

Abstract
IKZF1 gene deletions have been associated with a poor outcome in pediatric precursor B-cell acute lymphoblastic leukemia. To assess the prognostic relevance of IKZF1 deletions for patients treated on Berlin-Frankfurt-Münster Study Group trial ALL-BFM 2000, we screened 694 diagnostic acute lymphoblastic leukemia samples by Multiplex Ligation-dependent Probe Amplification. Patients whose leukemic cells bore IKZF1 deletions had a lower 5-year event-free survival (0.69±0.05 vs. 0.85±0.01; P<0.0001) compared to those without, mainly due to a higher cumulative incidence of relapses (0.21±0.04 vs. 0.10±0.01; P=0.001). Although IKZF1 deletions were significantly associated with the P2RY8-CRLF2 rearrangement, their prognostic value was found to be independent from this association. Thus, IKZF1 deletion is an independent predictor of treatment outcome and a strong candidate marker for integration in future treatment stratification strategies on ALL-BFM protocols.
Clinicaltrials.gov identifier: NCT00430118
Introduction
Approximately 20% of children with acute lymphoblastic leukemia (ALL) still suffer from relapse and may benefit from improved risk stratification and adapted treatment strategies. In this context, the influence of IKZF1 gene aberrations on therapeutic outcome has received much attention in recent investigations. IKZF1 encodes for Ikaros, a zinc-finger transcription factor family member, which functions sequence-specific in transcriptional regulation and chromatin remodeling and is required for the development of all lymphoid line-ages.1–3 Somatic aberrations of IKZF1 have recurrently been observed in precursor B-cell ALL (pB-ALL), most frequently in those carrying a BCR/ABL1 rearrangement, and have been shown to confer a poor treatment outcome.4–13 However, aberrations of IKZF1 were also found to associate with additional genetic alterations recurrently observed in childhood ALL, such as JAK mutations and translocations involving the chemokine receptor like factor 2 (CRLF2) gene.4,7,14–18
Juxtaposition of CRLF2 to the IgH@ enhancer or the P2RY8 promoter leads to elevated expression of wild-type CRLF2 in ALL and has been shown to exert a negative prognostic impact on outcome.17,18 However, the prognostic relevance seems to be treatment-dependent and it is not clear yet whether the prognostic impact of IKZF1 is independent of these concurrent lesions.19 In the present study, we assessed the prognostic role of IKZF1 deletions in a large cohort of 694 pediatric ALL patients treated according to the ALL-BFM 2000 protocol.
Design and Methods
Patients
In accordance with institutional review board regulations, clinical samples were obtained from children with ALL before treatment. The study was approved by the institutional review board of the Hannover Medical School, Hannover, Germany, and informed consent obtained from patients and/or their legal guardians in accordance with the Declaration of Helsinki. Diagnostics, risk group assignment, and treatment were performed according to the ALL-BFM 2000 protocol.20–22 Risk group stratification (standard risk, SR; intermediate risk, IR; high risk, HR) was mainly based on minimal residual disease (MRD) analysis after induction (time point 1, TP1) and consolidation therapy (TP2).20 SR patients were MRD-negative on both TP and HR patients had MRD levels of 10−3 or over at TP2. MRD-IR patients had positive MRD detection at either one or both time points but at a level of less than 10−3 at TP2. Patients with prednisone poor-response (PR; ≥1000 leukemic blood blasts/μL on treatment Day 8) or induction failure (≥5% leukemic blasts in the bone marrow, BM) or positivity for chromosomal translocations t(9;22)(q34;q11) or t(4;11)(q21;q23) or their molecular equivalents (BCR/ABL1 or MLL/AF4 rearrangement) were stratified into the HR group, independent of MRD.
Consecutively enrolled patients from the ALL-BFM 2000 study population with sufficient spare leukemic DNA available were included in our present study (Online Supplementary Table S1). BM or peripheral blood specimens had to contain more than 80% blasts, as assessed morphologically before gradient centrifugation.
Multiplex ligation-dependent probe amplification (MLPA) analysis
Recently, it was shown that MLPA is ideal for rapid high-throughput testing of large cohorts with a view to establish incidence and prognostic significance of certain gene aberrations.23 MLPA analysis was performed using the MLPA SALSA kit P335-A3 ALL-IKZF1 (MRC-Holland, Amsterdam, The Netherlands; www.mlpa.com) according to the manufacturer’s protocol. The assay includes probes for each of the eight exons of the IKZF1 gene and is able to detect deletions of the whole gene as well as all types of focal intragenic deletions. Selected exons of the genes EBF1, CDKN2A/B, PAX5, ETV6, BTG1, RB1 and the PAR1 region (approx. 230 kBp downstream of SHOX, CRLF2, CSF2RA and IL3RA) are also covered. The P2RY8-CRLF2 fusion can be identified through assessment of CSFRA and IL3RA deletions. Fragment analyses were performed on an Applied Biosystems 3730 DNA Analyzer (Applied Biosystems, Carlsbad, CA, USA) and data analyzed using Peak Scanner v1.0 and Coffalyser v9.4 software. Relative copy number was calculated after intra-sample normalization against control fragments and inter-sample normalization against control samples (healthy blood donor DNA). A ratio of 1±0.3 represents a normal copy number of 2, ratios of less than 0.7 and less than 0.3 represent heterozygous and homozyous deletions, respectively, while ratios of more than 1.3 indicate amplifications. Ratios for all fragments were visually inspected for plausibility and outliers included/excluded where appropriate. In a separate cohort of 25 patients (23 with IKZF1 deletion), we compared the results from Affymetrix SNP 6.0 arrays with MLPA kit P335 (Online Supplementary Figure S1). All 23 deletions that were known from SNP 6.0 arrays were also detected by MLPA, in 19 cases with exact overlap concerning the deleted exons. In 3 cases, not all exons were called correctly by MLPA, probably due to subclonality of the deletions. In one additional case, the deletion that was found in exon 3 by MLPA was detected in intron 3 on the SNP 6.0 array due to the location of SNP markers on the array. Comparison of the data obtained by the MLPA kit P335-A3 and the MLPA kit P202-A1 could be undertaken in 78 out of the 84 cases with IKZF1 deletions and only in one case was the deletion not detected using the MLPA kit P202, due to subclonality. Visual inspection of the results did not allow reliable detection of the lesion in P202 due to a higher background noise. (Online Supplementary Figure S2).
Statistical analysis
Event-free survival (EFS) was calculated from the date of diagnosis to last follow up or to the first event (no complete remission [CR] as event on Day 0, relapse, secondary malignancy, or death of any cause). Overall survival (OS) was calculated from the date of diagnosis to date of death by any cause. Rates were calculated according to Kaplan-Meier and compared by log rank test. Cumulative incidence of relapse (CIR) functions were constructed by the method of Kalbfleisch and Prentice and compared by the Gray test. Cox’s regression was used to calculate the hazard ratio for an event mediated by IKZF1 deletions. Proportional differences between patient groups were analyzed by χ2 or Fisher’s exact tests. Statistical analyses were carried out using the SAS statistical program (Version 9.1, Cary, NC, USA) and two-sided P values below 0.05 were considered statistically significant.
Results and Discussion
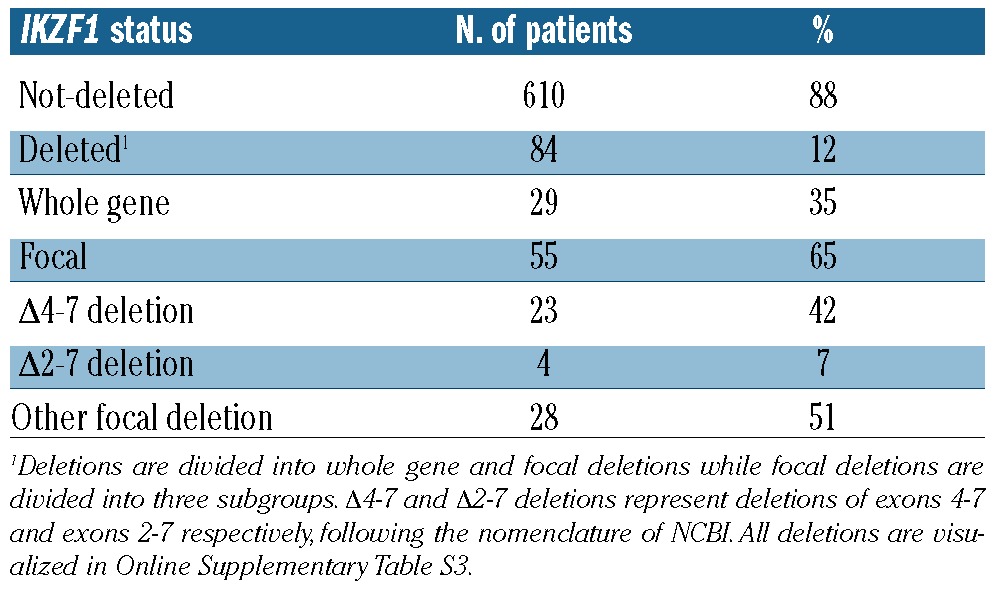
Genetic aberrations in IKZF1 were screened in diagnostic specimens of 694 ALL patients and IKZF1 deletions were detected in 84 out of 694 samples (12%) (Table 1). This frequency is within the range of abundances reported in other previously reported cohorts.7,9,13 Twenty-nine of these deletions covered the whole gene (35%), while 55 were focal deletions (65%). As described previously, focal lesions detected were mainly Δ4–7 (23 cases, 42%) and Δ2–7 (4 cases, 7%) deletions (Table 1 and Online Supplementary Figure S2).6,8,9,14,23 Δ4–7 and Δ2–7 deletions represent deletions of exons 4–7 and exons 2–7, respectively. All deletions are visualized in Online Supplementary Figure S2.
Table 1.
MLPA analysis of IKZF1 deletions in 694 patients with pediatric ALL.
Comparing leukemic and clinical characteristics of patients with and without IKZF1 deletion, no significant differences were observed concerning gender, age or presence of an MLL/AF4 rearrangement (Table 2). There was a positive association of IKZF1 deletion with higher white blood cell counts (WBC) at diagnosis (P=0.01), pB-ALL immunophenotype (P=0.01), positivity for a BCR/ABL rearrangement (P=0.03), as well as negativity for an ETV6/RUNX1 rearrangement (P<0.01). Of interest, only 5 out of 15 BCR/ABL1-positive cases harbored a deletion, which contrasts with previously published data describing the presence of IKZF1 deletions in approximately 80% of BCR/ABL1-positive ALL.5,6,8
Table 2.
Patients’ characteristics and response to treatment according to IKZF1 deletion status in 694 pediatric patients with ALL.
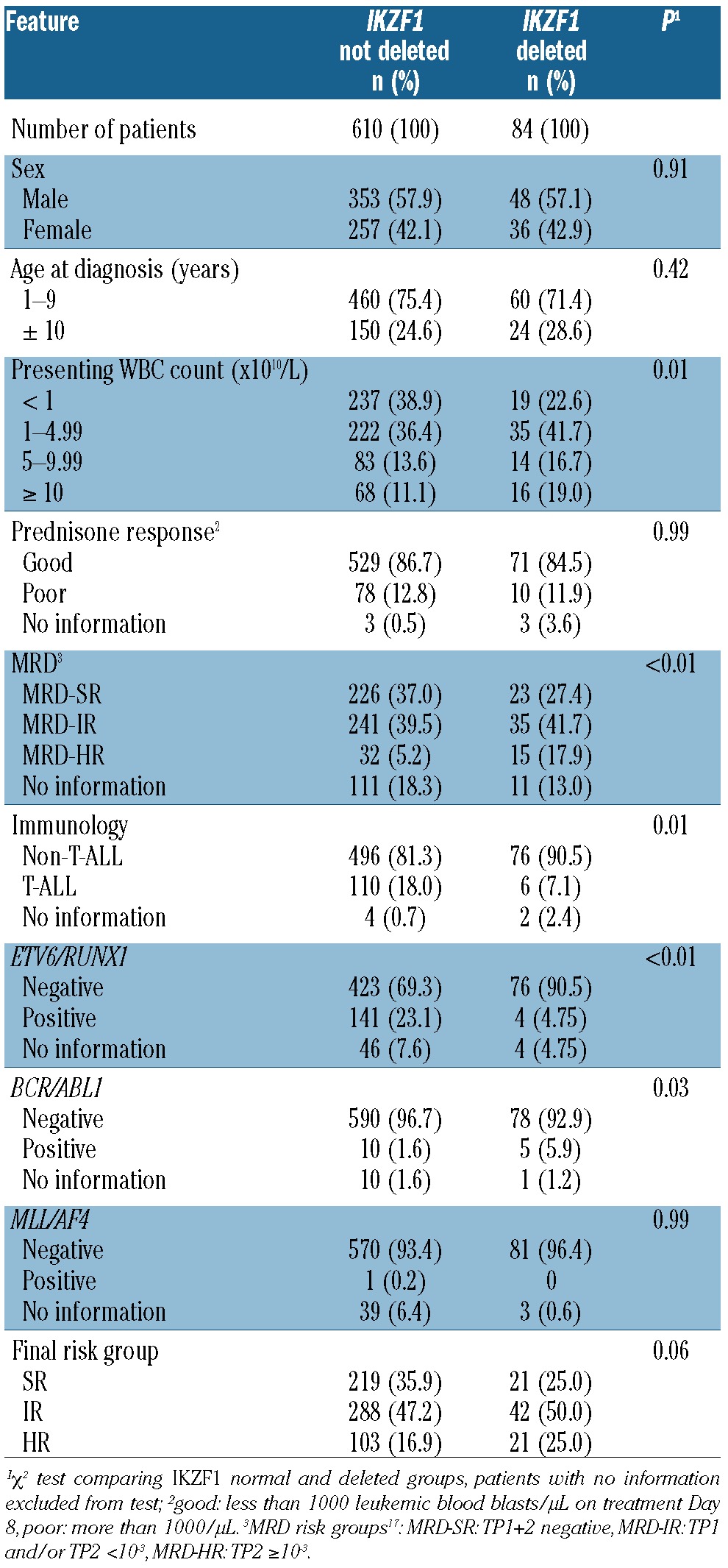
Most studies published so far focused on pB-ALL, and we also see a significant association of IKZF1 deletions with the pB-ALL phenotype. However, our cohort was made up of a total of 116 T-ALL patients, 6 of whom showed an IKZF1 deletion (5.2%). Out of the 6 T-ALL IKZF1-deleted patients, one was treated in the SR group while the others were HR patients. The SR patient is in CR, as are 2 of the HR patients, while the other 3 died (only one after a relapse).
Whereas no significant association of IKZF1 status with PR was observed, the presence of IKZF1 deletions was significantly more frequent in MRD-HR patients as compared to MRD-IR and MRD-SR patients (P<0.01). Five-year EFS was significantly lower in patients with an IKZF1 deletion compared to those without (0.69±0.05 vs. 0.85±0.01; P<0.0001) (Figure 1A). This difference was mainly attributable to a significantly higher CIR in IKZF1-deleted patients (0.21±0.04 vs. 0.10±0.01; P=0.001) (Figure 1B). This effect was most pronounced in the IR group, where the 5-year EFS was 0.71±0.07 in IKZF1-deleted patients compared to 0.84±0.02 in those without (P=0.008). The corresponding CIR was 0.26±0.07 and 0.10±0.02, respectively (P=0.0002) (Figures 1D and E). Fifty percent of all events and 13 of 19 relapses (68%) occurred in the IR group. No significant differences in EFS were seen in SR patients (deletion-positive vs. negative patients: 5-year EFS 0.85±0.08 vs. 0.92±0.02, P=0.42; CIR 0.08±0.02 vs. 0.05±0.05, P=0.54). While in HR-patients, EFS was 0.46±0.11 in the IKZF1-deleted versus 0.69±0.05 in the non-deleted group (P=0.03), there was no significant difference in CIR (0.25±0.10 vs. 0.15±0.04, P=0.28).
Figure 1.

Treatment outcome of patients with pediatric ALL comparing patients with and without IKZF1 deletions. Kaplan-Meier estimates for the whole cohort of 694 patients: (A) event-free survival (EFS) at 5 years, (B) cumulative incidence of relapse (CIR) at 5 years, and (C) overall survival (OS) at 5 years. For the intermediate risk group: (D) EFS, (E) CIR, and (F) OS.
Five-year OS was also significantly reduced in patients with IKZF1 deletions compared to patients without (0.82±0.04 vs. 0.92±0.01, P=0.003). The differences were, however, not significant when analyzing the data according to the current risk groups: (SR: deletion-positive vs. negative patients: 5-year OS 0.99±0.01 vs. 1.00, P=0.52; IR: 0.86±0.05 vs. 0.93±0.01, P=0.09; HR: 0.56±0.11 vs. 0.75±0.04, P=0.06). This suggests that patients with IKZF1 deletions who subsequently relapse are to a certain extent still treatment sensitive while in relapse.
In a Cox’s regression analysis considering the additional variables gender, initial WBC, MRD, and presence of the MLL/AF4, BCR/ABL1 and ETV6/RUNX1 rearrangement, IKZF1 deletions provided independent prognostic information (hazard ratio (HR) for an event 2.28, 95% confidence interval, CI: 1.44–3.60; P<0.001, Online Supplementary Table S2). IKZF1 deletions have been described to be associated with rearrangements of CRLF2 and, recently, we have shown that the P2RY8-CRLF2 rearrangement is associated with a poor outcome in patients treated according to the ALL-BFM 2000 protocol.17 In the study presented here, we confirmed a significantly higher number of IKZF1 deletions in patients positive for the P2RY8-CRLF2 rearrangement (13.1%) in comparison to those negative (2.6%; P<0.001). To explore whether IKZF1 has prognostic relevance independent of CRLF2 status, we first excluded CRLF2-rearranged patients from the multivariate analysis accounting for the strong association of the two factors (IKZF1 deletion and P2RY8-CRLF2 rearrangement), and the resulting co-linearity in the model. In this analysis, IKZF1 deletions still provided independent prognostic information (HR for an event 1.94; 95% CI: 1.19–3.16; P=0.008). Cox’s regression analysis including both factors resulted in a Hazard Ratio of 2.08 (95% CI: 1.32–3.28, P=0.002) for IKZF1-deletions and a hazard ratio of 2.04 (95% CI: 0.94–4.41, P=0.07) for P2RY8-CRLF2 (Online Supplementary Tables S3 and S4).
Comparing clinical and biological characteristics of patients with whole and focal gene deletions, no significant differences for gender, WBC, immunophenotype, involvement of the central nervous system (CNS), presence of BCR/ABL1, MLL/AF4 or ETV6/RUNX1 rearrangements, PR, MRD and final risk stratification were observed (data not shown). Patients with focal deletions were significantly older compared to patients with whole gene deletions (>10 years: 38% vs. 10%; P=0.01). There were no significant differences in 5-year EFS or CIR either when comparing whole and focal deletions or when comparing the different types of IKZF1 deletions (data not shown).
IKZF1 deletions were repeatedly reported to confer an increased risk of relapse and poor outcome in selected cohorts6,9 and recently in an unselected cohort of 131 pB-ALL cases.12,13 Here, we present data on the prognostic relevance of IKZF1 in a large set of nearly 700 patients uniformly treated on the MRD-based ALL-BFM 2000 protocol and were able to show that IKZF1 status exerts additive value as a prognostic factor, especially in the IR group in which still the majority of relapses occur. Therefore, the assessment of IKZF1 status may contribute to a molecular-based stratification algorithm aiming at improving outcome for children suffering from ALL. However, more work has to be done to clarify the molecular differences between IKZF1-deleted leukemias of patients who relapse and those who don’t. From our perspective, this is a prerequisite for an application of the IKZF1 status in clinical decision-making.
Supplementary Material
Acknowledgments
The authors would like to thank Birthe Fedders, Kristina Wulf and Christian Bretscher from the ALL-BFM laboratory and the members of the sequencing facility at the Institute for Clinical Molecular Biology at the University Hospital Schleswig-Holstein, Campus Kiel, for their excellent technical assistance.
Footnotes
Funding
Supported by the Federal Ministry of Education and Research (BMBF; NGFN project number 01GS0442), the Deutsche Krebshilfe and the Madeleine Schickedanz Kinderkrebs-Stiftung.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Georgopoulos K, Bigby M, Wang JH, Molnar A, Wu P, Winandy S, et al. The Ikaros gene is required for the development of all lymphoid lineages. Cell. 1994;79(1):143–56 [DOI] [PubMed] [Google Scholar]
- 2.Georgopoulos K. Haematopoietic cell-fate decisions, chromatin regulation and ikaros. Nat Rev Immunol. 2002;2(3):162–74 [DOI] [PubMed] [Google Scholar]
- 3.Molnar A, Wu P, Largespada DA, Vortkamp A, Scherer S, Copeland NG, et al. The Ikaros gene encodes a family of lymphocyte-restricted zinc finger DNA binding proteins, highly conserved in human and mouse. J Immunol. 1996;156(2):585–92 [PubMed] [Google Scholar]
- 4.Harvey RC, Mullighan CG, Wang XF, Dobbin KK, Davidson GS, Bedrick EJ, et al. Identification of novel cluster groups in pediatric high-risk B-precursor acute lymphoblastic leukemia with gene expression profiling: correlation with genome-wide DNA copy number alterations, clinical characteristics, and outcome. Blood. 2010;116(23):4874–84 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Iacobucci I, Storlazzi CT, Cilloni D, Lonetti A, Ottaviani E, Soverini S, et al. Identification and molecular characterization of recurrent genomic deletions on 7p12 in the IKZF1 gene in a large cohort of BCR-ABL1-positive acute lymphoblastic leukemia patients: on behalf of Gruppo Italiano Malattie Ematologiche dell’Adulto Acute Leukemia Working Party (GIMEMAALWP). Blood. 2009;114(10):2159–67 Erratum in: Blood. 2010;116(12):2196 [DOI] [PubMed] [Google Scholar]
- 6.Martinelli G, Iacobucci I, Storlazzi CT, Vignetti M, Paoloni F, Cilloni D, et al. IKZF1 (Ikaros) deletions in BCR-ABL1-positive acute lymphoblastic leukemia are associated with short disease-free survival and high rate of cumulative incidence of relapse: A GIMEMA AL WP report. J Clin Oncol. 2009;27(31):5202–7 [DOI] [PubMed] [Google Scholar]
- 7.Mullighan CG, Goorha S, Radtke I, Miller CB, Coustan-Smith E, Dalton JD, et al. Genome-wide analysis of genetic alterations in acute lymphoblastic leukaemia. Nature. 2007;446(7137):758–64 [DOI] [PubMed] [Google Scholar]
- 8.Mullighan CG, Miller CB, Radtke I, Phillips LA, Dalton J, Ma J, et al. BCR-ABL1 lymphoblastic leukaemia is characterized by the deletion of Ikaros. Nature. 2008;453(7191):110–5 [DOI] [PubMed] [Google Scholar]
- 9.Mullighan CG, Su XP, Zhang JH, Radtke I, Phillips LAA, Miller CB, et al. Deletion of IKZF1 and prognosis in acute lymphoblastic leukemia. N Engl J Med. 2009;360(5):470–80 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yang YL, Hung CC, Chen JS, Lin KH, Jou ST, Hsiao CC, et al. IKZF1 deletions predict a poor prognosis in children with B-cell progenitor acute lymphoblastic leukemia: a multicenter analysis in Taiwan. Cancer Sci. 2011; 10.1111/j.1349-7006.2011.02031.x [DOI] [PMC free article] [PubMed]
- 11.Den Boer ML, van Slegtenhorst M, De Menezes RX, Cheok MH, Buijs-Gladdines J, Peters S, et al. A subtype of childhood acute lymphoblastic leukaemia with poor treatment outcome: a genome-wide classification study. Lancet Oncol. 2009;10(2):125–34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kuiper RP, Waanders E, van der Velden VHJ, van Reijmersdal SV, Venkatachalam R, Scheijen B, et al. IKZF1 deletions predict relapse in uniformly treated pediatric precursor B-ALL. Leukemia. 2010;24(7):1258–64 [DOI] [PubMed] [Google Scholar]
- 13.Waanders E, van der Velden VHJ, van der Schoot CE, van Leeuwen FN, van Reijmersdal SV, de Haas V, Veerman AJ, Geurts van Kessel A, Hoogerbrugge PM, Kuiper RP, van Dongen JJM.Integrated use of minimal residual disease classification and IKZF1 alteration status accurately predicts 79% of relapses in pediatric acute lymphoblastic leukemia. Leukemia. 2011;25(2):254–8 [DOI] [PubMed] [Google Scholar]
- 14.Mullighan CG, Zhang JH, Harvey RC, Collins-Underwood JR, Schulman BA, Phillips LA, et al. JAK mutations in high-risk childhood acute lymphoblastic leukemia. Proc Natl Acad Sci USA. 2009;106(23):9414–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Russell LJ, Capasso M, Vater I, Akasaka T, Bernard OA, Calasanz MJ, et al. Deregulated expression of cytokine receptor gene, CRLF2, is involved in lymphoid transformation in B-cell precursor acute lymphoblastic leukemia. Blood. 2009;114(13):2688–98 [DOI] [PubMed] [Google Scholar]
- 16.Mullighan CG, Collins-Underwood JR, Phillips LAA, Loudin MG, Liu W, Zhang J. Rearrangement of CRLF2 in B-progenitor-and Down syndrome-associated acute lymphoblastic leukemia. Nature Genetics. 2009;41(11):1243–6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cario G, Zimmermann M, Romey R, Gesk S, Vater I, Harbott J, et al. Presence of the P2RY8-CRLF2 rearrangement is associated with a poor prognosis in non-high-risk precursor B-cell acute lymphoblastic leukemia in children treated according to the ALL-BFM 2000 protocol. Blood. 2010;115(26):5393–7 [DOI] [PubMed] [Google Scholar]
- 18.Harvey CR, Mullighan CG, Chen I-M, Wharton W, Mikhail FM, Carroll AJ, et al. Rearrangement of CRLF2 is associated with mutation of JAK kinases, alteration of IKZF1, Hispani/Latino ethnicicity, and a poor outcome in pediatric B-progenitor acute lymphoblastic leukemia. Blood. 2010;115(26):5312–21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ensor HM, Schwab C, Russell LJ, Richards SM, Morrison H, Masic D, et al. Demographical, clinical, and outcome features of children with acute lymphoblastic leukemia and CRLF2 deregulation: results from the MRC ALL97 clinical trial. Blood. 2011;117(7):2129–36 [DOI] [PubMed] [Google Scholar]
- 20.Flohr T, Schrauder A, Cazzaniga G, Panzer-Grumayer R, van der Velden V, Fischer S, et al. Minimal residual disease-directed risk stratification using real-time quantitative PCR analysis of immunoglobulin and T-cell receptor gene rearrangements in the international multicenter trial AIEOP-BFM ALL 2000 for childhood acute lymphoblastic leukemia. Leukemia. 2008;22(4):771–82 [DOI] [PubMed] [Google Scholar]
- 21.Stanulla M, Schaeffeler E, Flohr T, Cario G, Schrauder A, Zimmermann M, et al. Thiopurine methyltransferase (TPMT) genotype and early treatment response to mercaptopurine in childhood acute lymphoblastic leukemia. JAMA. 2005;293(12):1485–9 [DOI] [PubMed] [Google Scholar]
- 22.Conter V, Bartram CR, Valsecchi MG, Schrauder A, Panzer-Grumayer R, Moricke A, et al. Molecular response to treatment redefines all prognostic factors in children and adolescents with B-cell precursor acute lymphoblastic leukemia: results in 3184 patients of the AIEOP-BFM ALL 2000 study. Blood. 2010;115(16):3206–14 [DOI] [PubMed] [Google Scholar]
- 23.Schwab CJ, Jones LR, Morrison H, Ryan SL, Yigittop H, Schouten JP, et al. Evaluation of multiplex ligation-dependent probe amplification as a method for the detection of copy number abnormalities in B-cell precursor acute lymphoblastic leukemia. Genes Chromosomes Cancer. 2010;49(12):1104–13 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.