

Abstract
Objectives:
The present comparative analysis aimed at evaluating the mechanical behavior of various restorative materials in abfraction lesion in the presence and absence of occlusal restoration.
Materials and Methods:
A three-dimensional finite-element analysis was performed. Six experimental models of mandibular first premolar were generated and divided into two groups (groups A and B) of three each. All the groups had cervical abfraction lesion restored with materials and in addition group A had class I occlusal restoration. A load of 90 N, 200 N, and 400 N were applied at 45° loading angle on the buccal inclines of buccal cusp and Von Mises stresses was chosen for analysis.
Results:
In all the models, the values of stress recorded at the cervical margin of the restorations were at their maxima. Irrespective of the occlusal restoration, all the materials performed well at 90 N and 200 N. At 400 N, only low-shrink composite showed stresses lesser than its tensile strength indicating its success even at higher load.
Conclusion:
Irrespective of occlusal restoration, restorative materials with low modulus of elasticity are successful in abfraction lesions at moderate tensile stresses; whereas materials with higher modulus of elasticity and mechanical properties can support higher loads and resist wear.
Significance:
The model allows comparison of different restorative materials for restoration of abfraction lesions in the presence and absence of occlusal restoration. The model can be used to validate more sophisticated computational models as well as to conduct various optimization studies.
Keywords: Abfraction lesion, finite-element analysis, low-shrink composite, nano-filled restorative materials, resin-modified glass-ionomer, stress distribution
INTRODUCTION
Abfraction lesions present primarily at the cervical region of the dentition and are typically wedge-shaped, with a sharp internal and external line angles.[1,2] Studies have shown that it is multi-factorial in etiology. Recently, the finite-element analysis (FEA) has been extensively used in dentistry because it shows the tooth mechanical behavior in detail. This method is extremely useful for indicating mechanical aspects of biomaterials and human tissues that can hardly be measured in-vivo.[3]
Currently, materials indicated to be used for restoring the cervical lesions include: Glass-ionomer cements (GIC), resin-modified glass-ionomer cements (RMGIC), poly-acid modified resin-based composites (compomers) and composite resins.[4] Stress concentration at the cervical region is responsible not only for the development of cervical lesion but for restoration retention failure as well. Combining chemical adhesion and restorative materials of appropriate elastic properties show promise of long-term success.[5]
In this study, nano-filled RMGIC, micro-hybrid low-shrink resin composites were evaluated. Tyas,[6] recommended that RMGIC should be the first preference for restoration of non-carious cervical lesions (NCCLs) and RMGIC/GIC liner base be laminated with resin composite; hence, layering technique was also considered. So, the purpose of this study was two fold.First, to evaluate the mechanical behavior of various restorative materials in abfraction lesion and secondly, stresses generated in the tooth and cervical restoration in the presence and absence of occlusal restoration.
MATERIALS AND METHODS
A three-dimensional (3D) finite-element model (FEM) of a mandibular first premolar was created in the FEA software preprocessor ANSYS rel 9.0 FEM software (ANSYS Inc., Houston, USA). As judged by direct vision and radiography the reconstruction was done with comparison of literature data[7] on tooth morphology. According to Coolidge,[8] the periodontal ligament is of varying thickness in-vivo and has been applied in this study to make the model more precise and realistic. The alveolar bone (cancellous and compact) that supports the tooth was reconstructed with the upper line of the bone 3 mm below the cervical line of the tooth simulating an actual anatomic situation.
First order tetrahedral elements with 3 degree of freedom per node were used for meshing the models which resulted in 67,278 nodes and 357,333 elements of approximately 0.3 mm size. The exterior nodes of the alveolar bone were fixed in all directions as the boundary conditions. Modulus of elasticity and Poisson's ratio were assigned to the elements [Table 1].
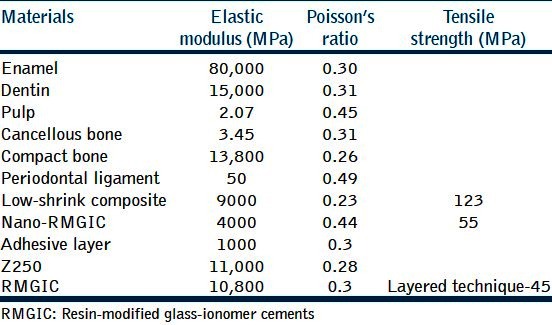
Table 1.
Material properties
Six experimental models were generated and an abfraction wedge shaped lesion was created on the buccal cervical margin of 1.5 mm deep and 2 mm in occluso-cervical direction. The angle of the wedge-shaped defect was 45° [Figure 1a]. Models were divided into groups A and B (n = 3). Group A models had an additional class-I shaped volume with cavity depth of 2 mm and was given the properties of micro-hybrid composite (Filtek Z250, 3M ESPE Seefeld, Germany). The adhesive layer was modeled in the cervical lesion and the occlusal cavity (group A) for composite resin restorations as a shell layer of 50 μm wide.
Figure 1.
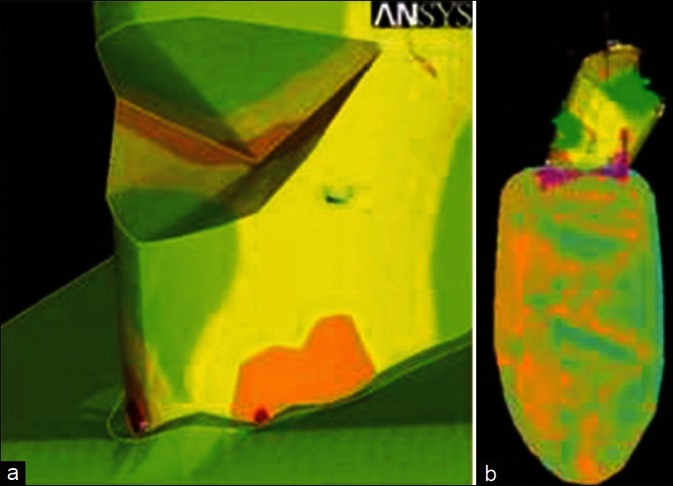
Finite element model of tooth, (a) Details of abfraction lesion, (b) Direction and location of applied force on tooth
All the models were grouped and sub-grouped as follows:
Group A: Model with abfraction lesion and occlusal restoration
Group B: Model with abfraction lesion and without occlusal restoration
A1 and B1: Low shrink composite (Filtek LS, 3M ESPE, Seefeld, Germany)
A2 and B2: Nano-RMGIC (Ketac N100, 3M ESPE, Seefeld, Germany)
A3 and B3: A layered technique with use of conventional resin-modified glass-ionomer cement (Fuji II LC, GC, Tokyo, Japan) of 0.5 mm thickness veneered by 1 mm thickness of low shrink composite.
Polymerization shrinkage was modeled in the materials using uniform volumetric contraction. Polymerization contraction of micro-hybrid composite in the occlusal cavity was modeled as 2% (group A) and low shrink composite in the abfraction lesion was modeled as 1%.
A load of 90 N, 200 N, and 400 N were applied on the buccal inclines of the buccal cusp and oriented in 45° oblique direction toward the buccal from the long axis of the tooth [Figure 1b]. This yielded three distinctive loading cases for each of the material under each group. Only static loading was considered and the occlusal load of typical magnitude was resolved into vertical (y-axis) and horizontal (x-axis) components and applied on the tooth [Figure 1b]. The failure was decided by the fact that a higher Von Mises stress value will be an indication of a greater possibility of failure and the resultant stresses were compared with the materials’ tensile strength.
In this study, the following assumptions were made:
Enamel, dentin, and the restorative materials were assumed to be homogeneous and isotropic.
The polymerization of the restoration results in uniform volume shrinkage.
RESULTS
The results are presented in terms of Von Mises stress values in MPa.
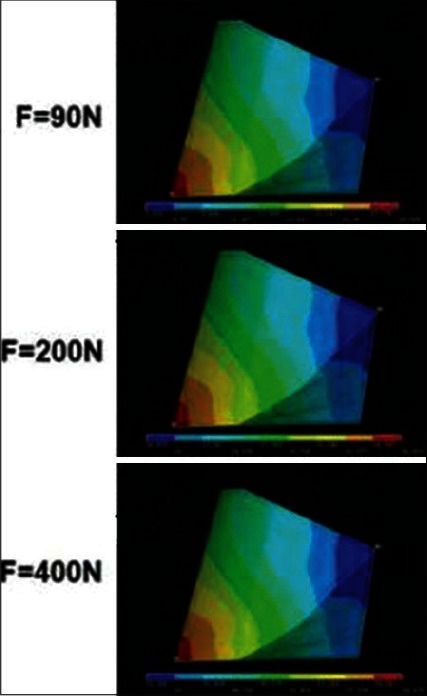
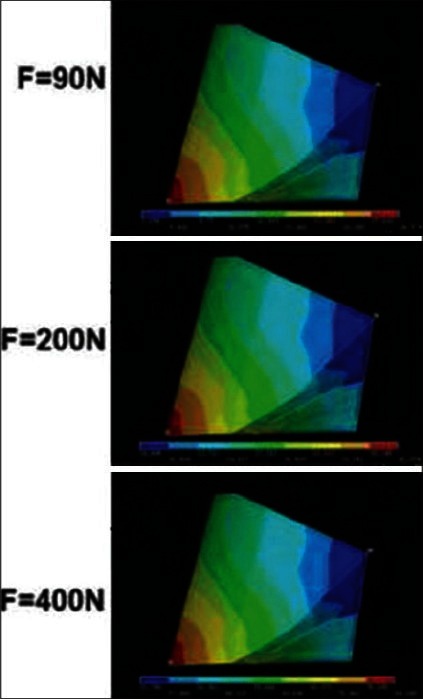
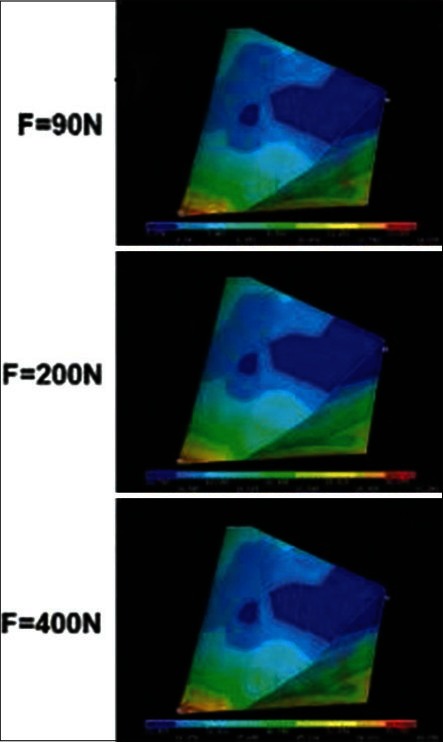
It was noticed that the Von Mises stress levels increased in direct proportion with increased loading in all the groups. Irrespective of the materials used, maximum stresses occurred at the cervical margin of the restoration [Tables 2 and 3]. The stresses in overall tooth show that, in group A [Figures 2–4], irrespective of loading condition low-shrink composite showed least stress followed by nano-RMGIC and layering technique. In group B [Figures 5–7], low-shrink composite and nano-RMGIC showed similar stresses, which were comparatively more than layering technique.
Table 2.
Von Mises stresses in tooth (MPa) with occlusal cavity (group A)

Table 3.
Von Mises stresses in tooth (MPa) without occlusal cavity (group B)

Figure 2.
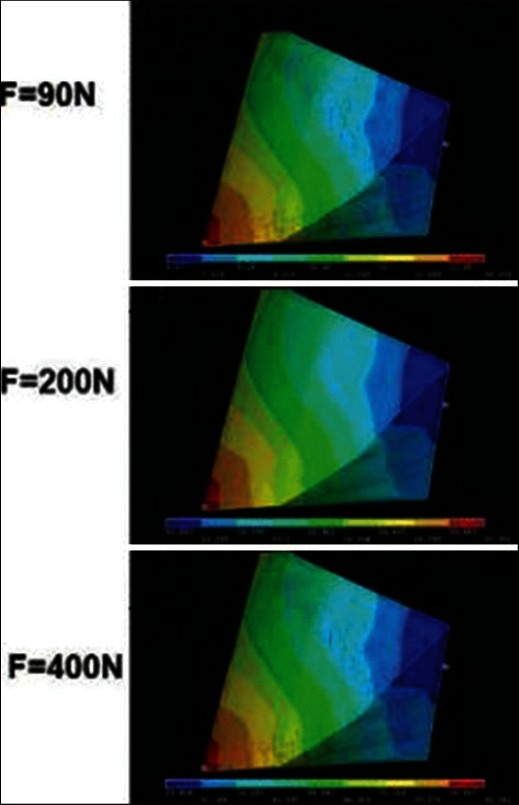
Stress distribution in low-shrink micro-hybrid composite with occlusal restoration at different loads. The value at the lower right hand side (red color) is the maximum stress and left hand side (blue color) is the least stress
Figure 4.
Stress distribution in layering technique with occlusal restoration at different loads
Figure 5.
Stress distribution in low-shrink micro-hybrid composite without occlusal restoration at different loads
Figure 7.
Stress distribution in layering technique without occlusal restoration at different loads
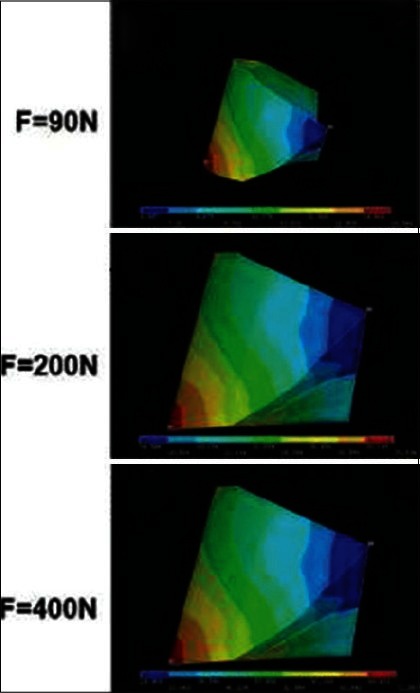
Figure 3.
Stress distribution in nano-ionomer with occlusal restoration at different loads
Figure 6.

Stress distribution in nano-ionomer without occlusal restoration at different loads
The stresses in cervical restoration show that, in group A, both low-shrink composite and nano-RMGIC resulted same stresses which were recorded to be marginally lower than layered restoration. In group B, nano-RMGIC revealed the least stress followed by low-shrink composite and layered restoration.
It was observed that the resultant maximum stresses in overall tooth and in the cervical region were higher in group B than in group A.
DISCUSSION
The scope of this study was to evaluate the mechanical behavior of various restorative materials known to be recommended or used in abfraction lesions under different loading characteristics. The possible changes in the tooth structure because of occlusal restoration, the utilized restorative material and their consequences were studied in detail.
The tooth modeled for this analysis was a mandibular first premolar. Literature review reveals highest incidence of abfraction lesions in mandibular bicuspids. The lingual orientation of mandibular bicuspids renders them more susceptible to the concentration of tensile stresses at the cervical region, the anatomically smaller cervical cross section may also contribute to the weakness of the teeth.[9]
In this study, 3D-FEA was used, which produces more accurate results compared to 2D-FEA modeling. 3D-FEA is preferred to obtain an optical realistic analysis with detailed tooth anatomy and computational process. In this study, the periodontal ligament and alveolar bone was modeled mimicking clinical situation. Modulus of elasticity of periodontal ligament is low; as a result, it allows the tooth to bottom out allowing tooth movement. Modeling periodontal ligament is important for realistic results.[10] Cementum is a very thin layer and has the same physical properties as dentin; therefore, it seemed unnecessary to define it as a separate layer from the dentin.
Our analysis reveals that, all the tooth models restored with different materials showed high resultant stresses concentrated at the cervical margin. Hence, this area is the most likely potential failure site of the restoration. This is in accordance with clinical surveys which showed a higher percentage of marginal defects in restorations of the NCCL occurring on the cervical area of the restoration.[11] From an analytical point of view, this study used different loads like 400 N, which was assumed to represent bruxism, 200 N vaguely represents the traumatic load and 90 N load was relatively modest in clinical terms.[12,13]
When a low-shrink composite was taken into consideration, in group A it showed least stresses compared to other materials. This could be attributed to the presence of adhesive layer. The necessity of stress buffering was acknowledged by Kemp-Scholte and Davidson[14,15] in the case of shrinkage stress reduction. However, this principle can be extrapolated to other functional load cases as shown by Ausiello et al.[16] The results of this study agree with the findings of Kemp-Scholte and Davidson, who reported an improvement of surface marginal integrity when a layer of adhesive resin was used in a class V composite restoration. This was attributed to an increase in strain capacity of the adhesive resin so that the restoration could deform under the loading of polymerization shrinkage.
When nano-RMGIC was taken into consideration, it developed least stresses in the cervical region of tooth with and without occlusal restoration. This may be due to the deformation and flexing of the material because of its low modulus, which absorbed the induced stresses and thus reduced the resultant stresses in the tooth. This is in accordance with Van Meerbeek et al.[17] who confirmed the correlation of improved clinical results with lower moduli of elasticity. The restorations with lower modulus of elasticity allow the restoration to flex with the tooth rather than debond.[13] On the contrary, a study[18] showed that class V lesions restored with materials of higher modulus of elasticity enabled better stress distribution. However, many studies[19] found no significant difference between materials with different elastic moduli.
When layered restoration was considered, in group A the stresses were more with this technique when compared with other two materials. But, in group B stresses were equivalent to low-shrink composite. A thick layer of RMGIC in the layered restoration acts as a stress breaker compared to the bulk filled technique.[14] In the layering technique a thin layer of a flexible material would fail in the cervical region, mainly because, its limited thickness cannot provide sufficient reduction in stress. In the case of thick layer, failure does not occur but the marginal tensile stresses are close to the failure limit.[20]
The occlusal restoration weakens the integrity of the tooth and allows greater flexing of the cusp under occlusal load.[21,22] On the contrary, in this study, teeth without occlusal restoration resulted in marginally higher stresses. For the tooth with occlusal restoration, the limited cuspal flexure may be explained by the perfect simulation of the bond between tooth and restoration, and such cusp reinforcement is achieved by the bonding agent.[23]
Failure to consider occlusion will likely lead to restorative failure as clearly demonstrated by previous studies.[22,24] Lambrechts et al.[25] pointed out that if the occlusion is not corrected, it results in premature loss of the cervical restoration. Elimination of non-axial forces can be achieved by simple occlusal equilibration, which will result in reduction or elimination of stress on the restoration. In this study, the resultants of the 90 N force can be compared to the stress obtained on occlusal correction.
The extent of the role of compressive stress versus tensile stress in the retentive failure in-vivo remains uncertain.[26] Finally any conclusions drawn by considering a single stress component will not reflect the true behavior of the tooth and hence will be far from accurate. The magnitude of stresses reported in this study are likely to be higher, since the polymerization shrinkage was assumed to be applied instantaneously where as, in reality, the shrinkage increases gradually, which may allow an opportunity for stress reduction, which cannot be simulated and calculated with computer. Small areas of de-bonding and composite flow during polymerization also may reduce the amount of stress on the tooth, in reality.[27] Studies have proven the anisotropic property of enamel and dentin and intraoral environment gives rise to nonlinearities in the periodontal ligament, residual stresses in restorative materials and inter facial stresses.[28] Such nonlinear simulations of the analysis were not carried out in this study, which will provide more realistic results. Further studies need to be carried out keeping into consideration all these factors accompanied by long-term clinical experiments.
CONCLUSION
Within the limitations of this study:
Restorative materials with low modulus of elasticity (nano-RMGIC restorative material) are successful in abfraction lesions at moderate tensile stresses whereas a higher modulus of elasticity and mechanical properties (low-shrink composites) can support higher loads and resist wear
Irrespective of occlusal restoration, low-shrink micro-hybrid composites showed good results at all the loading conditions without crossing its tensile strength limits
Irrespective of occlusal restoration, both nano-ionomer and layered technique performed well at 90 N and 200 N, but both failed at 400 N because of the resultant stresses produced beyond their tensile strength.
ACKNOWLEDGMENT
We would like to acknowledge Mr. Pawan Kumar, CAE Engineer, Bangalore, Karnataka, India.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Wood I, Jawad Z, Paisley C, Brunton P. Non-carious cervical tooth surface loss: A literature review. J Dent. 2008;36:759–66. doi: 10.1016/j.jdent.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 2.Michael JA, Townsend GC, Greenwood LF, Kaidonis JA. Abfraction: Separating fact from fiction. Aust Dent J. 2009;54:2–8. doi: 10.1111/j.1834-7819.2008.01080.x. [DOI] [PubMed] [Google Scholar]
- 3.Srirekha A, Bashetty K. Infinite to finite: An overview of finite element analysis. Indian J Dent Res. 2010;21:425–32. doi: 10.4103/0970-9290.70813. [DOI] [PubMed] [Google Scholar]
- 4.Onal B, Pamir T. The two-year clinical performance of esthetic restorative materials in noncarious cervical lesions. J Am Dent Assoc. 2005;136:1547–55. doi: 10.14219/jada.archive.2005.0085. [DOI] [PubMed] [Google Scholar]
- 5.Lee WC, Eakle WS. Possible role of tensile stress in the etiology of cervical erosive lesions of teeth. J Prosthet Dent. 1984;52:374–80. doi: 10.1016/0022-3913(84)90448-7. [DOI] [PubMed] [Google Scholar]
- 6.Tyas MJ. The class V lesion – Aetiology and restoration. Aust Dent J. 1995;40:167–70. doi: 10.1111/j.1834-7819.1995.tb05631.x. [DOI] [PubMed] [Google Scholar]
- 7.Ash MM, Nelson SJ. The permanent mandibular premolars. In: Penny Rudolph., editor. Dental Anatomy, Physiology and Occlusion. 8th edition. India: Elsevier Publishing; 2006. pp. 239–61. [Google Scholar]
- 8.Coolidge ED. The thickness of human periodontal ligament membrane. J Am Dent Assoc. 1937;24:1260–70. [Google Scholar]
- 9.Powell LV, Johnson GH, Gordon GE. Factors associated with clinical success of cervical abrasion/erosion restorations. Oper Dent. 1995;20:7–13. [PubMed] [Google Scholar]
- 10.Rees JS, Hammadeh M, Jagger DC. Abfraction lesion formation in maxillary incisors, canines and premolars: A finite element study. Eur J Oral Sci. 2003;111:149–54. doi: 10.1034/j.1600-0722.2003.00018.x. [DOI] [PubMed] [Google Scholar]
- 11.Brackett WW, Browning WD, Ross JA, Brackett MG. Two-year clinical performance of a polyacid-modified resin composite and a resin-modified glass-ionomer restorative material. Oper Dent. 2001;26:12–6. [PubMed] [Google Scholar]
- 12.Goel VK, Khera SC, Ralston JL, Chang KH. Stresses at the dentinoenamel junction of human teeth – A finite element investigation. J Prosthet Dent. 1991;66:451–9. doi: 10.1016/0022-3913(91)90504-p. [DOI] [PubMed] [Google Scholar]
- 13.Rees JS, Jacobsen PH. The effect of interfacial failure around a class V composite restoration analysed by the finite element method. J Oral Rehabil. 2000;27:111–6. doi: 10.1046/j.1365-2842.2000.00493.x. [DOI] [PubMed] [Google Scholar]
- 14.Kemp-Scholte CM, Davidson CL. Complete marginal seal of Class V resin composite restorations effected by increased flexibility. J Dent Res. 1990;69:1240–3. doi: 10.1177/00220345900690060301. [DOI] [PubMed] [Google Scholar]
- 15.Kemp-Scholte CM, Davidson CL. Marginal integrity related to bond strength and strain capacity of composite resin restorative systems. J Prosthet Dent. 1990;64:658–64. doi: 10.1016/0022-3913(90)90291-j. [DOI] [PubMed] [Google Scholar]
- 16.Ausiello P, Apicella A, Davidson CL. Effect of adhesive layer properties on stress distribution in composite restorations: A 3D finite element analysis. Dent Mater. 2002;18:295–303. doi: 10.1016/s0109-5641(01)00042-2. [DOI] [PubMed] [Google Scholar]
- 17.Van Meerbeek B, Peumans M, Verschueren M, Gladys S, Braem M, Lambrechts P, et al. Clinical status of ten dentin adhesive systems. J Dent Res. 1994;73:1690–702. doi: 10.1177/00220345940730110401. [DOI] [PubMed] [Google Scholar]
- 18.Subhashini N, Meena N, Shetty A, Kumari A, Naveen DN. Finite element analysis of stress concentration in class V restorations of four groups of restorative materials in mandibular premolar. J Conserv Dent. 2008;11:121–6. doi: 10.4103/0972-0707.45251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Browning WD, Brackett WW, Gilpatrick RO. Retention of microfilled and hybrid resin-based composite in noncarious class 5 lesions: A double-blind, randomized clinical trial. Oper Dent. 1999;24:26–30. [PubMed] [Google Scholar]
- 20.Campos PE, Barceleiro Mde O, Sampaio-Filho HR, Martins LR. Evaluation of the cervical integrity during occlusal loading of class II restorations. Oper Dent. 2008;33:59–64. doi: 10.2341/07-35. [DOI] [PubMed] [Google Scholar]
- 21.Rees JS, Jacobsen PH. The effect of cuspal flexure on a buccal class V restoration: A finite element study. J Dent. 1998;26:361–7. doi: 10.1016/s0300-5712(97)00015-8. [DOI] [PubMed] [Google Scholar]
- 22.Vasudeva G, Bogra P. The effect of occlusal restoration and loading on the development of abfraction lesions: A finite element study. J Conserv Dent. 2008;11:117–20. doi: 10.4103/0972-0707.45250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Magne P, Oganesyan T. Premolar cuspal flexure as a function of restorative material and occlusal contact location. Quintessence Int. 2009;40:363–70. [PubMed] [Google Scholar]
- 24.Van Meerbeek B, Braem M, Lambrechts P, Vanherle G. Evaluation of two dentin adhesives in cervical lesions. J Prosthet Dent. 1993;70:308–14. doi: 10.1016/0022-3913(93)90213-8. [DOI] [PubMed] [Google Scholar]
- 25.Lambrechts P, Braem M, Vanherle G. Buonocore memorial lecture. Evaluation of clinical performance for posterior composite resins and dentin adhesives. Oper Dent. 1987;12:53–78. [PubMed] [Google Scholar]
- 26.Lee WC, Eakle WS. Stress-induced cervical lesions: Review of advances in the past 10 years. J Prosthet Dent. 1996;75:487–94. doi: 10.1016/s0022-3913(96)90451-5. [DOI] [PubMed] [Google Scholar]
- 27.Carvalho RM, Pereira JC, Yoshiyama M, Pashley DH. A review of polymerization contraction: The influence of stress development versus stress relief. Oper Dent. 1996;21:17–24. [PubMed] [Google Scholar]
- 28.Wakabayashi N, Ona M, Suzuki T, Igarashi Y. Nonlinear finite element analyses: Advances and challenges in dental applications. J Dent. 2008;36:463–71. doi: 10.1016/j.jdent.2008.03.010. [DOI] [PubMed] [Google Scholar]