

Abstract
The prognosis of patients with central nervous system relapse of aggressive lymphoma is very poor with no therapy established so far. In a prospective multicenter phase II study, we evaluated a potentially curative chemotherapy-only regimen in these patients. Adult immunocompetent patients 65 years of age or under received induction chemotherapy with MTX/IFO/DEP (methotrexate 4 g/m2 intravenously (i.v.) Day 1, ifosfamide 2 g/m2 i.v. Days 3– 5 and liposomal cytarabine 50 mg intrathecally (i.th) Day 6) and AraC/TT/DEP (cytarabine 3g/m2 i.v. Days 1–2, thiotepa 40 mg/m2 i.v. Day 2 and i.th. liposomal cytarabine 50 mg i.th. Day 3) followed by high-dose chemotherapy with carmustine 400 mg/m2 i.v. Day −5, thiotepa 2×5 mg/kg i.v. Days −4 to −3 and etoposide 150 mg/m2 i.v. Days −5 to −3, and autologous stem cell transplantation Day 0 (HD-ASCT). Thirty eligible patients (median age 58 years) were enrolled. After HD-ASCT (n=24), there was a complete remission in 15 (63%), partial remission in 2 (8%) and progressive disease in 7 (29%) patients. Myelotoxicity was the most adverse event with CTC grade 3/4 infections in 12% of MTX/IFO/DEP courses, 21% of AraC/TT/DEP courses and 46% of HD-ASCT courses. The 2-year time to treatment failure was 49%±19 for all patients and 58%±22 for patients completing HD-ASCT. The protocol assessed proved feasible and highly active with long-lasting remissions in a large proportion of patients.
(ClinicalTrials.govIdentifier NCT01148173)
Introduction
Central nervous system (CNS) relapse is diagnosed in 2–5% of patients with aggressive systemic non-Hodgkin’s lymphoma after a median time of approximately six months after lymphoma diagnosis.1–6 It can occur either as an isolated event or in combination with systemic relapse. Primary extranodal involvement (particularly of the testes), elevated serum LDH and low performance status are among the most commonly reported risk factors associated with CNS relapse. On CNS relapse, neither the indication for CNS prophylaxis, nor the appropriate prophylaxis itself has been defined, nor has the most appropriate treatment been established.7
Data on therapy of secondary CNS lymphoma (SCNSL) are limited. With the exception of two prospective studies using intrathecal (i.th.) chemotherapy alone,8,9 only retrospective analyses have been published.5,10–12 With i.th. chemotherapy and/or radiotherapy, prognosis is poor with a median survival of only a few months.13 In younger patients with isolated CNS relapse, longer survival has been observed in retrospective analyses, in particular when high-dose methotrexate (HDMTX)-based chemotherapy was administered.10 However, in the vast majority of patients, it does not seem possible to offer a cure.
High-dose chemotherapy followed by stem-cell transplantation (HD-ASCT) offers a cure in relapsed systemic lymphoma.14,15 In primary CNS lymphoma (PCNSL), consolidating therapy with HD-ASCT with the blood-brain-barrier penetrating alkylating agents BCNU and thiotepa resulted in 5-year overall survival of over 80%.16,17 Small retrospective analyses have revealed long-term remissions in some patients treated with HD-ASCT for SCNSL.18–20 In a single institution retrospective analysis of 43 patients with SCNSL, long-term survival was found only in those treated with HD-ASCT.11
Here, we present the first completed prospective multicenter study to evaluate feasibility and efficacy of HD-ASCT in patients with SCNSL. The protocol was designed as a sequential application of blood-brain-barrier crossing cytostatics. To reduce the risk of delayed CNS toxicity, radiotherapy was omitted.
Design and Methods
Immunocompetent adult patients not older than 65 years with CNS relapse of systemic aggressive lymphoma with or without systemic relapse were eligible. Lymphoma had to be histologically confirmed at first diagnosis. Exclusion criteria were: Burkitt’s lymphoma/lymphoblastic lymphoma, prior therapy for SCNSL with the exception of corticosteroids, prior whole-brain or mediastinal irradiation, ECOG performance status over 2, neutrophils less than 1.5/nl, platelets less than 100/nl, bilirubin elevation, transaminases more than 3×UNL, creatinine clearance less than 50 ml/min, acute infection and pregnancy.
Staging procedures
Pre-treatment evaluation included contrast-enhanced magnetic resonance imaging (MRI) of the brain (spinal MRI on clinical suspicion only), lumbar puncture with cerebrospinal fluid (CSF) cytomorphological and immunocytological (if possible) evaluation, computed tomography (CT) of chest and abdomen, and bone marrow biopsy. In addition, laboratory testing with whole blood count, liver enzymes, lactate dehydrogenase (LDH), serum protein and electrophoresis, creatinine clearance, and hepatitis and HIV serology were performed. All patients gave their written informed consent, and the study was approved by the ethics committees of all participating centers.
CNS relapse was defined as at least one of the following: i) cytomorphological or immunocytological proof of lymphoma cells in the CSF; ii) clinical symptoms and meningeal enhancement on MRI; iii) parenchymal brain lesions on MRI with radiomorphology consistent with CNS lymphoma.21 Biopsy of parenchymal lesions for histological proof of diagnosis was not mandatory but strongly encouraged in patients with CNS lesions occurring more than two years after first lymphoma diagnosis.
Study design
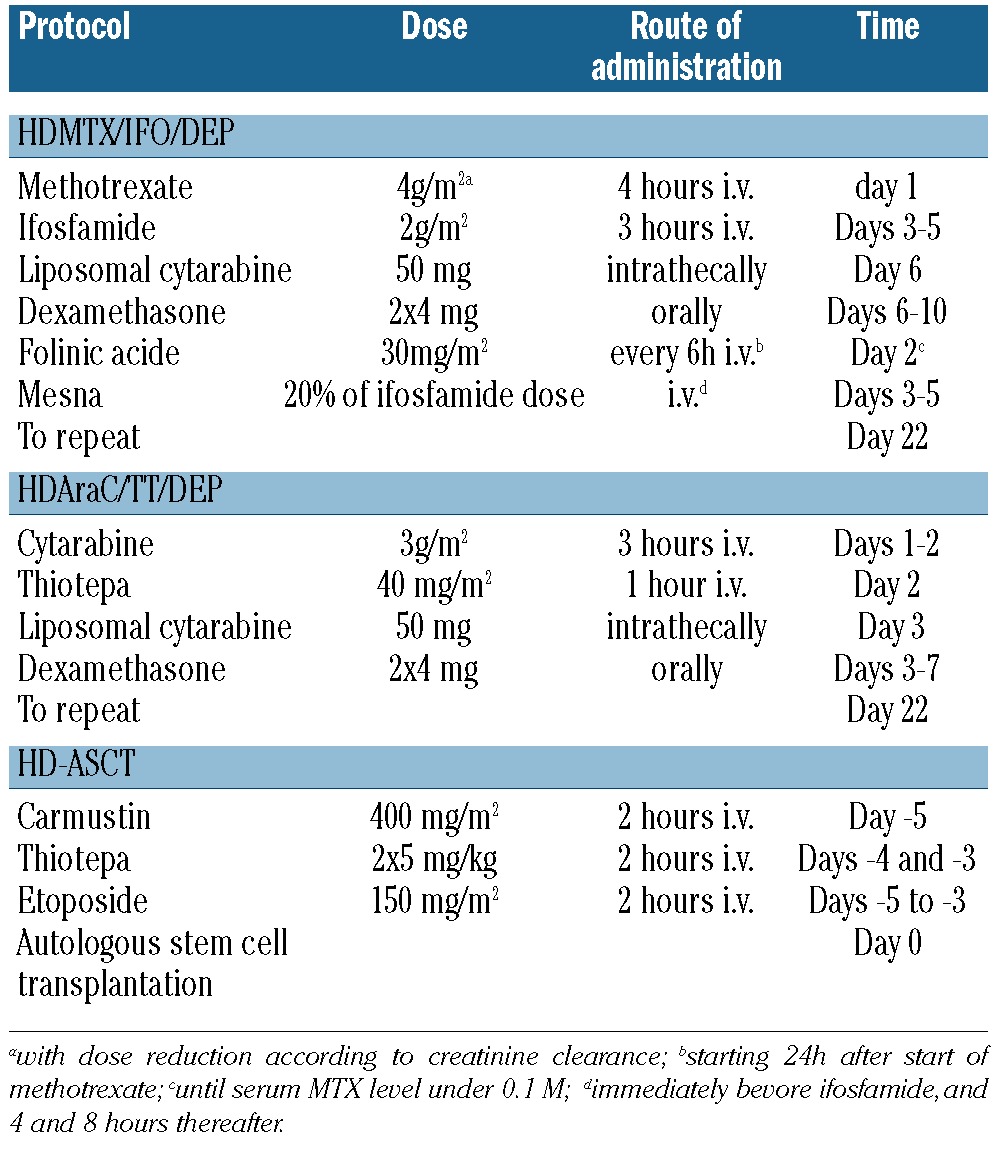
This was an open-label multicenter phase II trial. The treatment schedule consisted of three courses of induction therapy in responders followed by HD-ASCT (Table 1). All patients initially received one course HDMTX/IFO/DEP: methotrexate 4 g/m2/4 h i.v. Day 1, ifosfamide 2 g/m2/3 h i.v. Days 3–5, dexamethasone 2×4 mg orally Days 6-10 and liposomal cytarabine 50 mg i.th. by lumbar puncture Day 6. Methotrexate dose was adjusted to creatinine clearance as reported.22 Supportive therapy included vigorous intravenous hydration, urine alkalization and leukovorin rescue 30 mg/m2 every 6 h starting 24 h after start of HDMTX. In patients without lymphoma progression on Day 22 of the first HDMTX/IFO/DEP course, therapy was continued with a second HDMTX/IFO/DEP course; progressing patients were switched to HDAraC/TT/DEP: cytarabine 3 g/m2/3 h i.v. Days 1–2, thiotepa 40 mg/m2/1 h i.v. Day 2, dexamethasone 2x4 mg orally Days 3–7 and liposomal cytarabine 50 mg intrathecally Day 3. Prior to autologous stem cell mobilization, G-CSF 2×5 mg/kg was given subcutaneously starting on Day 7 after the second induction course. A minimum of 2×106 CD34+ cells per kg of body weight were required. A third course of induction chemotherapy with HDAraC/TT/DEP with response evaluation on Day 22 was given to all patients subsequently. All responding patients later received HD-ASCT. Patients not responding to induction chemotherapy without clinical deterioration were allowed to proceed to HD-ASCT at the discretion of the physician in charge; all others were treated off protocol. HD-ASCT included: carmustin 400 mg/m2/2 h i.v. Day −5, thiotepa 2×5 mg/kg/2 h i.v. Days −4 and −3 and etoposide 150 mg/m2/2 h i.v. Days −5 to −3 followed by ASCT on Day 0. Standard supportive measures were taken according to institutional guidelines. There was no obligatory antibacterial, antiviral or antimycotic prophylaxis, or obligatory G-CSF administration during the induction therapy.
Table 1.
Chemotherapy regimen.
Response and toxicity evaluation
Response was assessed by CSF examination and/or MRI (whichever revealed pathological results prior to treatment) after the first and the third induction therapy courses and following HD-ASCT. During follow up, CSF examination and MRI, as well as CT of chest and abdomen and bone marrow examination (in patients with systemic involvement at study entry or at clinical suspicion) were performed every three months. Systemic response was evaluated according to Cheson criteria.23 CNS response was evaluated according to agreed response criteria for PCNSL.24 Complete remission (CR) was defined as complete disappearance of all lymphoma-caused MRI abnormalities and clearance of lymphoma cells in the CSF in at least two consecutive CSF examinations as well as complete resolution of all lymphoma-caused clinical symptoms. Partial remission (PR) was applicable only to patients with parenchymal lesions visible on MRI and was defined as a 50% or more reduction in all lesions without new lesions irrespective of lymphoma cells detectable in the CSF. No change (NC) was defined as stable/improved clinical symptoms with a less than 50% reduction in parenchymal lesions or less than 25% growth. Progressive disease (PD) was defined as appearance of new symptoms or lesions or more than 25% growth of parenchymal lesions or increase in lymphoma cell number in the CSF. Appearance of new symptoms or of new lymphoma lesions after a CR lasting more than two months was defined as relapse, and cases of shorter response duration as progression. Treatment toxicity was graded according to NCI CTC criteria. For each patient, only the maximal toxicity grade was registered.
Statistical analysis
All 30 patients matching the inclusion/exclusion criteria were included in the intent-to-treat analysis. Primary end point was time to treatment failure (TTF) measured from start of study therapy (for HD-ASCT from time of ASCT) to first progression, relapse or death due to lymphoma or to therapy-related toxicity. Secondary end points were response, toxicity and overall survival. There was no formal sample size estimation due to the low frequency of SCNSL. However, in the study protocol we stated that, depending on the observed frequencies, 95% confidence limits would have a range of 10–20%. For the primary end point, we expected a very low frequency of event free subjects. This was based on the assumption of an overall survival of 50% after six months.5,11 Assuming an exponential survival after 24 months we could expect only 12.5% to have survived. As the event rate for TTF was assumed to be smaller, we expected a proportion of less than 10% of event free subjects. For 10% event-free subjects, the 95% confidence limit would have been 2.1–26.5% (exact binomial distribution, ignoring censoring). However, in our study, results were much more favorable with a TTF rate after two years of approximately 50%. Therefore, precision of observed results is approximately ±20%.
The Kaplan-Meier method was used to estimate survival probabilities with 95% confidence interval (CI). Significance tests were carried out with type 1 error = 5% (two-sided). However, with 15 events, hazard ratios (HR) only as large as 4.3 or higher could have been detected in survival analyses (type 1 error 0.05, two-sided, power 80%). SPSS for Windows (release 18.0) was used for all statistical analysis.
Results
Patients’ characteristics
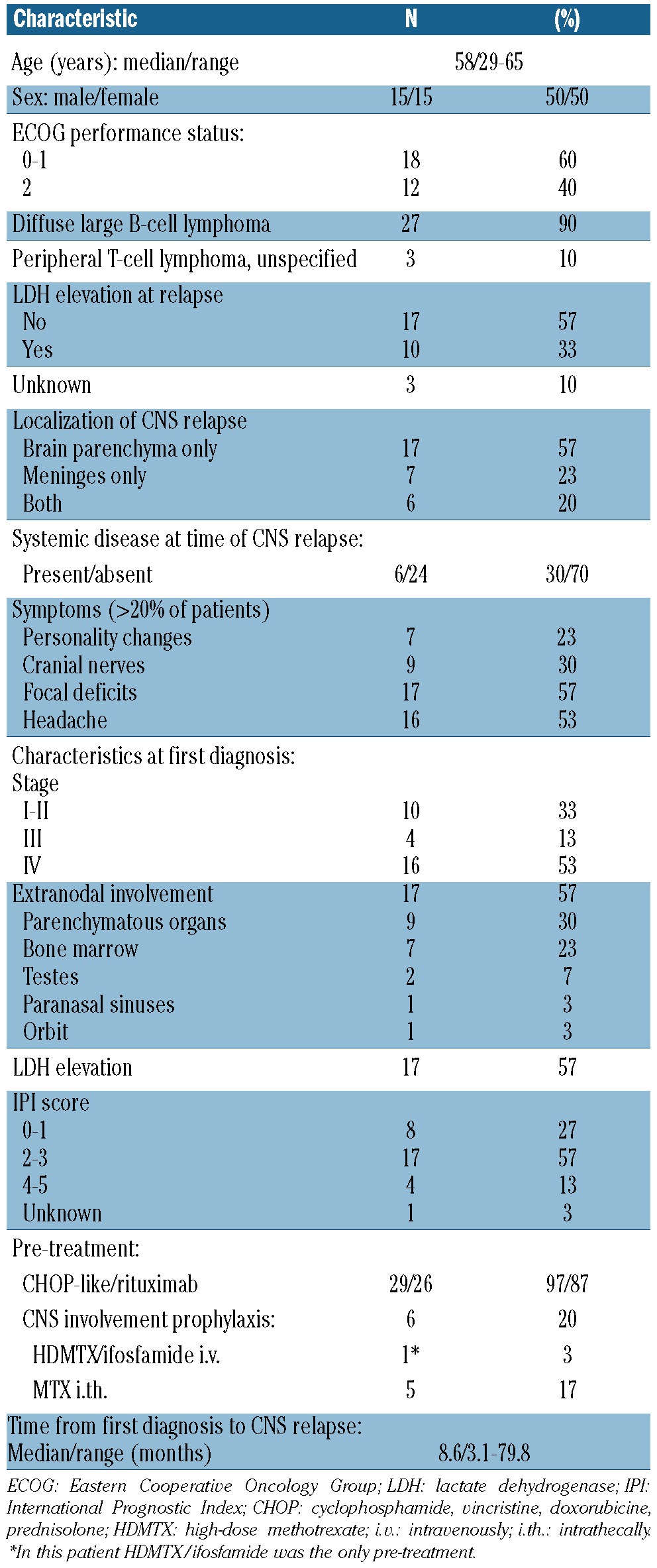
Thirty-three patients with a median age of 58 years were screened. Three of those did not meet the inclusion criteria (one with Burkitt’s lymphoma and 2 with CNS relapse of PCNSL). Therefore, 30 patients were enrolled and considered as the intent-to-treat population (Table 2). The original lymphoma diagnosis was confirmed by reference pathology (pathologists` panel of the German HighGrade Non-Hodgkin’s Lymphoma Study Group) in all patients. All patients were pre-treated with only one treatment regimen.
Table 2.
Patients’ characteristics.
Treatment and response
MTX dose had to be reduced due to creatinine clearance of less than 100 ml/min in 2 patients once and in one patient twice. Intrathecal application of liposomal cytarabine was omitted in 2 patients on HDMTX/IFO/DEP and in 4 patients on HDAraC/TT/DEP at the discretion of the physician in charge.
After the first HDMTX/IFO/DEP course, CR was achieved in the CNS in 5 (17%), PR in 14 (47%) and NC in 6 (20%) patients (Figure 1). Response was not evaluated in 5 patients (17%): 4 with clinical improvement (due to decision of the physician in charge) and one who died of septic colitis prior to response evaluation. Of 29 patients proceeding to the second induction course, 27 continued with a second course of HDMTX/IFO/DEP and 2 were switched to HDAraC/TT/DEP (due to transaminases elevation grade 4 and worsening of clinical symptoms in one patient each). One of those had PD in the CNS after the second HDMTX/IFO/DEP and died 3.5 months after study entry without further therapy, and one patient in CR refused further chemotherapy, received WBRT and was alive 28 months after study entry. Twenty-seven patients continued induction therapy: one with HDMTX/IFO/DEP due to the decision of the physician in charge and 26 with HDAraC/TT/DEP. At the end of induction chemotherapy, CR was documented in 7 (26%), PR in 13 (48%), NC in 2 (7%) and PD in 4 patients (15%); in one patient (4%) no response evaluation after complete induction therapy was performed. In all patients, autologous stem cells could be collected in sufficient numbers as planned in the study protocol. The median number of CD34+ cells collected was 5.3×106/kg.
Figure 1.
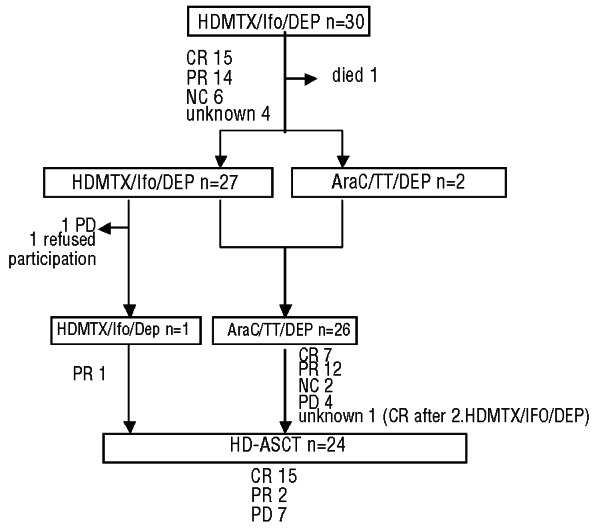
Course of therapy and response. Note that one patient with progressive disease after AraC/TT/DEP received HD-ASCT. HDMTX/IFO/DEP: high-dose methotrexate, ifosfamide and liposomal cytarabine intrathecally; CR: complete response; PR: partial response; NC: no change; HDAraC/TT/DEP: high-dose cytarabine, thiotepa and liposomal cytarabine intrathecally; PD: progressive disease; HD-ASCT: high-dose chemotherapy followed by autologous stem-cell transplantation.
HD-ASCT was given to a total of 24 patients, since one patient with PD but stable symptoms received it at the discretion of the physician in charge. The median number of CD34+ cells reinfused was 3.6×106/kg.
After HD-ASCT, CR was documented in 15 (63%), PR in 2 (8%) and PD in 7 (29%) patients.
Of the 6 patients with concomitant systemic lymphoma, one patient achieved systemic CR following induction therapy and maintained it after HD-ASCT, 3 patients achieved PR after induction therapy and had CR (n=2) or PR (n=1) after HD-ASCT, one had systemic PR after induction therapy, but progressed in the CNS, and one had NC after induction therapy and responded partially to HD-ASCT.
Toxicity
Toxicity was mainly hematologic. Anemia grade 3 was reported in 8 of 58 (14%) of HDMTX/Ifo/Dep courses, in 12 of 28 (43%) of HDAraC/TT/DEP courses and in 8 of 24 (33%) of HD-ASCT courses, anemia grade 4 in 1 of 58 (2%), 2 of 28 (7%) and 2 of 24 (8%) of courses, respectively. Leukopenia grade 3 was reported in 12 of 58 (21%) of HDMTX/Ifo/Dep courses and in 4 of 28 (14%) of HDAraC/TT/DEP courses, grade 4 in 9 of 58 (16%) and in 13 of 28 (46%) courses, respectively, and in all HD-ASCT courses. Thrombopenia grade 3 occurred in 5 of 58 (9%) of HDMTX/Ifo/DEP courses and grade 4 in 3 of 58 (5%) of HDMTX/Ifo/DEP courses, in 16 of 28 (57%) of HDAraC/TT/DEP courses and all HD-ASCT courses. There was a grade 3 infection in 5 of 58 (9%) of HDMTX/Ifo/DEP courses, 6 of 28 (21%) HDAraC/TT/DEP courses and 10 of 24 (42%) HD-ASCT courses. Grade 4 infection was registered in 2 of 58 (3%), 0 and 1 of 24 (4%) courses, respectively. Other frequent toxicities were: transaminase elevation grade 3 in 9 of 30 (30%) patients on HDMTX/Ifo/DEP, stomatitis grade 3 in 4 of 24 (17%) patients and grade 4 in 3 of 24 patients (13%) on HD-ASCT, and grade 3 diarrhea in one of 30 patients (3%) on HDMTX/Ifo/DEP and in 3 of 24 patients (13%) on HD-ASCT. Additionally, nausea/vomiting grade 3 was documented in one of 25 patients (4%) on HDAraC/TT/DEP and in 2 of 24 patients (8%) on HD-ASCT, grade 3 headache in 2 of 23 patients (9%) on HDAraC/TT/DEP, bilirubine elevation grade 3 and pneumonitis grade 4 in one patient each on HDMTX/IFO/DEP, and confusion grade 3 in one of 30 patients (3%) on HDMTX/IFO/DEP and one of 24 patients (4%) on HDAraC/TT/DEP.
There was one death on therapy; a 62-year old patient developed a diverticulitis during the first course of HDMTX/IFO/DEP and succumbed due to neutropenic septicemia. In follow up, one patient developed an irreversible cauda equina syndrome with bladder and bowel dysfunction.
Outcome and follow up
Of 4 patients with PD after induction therapy, 3 died without further treatment two, six and eight months after study entry due to lymphoma, and one patient received salvage WBRT but relapsed and died 14 months after study entry.
Seventeen patients were in remission after HD-ASCT: 15 had CR and 2 PR. Two of 7 patients with PD after HD-ASCT received i.th. chemotherapy and died of lymphoma six and nine months after study entry, respectively. One patient was rescued with WBRT but relapsed and died after 13 months, and 4 died of progression without further treatment (after 11, 6, 6 and 8 months, respectively).
After a median follow up of 21 months (95%CI: 10–32) 17 patients were alive by intent-to-treat analysis. The 2-year TTF was 49%±19 for all patients (Figure 2A) and 58%±22% for patients completing HD-ASCT (Figure 2C); median TTF was 12 months (95%CI: 0–34.9) and 24.3 months (95%CI: 5.9–42.8), respectively. The 2-year OS was 63±19% for all patients (Figure 2B) and 68±20% after HD-ASCT (Figure 2D); the median OS has not been reached in either group.
Figure 2.

(A) Time to treatment failure (TTF) for all patients (n=30). (B) Overall survival (OS) for all patients. (C) TTF for patients with highdose chemotherapy and autologous stem cell transplantation (HD-ASCT; n=24). (D) OS for HD-ASCT patients. For analysis B and D, time at risk started at the beginning of HD-ASCT.
Secondary relapse or progressive disease was localized in the CNS in 11 of 16 patients (69%), outside the CNS in 3 (19%) patients (kidney, lymph nodes/bone marrow and bone marrow alone in one patient each), and both in and outside the CNS in 2 (13%) patients.
No significant difference was found for either OS or TTF when the following factors were examined: meningeal versus parenchymal involvement, normal LDH at CNS relapse versus elevated, ECOG at CNS relapse 0–1 versus 2, CNS relapse within 12 months after first lymphoma diagnosis versus later. However, regarding OS and TTF for all patients, those with ECOG performance of 2 compared to patients with ECOG 0 or 1 and patients with parenchymal involvement compared to patients with meningeal involvement showed approximately 2-fold to 3-fold hazard ratios (ECOG: HR=2.9, P=0.053, and HR=2.2, P=0.12, parenchymal involvement: HR=2.17, P=0.31, and HR=1.92, P=0.31). Regarding OS and TTF for HD-ASCT patients, those with CNS relapse after 12 months or later showed a 2-fold hazard ratio (HR=2.50, P=0.18 and HR=2.04, P=0.27) as compared to patients with relapse within 12 months. All other hazard ratios were smaller than 2 and are not reported.
Discussion
The prognosis of SCNSL is dismal and cure is only achieved in exceptional cases. In this study, a novel potentially curative chemotherapeutic regimen was evaluated. The protocol was based exclusively on cytostatics both highly active in lymphoma and capable of penetrating the intact blood-brain barrier. The HDMTX/IFO combination proved tolerable and highly active with a response rate of 90% in a pilot study with 20 patients.25 Intrathecal therapy with liposomal AraC was added to the present protocol based on its higher effectiveness compared to conventional i.th. cytarabine in patients with lymphomatous meningitis in terms of tumor clearance rate, time to neurological progression, and survival, as well as longer half-life allowing longer administration intervals.8 The HD-ASCT regimen with BCNU and thiotepa has been successfully applied to patients with PCNSL with an estimated survival probability of 87% at both three and five years, however, with WBRT in all patients.16,17 In the present study a similar regimen was used. However, etoposide has been added based on the analysis of the German High-Grade Non-Hodgkin's Lymphoma Study Group, which found etoposide an independent prognostic factor for the prevention of CNS recurrence.2,5 The choice of the high-dose regimen seems of great importance in CNS lymphoma since disappointing treatment results have been reported in PCNSL with the BEAM (BCNU, etoposide, low-dose cytarabine and melphalan) protocol with a median event-free survival of only 9.3 months for the 14 patients who underwent transplantation.26 We decided not to use rituximab for B-cell lymphoma in this protocol owing to its negligible CNS penetration and thus assumed negligible contribution to treatment success for the most important prognostic factor, CNS disease. Moreover, rituximab was considered to have been part of the initial therapy applied to these patients shortly before study entry. WBRT was omitted in the present study to minimize the risk of delayed CNS toxicity. Moreover, when given after primary HDMTX-based chemotherapy, it did not significantly prolong overall survival in patients with PCNSL in a randomized phase III study.27
Our patients are extremely comparable to other SCNSL patients in the rituximab era reported so far. Interestingly, with the introduction of rituximab, a change in relapse localization seems to have occurred. The relatively low frequency of simultaneous systemic relapse of 20% in our patients is comparable to other more recent studies: 30.4% in the study of Schmitz et al., 41.4% in the study of Boehme et al., and 21% in the study of Villa et al.2,5,28 probably reflecting more efficacy of rituximab in controlling the systemic disease as compared to the CNS. The rather frequent brain parenchyma involvement of 77% observed in the present study corresponds to findings of others: 43.3% in the study of Boehme et al. and 84% in the study of Villa et al. It may be speculated that the inclusion of both patients with parenchymal and meningeal relapse might have introduced some heterogeneity since an impact on prognosis for parenchymal relapse is suggested in this study.
The present study is the first to evaluate a potentially curative protocol in SCNSL. Remarkably good results were achieved with a median OS of over 30 months and a 2-year OS of 63% in patients whose prognosis is generally regarded very poor. The effectiveness of the protocol used did not seem different from that observed in patients with T-cell lymphoma, all of whom responded. Our protocol within a prospective study compares very favorably to other treatment strategies for this entity. In a retrospective multicenter analysis of 113 patients (median age 61 years, 62% treated with HDMTX and 53% with WBRT) a median OS of 1.6 years has been reported.10 In another retrospective study, a median OS of seven months has been outlined based on a dual-center analysis of 23 patients with isolated CNS relapse, all of whom received an intensive HDMTX-based chemotherapy including i.th. chemotherapy in 15.12 A retrospective analysis of the German High-Grade Non-Hodgkin’s Lymphoma Study Group for patients under 61 years of age revealed a median OS of only five months for patients with CNS relapse of DLBCL (n=56; median age 50.5 years).5 The results of the present study suggest that our protocol is potentially curative in almost half of the patients suffering from CNS relapse of aggressive lymphoma. The long-term results of the present study seem similar to those achieved in patients with systemic relapse of aggressive lymphoma14 suggesting, together with the lack of systemic progress in the majority of patients, that SCNSL does not necessarily represent a refractory condition, but rather needs to be treated with substances targeting the CNS compartment. These substances, in addition, need to be administered at high doses in the setting of HD-ASCT. Obviously, this regimen is associated with more toxicity than palliative treatment strategies limiting its use to younger and fitter patients. Treatment-related mortality of 3%, however, is no higher than in other studies on systemic aggressive lymphomas. Moreover, the risk of infectious complications can likely be reduced by the prophylactic use of antibiotics and G-CSF, so its routine implementation into our protocol can be recommended.
Early relapse (<12 months) is reportedly a negative prognostic factor in patients with systemic relapse of DLBCL.14 No prognostic factors in CNS relapse have been established so far. In a retrospective analysis of 43 heterogeneously treated patients, LDH and CNS response to therapy proved to be the only independent prognostic factors for survival in multivariate analysis.11 In the present study, none of the potential prognostic factors examined proved significant, probably due to the small number of patients. However, hazard ratios for “ECOG 0–1” and “time to relapse under 12 months” were higher than 2, suggesting a prognostic role that should be validated in the future.
Since the protocol used here was very complex, it is not possible to estimate the contribution of each component. However, the complexity seems justifiable regarding the otherwise dismal prognosis of SCNSL. The relatively small number of patients is a further limitation of our study. Regarding the low frequency of CNS relapses in lymphoma, and given the study design, it did not appear realistic to include more patients.
In summary, the protocol evaluated in this prospective trial proved highly active with acceptable toxicity. Its curative potential remains to be confirmed, and a study addressing this question in a larger patient cohort is underway.
Supplementary Material
Acknowledgments
The authors would like to thank the Competence Network on Malignant Lymphoma (Kompetenznetz Maligne Lymphome) and Arbeitsgemeinschaft Internistische Onkologie for logistical support and the International Collaborative Primary CNS Lymphoma Study Group for fruitful discussions of interim results during the study.
Footnotes
Funding
This work was supported by a grant from Mundipharma GmbH.
Disclosures
Presented in part at the 11th International Conference on Malignant Lymphoma, Lugano, Switzerland, June 15-18, 2011, and at the American Society of Clinical Oncology Annual Meeting, Chicago, Illinois, June 4-8, 2011.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Bierman P, Giglio P. Diagnosis and treatment of central nervous system involvement in non-Hodgkin's lymphoma. Hematol Oncol Clin North Am. 2005; 19(4):597–609 [DOI] [PubMed] [Google Scholar]
- 2.Boehme V, Zeynalova S, Kloess M, Loeffler M, Kaiser U, Pfreundschuh M, et al. Incidence and risk factors of central nervous system recurrence in aggressive lymphoma--a survey of 1693 patients treated in protocols of the German High-Grade Non-Hodgkin's Lymphoma Study Group (DSHNHL). Ann Oncol. 2007;18(1):149–57 [DOI] [PubMed] [Google Scholar]
- 3.Boehme V, Schmitz N, Zeynalova S, Loeffler M, Pfreundschuh M. CNS events in elderly patients with aggressive lymphoma treated with modern chemotherapy (CHOP-14) with or without rituximab: an analysis of patients treated in the RICOVER-60 trial of the German High-Grade Non-Hodgkin Lymphoma Study Group (DSHNHL). Blood. 2009; 113(17):3896–902 [DOI] [PubMed] [Google Scholar]
- 4.Feugier P, Virion JM, Tilly H, Haioun C, Marit G, Macro M, et al. Incidence and risk factors for central nervous system occurrence in elderly patients with diffuse large-B-cell lymphoma: influence of rituximab. Ann Oncol. 2004;15(1):129–33 [DOI] [PubMed] [Google Scholar]
- 5.Schmitz N, Zeynalova S, Glass B, Kaiser U, Cavallin-Stahl E, Wolf M, et al. CNS disease in younger patients with aggressive B-cell lymphoma: an analysis of patients treated on the Mabthera International Trial and trials of the German High-Grade Non-Hodgkin Lymphoma Study Group. Ann Oncol. 2012;23(5):1267–73 [DOI] [PubMed] [Google Scholar]
- 6.van Besien K, Ha CS, Murphy S, McLaughlin P, Rodriguez A, Amin K, et al. Risk factors, treatment, and outcome of central nervous system recurrence in adults with intermediate-grade and immunoblastic lymphoma. Blood. 1998;91(4):1178–84 [PubMed] [Google Scholar]
- 7.Korfel A. Prevention of central nervous system relapses in diffuse large B-cell lymphoma: which patients and how¿ Curr Opin Oncol. 2011;23(5):436–40 [DOI] [PubMed] [Google Scholar]
- 8.Glantz MJ, LaFollette S, Jaeckle KA, Shapiro W, Swinnen L, Rozental JR, et al. Randomized trial of a slow-release versus a standard formulation of cytarabine for the intrathecal treatment of lymphomatous meningitis. J Clin Oncol. 1999;17(10):3110–6 [DOI] [PubMed] [Google Scholar]
- 9.Grossman SA, Finkelstein DM, Ruckdeschel JC, Trump DL, Moynihan T, Ettinger DS. Randomized prospective comparison of intraventricular methotrexate and thiotepa in patients with previously untreated neoplastic meningitis. Eastern Cooperative Oncology Group. J Clin Oncol. 1993;11(3):561–9 [DOI] [PubMed] [Google Scholar]
- 10.Doolittle ND, Abrey LE, Shenkier TN, Tali S, Bromberg JE, Neuwelt EA, et al. Brain parenchyma involvement as isolated central nervous system relapse of systemic non-Hodgkin lymphoma: an International Primary CNS Lymphoma Collaborative Group report. Blood. 2008;111(3):1085–93 [DOI] [PubMed] [Google Scholar]
- 11.Jahnke K, Thiel E, Martus P, Schwartz S, Korfel A. Retrospective study of prognostic factors in non-Hodgkin lymphoma secondarily involving the central nervous system. Ann Hematol. 2006;85(1):45–50 [DOI] [PubMed] [Google Scholar]
- 12.Patrij K, Reiser M, Watzel L, Pels H, Kowoll A, Herrlinger U, et al. Isolated central nervous system relapse of systemic lymphoma (SCNSL): clinical features and outcome of a retrospective analysis. Ger Med Sci. 2011;Vol. 9, ISSN 1612-3174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Herrlinger U, Forschler H, Kuker W, Meyermann R, Bamberg M, Dichgans J, et al. Leptomeningeal metastasis: survival and prognostic factors in 155 patients. J Neurol Sci. 2004;223(2):167–78 [DOI] [PubMed] [Google Scholar]
- 14.Gisselbrecht C, Glass B, Mounier N, Singh Gill D, Linch DC, Trneny M, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(27):4184–90 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Philip T, Chauvin F, Armitage J, Bron D, Hagenbeek A, Biron P, et al. Parma international protocol: pilot study of DHAP followed by involved-field radiotherapy and BEAC with autologous bone marrow transplantation. Blood. 1991;77(7):1587–92 [PubMed] [Google Scholar]
- 16.Illerhaus G, Marks R, Ihorst G, Guttenberger R, Ostertag C, Derigs G, et al. High-Dose Chemotherapy With Autologous Stem-Cell Transplantation and Hyperfractionated Radiotherapy As First-Line Treatment of Primary CNS Lymphoma. J Clin Oncol. 2006;24(24):3875–80 [DOI] [PubMed] [Google Scholar]
- 17.Illerhaus G, Muller F, Feuerhake F, Schäfer AO, Ostertag C, Finke J. High-dose chemotherapy and autologous stem-cell transplantation without consolidating radiotherapy as first-line treatment for primary lymphoma of the central nervous system. Haematologica. 2008;93(1):147–8 [DOI] [PubMed] [Google Scholar]
- 18.Alvarnas JC, Negrin RS, Horning SJ, Hu WW, Long GD, Schriber JR, et al. Highdose therapy with hematopoietic cell transplantation for patients with central nervous system involvement by non-Hodgkin's lymphoma. Biol Blood Marrow Transplant. 2000;6(3A):352–8 [DOI] [PubMed] [Google Scholar]
- 19.Kasamon YL, Jones RJ, Piantadosi S, Ambinder RF, Abrams RA, Borowitz MJ, et al. High-dose therapy and blood or marrow transplantation for non-Hodgkin lymphoma with central nervous system involvement. Biol Blood Marrow Transplant. 2005;11(2):93–100 [DOI] [PubMed] [Google Scholar]
- 20.Williams CD, Pearce R, Taghipour G, Green ES, Philip T, Goldstone AH. Autologous bone marrow transplantation for patients with non-Hodgkin's lymphoma and CNS involvement: those transplanted with active CNS disease have a poor outcome--a report by the European Bone Marrow Transplant Lymphoma Registry. J Clin Oncol. 1994;12(11):2415–22 [DOI] [PubMed] [Google Scholar]
- 21.Kuker W, Nagele T, Thiel E, Weller M, Herrlinger U. Primary central nervous system lymphomas (PCNSL): MRI response criteria revised. Neurology. 2005;65(7):1129–31 [DOI] [PubMed] [Google Scholar]
- 22.Jahnke K, Korfel A, Martus P, Weller M, Herrlinger U, Schmittel A, et al. High-dose methotrexate toxicity in elderly patients with primary central nervous system lymphoma. Ann Oncol. 2005;16(3):445–9 [DOI] [PubMed] [Google Scholar]
- 23.Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, et al. Report of an international workshop to standardize response criteria for non-Hodgkin's lymphomas. NCI Sponsored International Working Group. J Clin Oncol. 1999;17(4):1244. [DOI] [PubMed] [Google Scholar]
- 24.Abrey LE, Batchelor TT, Ferreri AJ, Gospodarowicz M, Pulczynski EJ, Zucca E, et al. Report of an international workshop to standardize baseline evaluation and response criteria for primary CNS lymphoma. J Clin Oncol. 2005;23(22):5034–43 [DOI] [PubMed] [Google Scholar]
- 25.Fischer L, Korfel A, Kiewe P, Neumann M, Jahnke K, Thiel E. Systemic high-dose methotrexate plus ifosfamide is highly effective for central nervous system (CNS) involvement of lymphoma. Ann Hematol. 2009;88(2):133–9 [DOI] [PubMed] [Google Scholar]
- 26.Abrey LE, Moskowitz CH, Mason WP, Crump M, Stewart D, Forsyth P, et al. Intensive methotrexate and cytarabine followed by high-dose chemotherapy with autologous stem-cell rescue in patients with newly diagnosed primary CNS lymphoma: an intent-to-treat analysis. J Clin Oncol. 2003;21(22):4151–6 [DOI] [PubMed] [Google Scholar]
- 27.Thiel E, Korfel A, Martus P, Kanz L, Griesinger F, Rauch M, et al. High-dose methotrexate with or without whole brain radiotherapy for primary CNS lymphoma (G-PCNSL-SG-1): a phase 3, randomised, non-inferiority trial. Lancet Oncol. 2010;11(11):1036–47 [DOI] [PubMed] [Google Scholar]
- 28.Villa D, Connors JM, Shenkier TN, Gascoyne RD, Sehn LH, Savage KJ. Incidence and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: the impact of the addition of rituximab to CHOP chemotherapy. Ann Oncol. 2010;21(5):1046–52 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.