/s12015-012-9368-5. [DOI] [PubMed] [Google Scholar]
- 35.Miranville A, Heeschen C, Sengenes C, et al. Improvement of postnatal neovascularization by human adipose tissue-derived stem cells. Circulation. 2004;110:349–355. doi: 10.1161/01.CIR.0000135466.16823.D0. [DOI] [PubMed] [Google Scholar]
- 36.Planat-Benard V, Silvestre JS, Cousin B, et al. Plasticity of human adipose lineage cells toward endothelial cells: Physiological and therapeutic perspectives. Circulation. 2004;109:656–663. doi: 10.1161/01.CIR.0000114522.38265.61. [DOI] [PubMed] [Google Scholar]
- 37.Moon MH, Kim SY, Kim YJ, et al. Human adipose tissue-derived mesenchymal stem cells improve postnatal neovascularization in a mouse model of hindlimb ischemia. Cell Physiol Biochem. 2006;17:279–290. doi: 10.1159/000094140. [DOI] [PubMed] [Google Scholar]
- 38.Kondo K, Shintani S, Shibata R, et al. Implantation of adipose-derived regenerative cells enhances ischemia-induced angiogenesis. Arterioscler Thromb Vasc Biol. 2009;29:61–66. doi: 10.1161/ATVBAHA.108.166496. [DOI] [PubMed] [Google Scholar]
- 39.Covas DT, Panepucci RA, Fontes AM, et al. Multipotent mesenchymal stromal cells obtained from diverse human tissues share functional properties and gene-expression profile with CD146+ perivascular cells and fibroblasts. Exp Hematol. 2008;36:642–654. doi: 10.1016/j.exphem.2007.12.015. [DOI] [PubMed] [Google Scholar]
- 40.da Silva ML, Caplan AI, Nardi NB. In search of the in vivo identity of mesenchymal stem cells. Stem Cells. 2008;26:2287–2299. doi: 10.1634/stemcells.2007-1122. [DOI] [PubMed] [Google Scholar]
- 41.Caplan AI. All MSCs are pericytes? Cell Stem Cell. 2008;3:229–230. doi: 10.1016/j.stem.2008.08.008. [DOI] [PubMed] [Google Scholar]
- 42.Corselli M, Chen CW, Crisan M, et al. Perivascular ancestors of adult multipotent stem cells. Arterioscler Thromb Vasc Biol. 2010;30:1104–1109. doi: 10.1161/ATVBAHA.109.191643. [DOI] [PubMed] [Google Scholar]
- 43.von Tell D, Armulik A, Betsholtz C. Pericytes and vascular stability. Exp Cell Res. 2006;312:623–629. doi: 10.1016/j.yexcr.2005.10.019. [DOI] [PubMed] [Google Scholar]
- 44.Arts CH, de GP, Heijnen-Snyder GJ, et al. Application of a clinical grade CD34-mediated method for the enrichment of microvascular endothelial cells from fat tissue. Cytotherapy. 2004;6:30–42. doi: 10.1080/14653240310004476. [DOI] [PubMed] [Google Scholar]
- 45.Hewett PW. Vascular endothelial cells from human micro- and macrovessels: Isolation, characterisation and culture. Methods Mol Biol. 2009;467:95–111. doi: 10.1007/978-1-59745-241-0_5. [DOI] [PubMed] [Google Scholar]
- 46.Kern PA, Knedler A, Eckel RH. Isolation and culture of microvascular endothelium from human adipose tissue. J Clin Invest. 1983;71:1822–1829. doi: 10.1172/JCI110937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Koyama M, Satoh K, Yoshida H, et al. Surface coverage of vascular grafts with cultured human endothelial cells from subcutaneous fat tissue obtained with a biopsy needle. Thromb Haemost. 1996;76:610–614. [PubMed] [Google Scholar]
- 48.Sharp WV, Schmidt SP, Meerbaum SO, et al. Derivation of human microvascular endothelial cells for prosthetic vascular graft seeding. Ann Vasc Surg. 1989;3:104–107. doi: 10.1016/S0890-5096(06)62001-3. [DOI] [PubMed] [Google Scholar]
- 49.Hristov M, Weber C. Endothelial progenitor cells: Characterization, pathophysiology, and possible clinical relevance. J Cell Mol Med. 2004;8:498–508. doi: 10.1111/j.1582-4934.2004.tb00474.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Urbich C, Dimmeler S. Endothelial progenitor cells functional characterization. Trends Cardiovasc Med. 2004;14:318–322. doi: 10.1016/j.tcm.2004.10.001. [DOI] [PubMed] [Google Scholar]
- 51.Bagley RG, Walter-Yohrling J, Cao X, et al. Endothelial precursor cells as a model of tumor endothelium: Characterization and comparison with mature endothelial cells. Cancer Res. 2003;63:5866–5873. [PubMed] [Google Scholar]
- 52.Casteilla L, Planat-Benard V, Laharrague P, et al. Adipose-derived stromal cells: Their identity and uses in clinical trials, an update. World J Stem Cells. 2011;3:25–33. doi: 10.4252/wjsc.v3.i4.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hicok KC, Hedrick MH. Automated isolation and processing of adipose-derived stem and regenerative cells. Methods Mol Biol. 2011;702:87–105. doi: 10.1007/978-1-61737-960-4_8. [DOI] [PubMed] [Google Scholar]
- 54.Doi K, Tanaka S, Iida H, et al. Stromal vascular fraction isolated from lipo-aspirates using an automated processing system: Bench and bed analysis. J Tissue Eng Regen Med. 2012 doi: 10.1002/term.1478. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 55.Güven S, Karagianni M, Schwalbe M, et al. Validation of an automated procedure to isolate human adipose tissue-derived cells by using the Sepax(®) technology. Tissue Eng Part C Methods. 2012;18:575–582. doi: 10.1089/ten.tec.2011.0617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Alexander I, Edelman ER, Methe H. Function and mode of regulation of endothelial major histocompatibility complex class II. Cell Transplant. 2009;18:255–259. doi: 10.3727/096368909788534997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Prunet-Marcassus B, Cousin B, Caton D, et al. From heterogeneity to plasticity in adipose tissues: Site-specific differences. Exp Cell Res. 2006;312:727–736. doi: 10.1016/j.yexcr.2005.11.021. [DOI] [PubMed] [Google Scholar]
- 58.Puissant B, Barreau C, Bourin P, et al. Immunomodulatory effect of human adipose tissue-derived adult stem cells: Comparison with bone marrow mesenchymal stem cells. Br J Haematol. 2005;129:118–129. doi: 10.1111/j.1365-2141.2005.05409.x. [DOI] [PubMed] [Google Scholar]
- 59.Yanez R, Lamana ML, Garcia-Castro J, et al. Adipose tissue-derived mesenchymal stem cells have in vivo immunosuppressive properties applicable for the control of the graft-versus-host disease. Stem Cells. 2006;24:2582–2591. doi: 10.1634/stemcells.2006-0228. [DOI] [PubMed] [Google Scholar]
- 60.Kucerova L, Altanerova V, Matuskova M, et al. Adipose tissue-derived human mesenchymal stem cells mediated prodrug cancer gene therapy. Cancer Res. 2007;67:6304–6313. doi: 10.1158/0008-5472.CAN-06-4024. [DOI] [PubMed] [Google Scholar]
- 61.Yu JM, Jun ES, Bae YC, et al. Mesenchymal stem cells derived from human adipose tissues favor tumor cell growth in vivo. Stem Cells Dev. 2008;17:463–473. doi: 10.1089/scd.2007.0181. [DOI] [PubMed] [Google Scholar]
- 62.Muehlberg FL, Song YH, Krohn A, et al. Tissue-resident stem cells promote breast cancer growth and metastasis. Carcinogenesis. 2009;30:589–597. doi: 10.1093/carcin/bgp036. [DOI] [PubMed] [Google Scholar]
- 63.Cousin B, Ravet E, Poglio S, et al. Adult stromal cells derived from human adipose tissue provoke pancreatic cancer cell death both in vitro and in vivo. PLoS One. 2009;4:e6278. doi: 10.1371/journal.pone.0006278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Casiraghi F, Remuzzi G, Abbate M, et al. Multipotent mesenchymal stromal cell therapy and risk of malignancies. Stem Cell Rev. 2012 doi: 10.1007/s12015-011-9345-4. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 65.von Bahr L, Batsis I, Moll G, et al. Analysis of tissues following mesenchymal stromal cell therapy in humans indicates limited long-term engraftment and no ectopic tissue formation. Stem Cells. 2012;30:1575–1578. doi: 10.1002/stem.1118. [DOI] [PubMed] [Google Scholar]
- 66.Lee JS, Hong JM, Moon GJ, et al. A long-term follow-up study of intravenous autologous mesenchymal stem cell transplantation in patients with ischemic stroke. Stem Cells. 2010;28:1099–1106. doi: 10.1002/stem.430. [DOI] [PubMed] [Google Scholar]
- 67.Kaneko Y, Tajiri N, Shinozuka K, et al. Cell therapy for stroke: Emphasis on optimizing safety and efficacy profile of endothelial progenitor cells. Curr Pharm Des. 2012;18:3731–3734. doi: 10.2174/138161212802002733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Peck M, Gebhart D, Dusserre N, et al. The evolution of vascular tissue engineering and current state of the art. Cells Tissues Organs. 2012;195:144–158. doi: 10.1159/000331406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Clifford DM, Fisher SA, Brunskill SJ, et al. Stem cell treatment for acute myocardial infarction. Cochrane Database Syst Rev. 2012;2:CD006536. doi: 10.1002/14651858.CD006536.pub3. [DOI] [PubMed] [Google Scholar]
- 70.Beitnes JO, Lunde K, Brinchmann JE, et al. Stem cells for cardiac repair in acute myocardial infarction. Expert Rev Cardiovasc Ther. 2011;9:1015–1025. doi: 10.1586/erc.11.108. [DOI] [PubMed] [Google Scholar]
- 71.Robich MP, Chu LM, Oyamada S, et al. Myocardial therapeutic angiogenesis: A review of the state of development and future obstacles. Expert Rev Cardiovasc Ther. 2011;9:1469–1479. doi: 10.1586/erc.11.148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Beitnes JO, Oie E, Shahdadfar A, et al. Intramyocardial injections of human mesenchymal stem cells following acute myocardial infarction modulate scar formation and improve left ventricular function. Cell Transplant. 2012 doi: 10.3727/096368911X627462. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 73.Wollert KC, Drexler H. Cell therapy for the treatment of coronary heart disease: A critical appraisal. Nat Rev Cardiol. 2010;7:204–215. doi: 10.1038/nrcardio.2010.1. [DOI] [PubMed] [Google Scholar]
- 74.Fuchs S, Satler LF, Kornowski R, et al. Catheter-based autologous bone marrow myocardial injection in no-option patients with advanced coronary artery disease: A feasibility study. J Am Coll Cardiol. 2003;41:1721–1724. doi: 10.1016/s0735-1097(03)00328-0. [DOI] [PubMed] [Google Scholar]
- 75.Vicario J, Campo C, Piva J, et al. One-year follow-up of transcoronary sinus administration of autologous bone marrow in patients with chronic refractory angina. Cardiovasc Revasc Med. 2005;6:99–107. doi: 10.1016/j.carrev.2005.08.002. [DOI] [PubMed] [Google Scholar]
- 76.Fuchs S, Kornowski R, Weisz G, et al. Safety and feasibility of transendocardial autologous bone marrow cell transplantation in patients with advanced heart disease. Am J Cardiol. 2006;97:823–829. doi: 10.1016/j.amjcard.2005.09.132. [DOI] [PubMed] [Google Scholar]
- 77.Beeres SL, Bax JJ, Dibbets-Schneider P, et al. Sustained effect of autologous bone marrow mononuclear cell injection in patients with refractory angina pectoris and chronic myocardial ischemia: Twelve-month follow-up results. Am Heart J. 2006;152:684.e11–684.e16. doi: 10.1016/j.ahj.2006.07.018. [DOI] [PubMed] [Google Scholar]
- 78.Tse HF, Thambar S, Kwong YL, et al. Safety of catheter-based intramyocardial autologous bone marrow cells implantation for therapeutic angiogenesis. Am J Cardiol. 2006;98:60–62. doi: 10.1016/j.amjcard.2006.01.056. [DOI] [PubMed] [Google Scholar]
- 79.Briguori C, Reimers B, Sarais C, et al. Direct intramyocardial percutaneous delivery of autologous bone marrow in patients with refractory myocardial angina. Am Heart J. 2006;151:674–680. doi: 10.1016/j.ahj.2005.04.033. [DOI] [PubMed] [Google Scholar]
- 80.Boyle AJ, Whitbourn R, Schlicht S, et al. Intra-coronary high-dose CD34+ stem cells in patients with chronic ischemic heart disease: A 12-month follow-up. Int J Cardiol. 2006;109:21–27. doi: 10.1016/j.ijcard.2005.05.024. [DOI] [PubMed] [Google Scholar]
- 81.Tse HF, Thambar S, Kwong YL, et al. Prospective randomized trial of direct endomyocardial implantation of bone marrow cells for treatment of severe coronary artery diseases (PROTECT-CAD trial) Eur Heart J. 2007;28:2998–3005. doi: 10.1093/eurheartj/ehm485. [DOI] [PubMed] [Google Scholar]
- 82.Losordo DW, Schatz RA, White CJ, et al. Intramyocardial transplantation of autologous CD34+ stem cells for intractable angina: A phase I/IIa double-blind, randomized controlled trial. Circulation. 2007;115:3165–3172. doi: 10.1161/CIRCULATIONAHA.106.687376. [DOI] [PubMed] [Google Scholar]
- 83.Pompilio G, Steinhoff G, Liebold A, et al. Direct minimally invasive intramyocardial injection of bone marrow-derived AC133+ stem cells in patients with refractory ischemia: Preliminary results. Thorac Cardiovasc Surg. 2008;56:71–76. doi: 10.1055/s-2007-989351. [DOI] [PubMed] [Google Scholar]
- 84.van Ramshorst J, Bax JJ, Beeres SL, et al. Intramyocardial bone marrow cell injection for chronic myocardial ischemia: A randomized controlled trial. JAMA. 2009;301:1997–2004. doi: 10.1001/jama.2009.685. [DOI] [PubMed] [Google Scholar]
- 85.Hossne NA, Jr., Invitti AL, Buffolo E, et al. Refractory angina cell therapy (ReACT) involving autologous bone marrow cells in patients without left ventricular dysfunction: A possible role for monocytes. Cell Transplant. 2009;18:1299–1310. doi: 10.3727/096368909X484671. [DOI] [PubMed] [Google Scholar]
- 86.Wang S, Cui J, Peng W, et al. Intracoronary autologous CD34+ stem cell therapy for intractable angina. Cardiology. 2010;117:140–147. doi: 10.1159/000320217. [DOI] [PubMed] [Google Scholar]
- 87.Lasala GP, Silva JA, Kusnick BA, et al. Combination stem cell therapy for the treatment of medically refractory coronary ischemia: A Phase I study. Cardiovasc Revasc Med. 2011;12:29–34. doi: 10.1016/j.carrev.2010.01.001. [DOI] [PubMed] [Google Scholar]
- 88.Friis T, Haack-Sørensen M, Mathiasen AB, et al. Mesenchymal stromal cell derived endothelial progenitor treatment in patients with refractory angina. Scand Cardiovasc J. 2011;45:161–168. doi: 10.3109/14017431.2011.569571. [DOI] [PubMed] [Google Scholar]
- 89.Losordo DW, Henry TD, Davidson C, et al. Intramyocardial, autologous CD34+ cell therapy for refractory angina. Circ Res. 2011;109:428–436. doi: 10.1161/CIRCRESAHA.111.245993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Tuma J, Fernandez-Vina R, Carrasco A, et al. Safety and feasibility of percutaneous retrograde coronary sinus delivery of autologous bone marrow mononuclear cell transplantation in patients with chronic refractory angina. J Transl Med. 2011;9:183. doi: 10.1186/1479-5876-9-183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Haack-Sørensen M, Friis T, Mathiasen AB, et al. Direct intramyocardial mesenchymal stromal cell injections in patients with severe refractory angina: One year follow-up. Cell Transplant. 2012 doi: 10.3727/096368912X636830. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 92.Lenk K, Adams V, Lurz P, et al. Therapeutical potential of blood-derived progenitor cells in patients with peripheral arterial occlusive disease and critical limb ischaemia. Eur Heart J. 2005;26:1903–1909. doi: 10.1093/eurheartj/ehi285. [DOI] [PubMed] [Google Scholar]
- 93.Huang P, Li S, Han M, et al. Autologous transplantation of granulocyte colony-stimulating factor-mobilized peripheral blood mononuclear cells improves critical limb ischemia in diabetes. Diabetes Care. 2005;28:2155–2160. doi: 10.2337/diacare.28.9.2155. [DOI] [PubMed] [Google Scholar]
- 94.Koshikawa M, Shimodaira S, Yoshioka T, et al. Therapeutic angiogenesis by bone marrow implantation for critical hand ischemia in patients with peripheral arterial disease: A pilot study. Curr Med Res Opin. 2006;22:793–798. doi: 10.1185/030079906X1000078. [DOI] [PubMed] [Google Scholar]
- 95.Bartsch T, Brehm M, Zeus T, et al. Transplantation of autologous mononuclear bone marrow stem cells in patients with peripheral arterial disease (the TAM-PAD study) Clin Res Cardiol. 2007;96:891–899. doi: 10.1007/s00392-007-0569-x. [DOI] [PubMed] [Google Scholar]
- 96.Hernández P, Cortina L, Artaza H, et al. Autologous bone-marrow mononuclear cell implantation in patients with severe lower limb ischaemia: A comparison of using blood cell separator and Ficoll density gradient centrifugation. Atherosclerosis. 2007;194:e52–e56. doi: 10.1016/j.atherosclerosis.2006.08.025. [DOI] [PubMed] [Google Scholar]
- 97.Kajiguchi M, Kondo T, Izawa H, et al. Safety and efficacy of autologous progenitor cell transplantation for therapeutic angiogenesis in patients with critical limb ischemia. Circ J. 2007;71:196–201. doi: 10.1253/circj.71.196. [DOI] [PubMed] [Google Scholar]
- 98.Matoba S, Tatsumi T, Murohara T, et al. Long-term clinical outcome after intramuscular implantation of bone marrow mononuclear cells (Therapeutic Angiogenesis by Cell Transplantation [TACT] trial) in patients with chronic limb ischemia. Am Heart J. 2008;156:1010–1018. doi: 10.1016/j.ahj.2008.06.025. [DOI] [PubMed] [Google Scholar]
- 99.Van Tongeren RB, Hamming JF, Fibbe WE, et al. Intramuscular or combined intramuscular/intra-arterial administration of bone marrow mononuclear cells: A clinical trial in patients with advanced limb ischemia. J Cardiovasc Surg (Torino) 2008;49:51–58. [PubMed] [Google Scholar]
- 100.Wester T, Jorgensen JJ, Stranden E, et al. Treatment with autologous bone marrow mononuclear cells in patients with critical lower limb ischaemia. A pilot study. Scand J Surg. 2008;97:56–62. doi: 10.1177/145749690809700108. [DOI] [PubMed] [Google Scholar]
- 101.Chochola M, Pytlik R, Kobylka P, et al. Autologous intra-arterial infusion of bone marrow mononuclear cells in patients with critical leg ischemia. Int Angiol. 2008;27:281–290. [PubMed] [Google Scholar]
- 102.Cobellis G, Silvestroni A, Lillo S, et al. Long-term effects of repeated autologous transplantation of bone marrow cells in patients affected by peripheral arterial disease. Bone Marrow Transplant. 2008;42:667–672. doi: 10.1038/bmt.2008.228. [DOI] [PubMed] [Google Scholar]
- 103.Napoli C, Farzati B, Sica V, et al. Beneficial effects of autologous bone marrow cell infusion and antioxidants/l-arginine in patients with chronic critical limb ischemia. Eur J Cardiovasc Prev Rehabil. 2008;15:709–718. doi: 10.1097/HJR.0b013e3283193a0f. [DOI] [PubMed] [Google Scholar]
- 104.Kawamoto A, Katayama M, Handa N, et al. Intramuscular transplantation of G-CSF-mobilized CD34(+) cells in patients with critical limb ischemia: A phase I/IIa, multicenter, single-blinded, dose-escalation clinical trial. Stem Cells. 2009;27:2857–2864. doi: 10.1002/stem.207. [DOI] [PubMed] [Google Scholar]
- 105.Amann B, Luedemann C, Ratei R, et al. Autologous bone marrow cell transplantation increases leg perfusion and reduces amputations in patients with advanced critical limb ischemia due to peripheral artery disease. Cell Transplant. 2009;18:371–380. doi: 10.3727/096368909788534942. [DOI] [PubMed] [Google Scholar]
- 106.Burt RK, Testori A, Oyama Y, et al. Autologous peripheral blood CD133+ cell implantation for limb salvage in patients with critical limb ischemia. Bone Marrow Transplant. 2010;45:111–116. doi: 10.1038/bmt.2009.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Lasala GP, Silva JA, Gardner PA, et al. Combination stem cell therapy for the treatment of severe limb ischemia: Safety and efficacy analysis. Angiology. 2010;61:551–556. doi: 10.1177/0003319710364213. [DOI] [PubMed] [Google Scholar]
- 108.Kolvenbach R, Kreissig C, Cagiannos C, et al. Intraoperative adjunctive stem cell treatment in patients with critical limb ischemia using a novel point-of-care device. Ann Vasc Surg. 2010;24:367–372. doi: 10.1016/j.avsg.2009.07.018. [DOI] [PubMed] [Google Scholar]
- 109.Lara-Hernandez R, Lozano-Vilardell P, Blanes P, et al. Safety and efficacy of therapeutic angiogenesis as a novel treatment in patients with critical limb ischemia. Ann Vasc Surg. 2010;24:287–294. doi: 10.1016/j.avsg.2009.10.012. [DOI] [PubMed] [Google Scholar]
- 110.Sprengers RW, Moll FL, Teraa M, et al. Rationale and design of the JUVENTAS trial for repeated intra-arterial infusion of autologous bone marrow-derived mononuclear cells in patients with critical limb ischemia. J Vasc Surg. 2010;51:1564–1568. doi: 10.1016/j.jvs.2010.02.020. [DOI] [PubMed] [Google Scholar]
- 111.Procházka V, Gumulec J, Jaluvka F, et al. Cell therapy, a new standard in management of chronic critical limb ischemia and foot ulcer. Cell Transplant. 2010;19:1413–1424. doi: 10.3727/096368910X514170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Walter DH, Krankenberg H, Balzer JO, et al. Intraarterial administration of bone marrow mononuclear cells in patients with critical limb ischemia: A randomized-start, placebo-controlled pilot trial (PROVASA) Circ Cardiovasc Interv. 2011;4:26–37. doi: 10.1161/CIRCINTERVENTIONS.110.958348. [DOI] [PubMed] [Google Scholar]
- 113.Powell RJ, Comerota AJ, Berceli SA, et al. Interim analysis results from the RESTORE-CLI, a randomized, double-blind multicenter phase II trial comparing expanded autologous bone marrow-derived tissue repair cells and placebo in patients with critical limb ischemia. J Vasc Surg. 2011;54:1032–1041. doi: 10.1016/j.jvs.2011.04.006. [DOI] [PubMed] [Google Scholar]
- 114.Idei N, Soga J, Hata T, et al. Autologous bone-marrow mononuclear cell implantation reduces long-term major amputation risk in patients with critical limb ischemia: A comparison of atherosclerotic peripheral arterial disease and Buerger disease. Circ Cardiovasc Interv. 2011;4:15–25. doi: 10.1161/CIRCINTERVENTIONS.110.955724. [DOI] [PubMed] [Google Scholar]
- 115.Lu D, Chen B, Liang Z, et al. Comparison of bone marrow mesenchymal stem cells with bone marrow-derived mononuclear cells for treatment of diabetic critical limb ischemia and foot ulcer: A double-blind, randomized, controlled trial. Diabetes Res Clin Pract. 2011;92:26–36. doi: 10.1016/j.diabres.2010.12.010. [DOI] [PubMed] [Google Scholar]
- 116.Murphy MP, Lawson JH, Rapp BM, et al. Autologous bone marrow mononuclear cell therapy is safe and promotes amputation-free survival in patients with critical limb ischemia. J Vasc Surg. 2011;53:1565–1574. doi: 10.1016/j.jvs.2011.01.074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Perin EC, Silva G, Gahremanpour A, et al. A randomized, controlled study of autologous therapy with bone marrow-derived aldehyde dehydrogenase bright cells in patients with critical limb ischemia. Catheter Cardiovasc Interv. 2011;78:1060–1067. doi: 10.1002/ccd.23066. [DOI] [PubMed] [Google Scholar]
- 118.Gabr H, Hedayet A, Imam U, et al. Limb salvage using intramuscular injection of unfractionated autologous bone marrow mononuclear cells in critical limb ischemia: A prospective pilot clinical trial. Exp Clin Transplant. 2011;9:197–202. [PubMed] [Google Scholar]