

Abstract
OBJECTIVE
Metabolic syndrome is a multiplex disorder and puts patients on the road to type 2 diabetes and atherosclerotic cardiovascular diseases. However, a surrogate biomarker in plasma or urine in fully reflecting features of metabolic syndrome has not been explored.
RESEARCH DESIGN AND METHODS
Urine metabolomics has potential utility in metabolic profiling because urine metabolites analysis reflects global outflux of metabolic change. Accordingly, we collected data on subjects (n = 99) with overweight, dyslipidemia, hypertension or impaired glucose tolerance and took a metabolomics approach to analyze the metabolites of urine revealed in metabolic syndrome by high-performance liquid chromatography–time-of-flight mass spectrometry and elicit potential biomarkers to picture metabolic syndrome.
RESULTS
Our results revealed that the urine nicotinuric acid value of subjects with diabetes (HbA1c ≥6.5% or those receiving diabetes medications) (n = 25) was higher than subjects without diabetes (n = 37) (221 ± 31 vs. 152 ± 13 × 103 mAU, P = 0.0268). Moreover, urinary nicotinuric acid level was positively correlated with body mass index, blood pressure, total cholesterol, low-density lipoprotein cholesterol, triacylglycerol and high sensitivity C-reactive protein, but negatively correlated with high-density lipoprotein cholesterol.
CONCLUSIONS
This is the first study, to our knowledge, to propose that nicotinuric acid represents an important pathogenic mechanism in process from metabolic syndrome to diabetes and atherosclerotic cardiovascular disease.
Metabolic syndrome is a multifaceted disorder and considered to be a major cause of type 2 diabetes and atherosclerotic cardiovascular diseases. Although urine metabolomics has potential utility in metabolic profiling because urine metabolites reveal a global outflux of metabolic change, a surrogate biomarker in urine that fully reflects features of metabolic syndrome has not been explored. The aim of this study was to isolate a potential biomarker of metabolic syndrome through analysis of urine metabolites in subjects with features of metabolic syndrome.
RESEARCH DESIGN AND METHODS
Urine samples were obtained after overnight fasting from 99 unselected subjects (66 women, mean age 69 ± 13 years) who visited the hospital for a health checkup. Chromatographic separation of urine supernatant was performed on a reversed-phase Acquity UPLC BEH C18 column (Waters Corporation, Milford, MA) using an Agilent 1200 Series Rapid Resolution LC (liquid chromatography) system (Agilent Technologies, Santa Clara, CA). The LC system was coupled to an Agilent 6510 Q-TOF MS (mass spectrometer) equipped with an electrospray ionization source. Subsequent mass spectrometric analysis has been previously described (1).
Agilent GeneSpring MS version 1.2 software was used to analyze datasets in numerical data matrices. Principal components analysis was applied for differentiation of subjects with various pathophysiological features. The relative concentrations of metabolites in separate groups were compared by ANOVA with Tukey honestly significant difference correction using SPSS 13.0 (International Business Machines Corporation, Chicago, IL) software. Accurate masses of features showing significant differences between groups were searched against the METLIN Metabolite Database, the Human Metabolome Database, and the Kyoto Encyclopedia of Genes and Genomes database.
For confirmation of metabolite identity, samples were run under chromatographic conditions similar to those of profiling studies. Mass spectrometric analyses were performed using the Agilent 6510 Q-TOF MS under similar conditions.
RESULTS
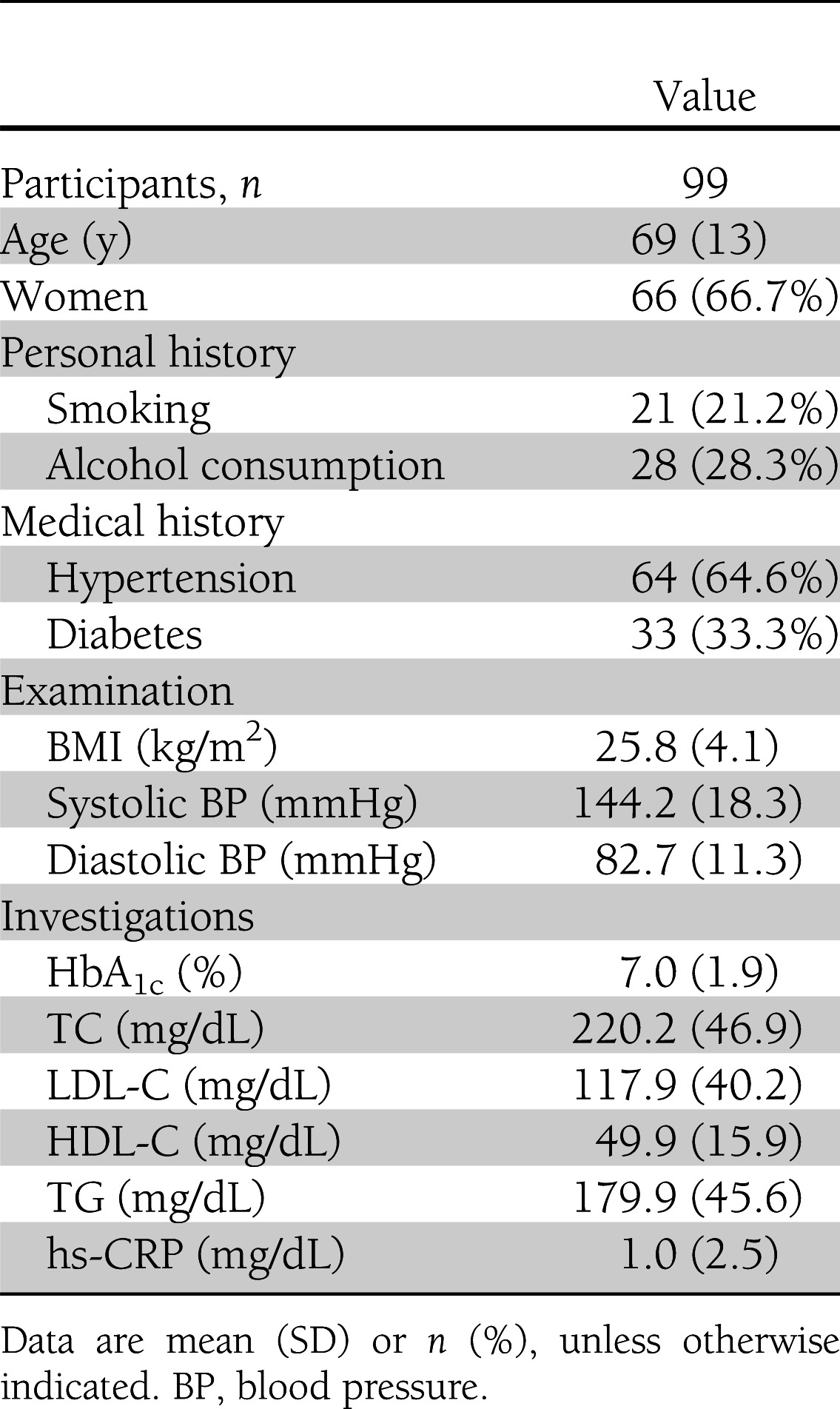
As shown in Table 1, the subjects’ average BMI, blood glucose level, blood pressure, and lipid levels were just slightly above the standard values, reflecting the typical characteristics of patients with metabolic syndrome. Through urinary data analysis, metabolites were grouped according to BMI, hypertension, diabetes, total cholesterol (TC), and triacylglycerol (TG) indexes. We observed that many metabolites (e.g., nicotinuric acid, hypoxanthine, tiglylcarnitine, 1-methylhistidine) were the basis for clustering of certain indexes (BMI, TC, TG and blood pressure before eating, and having or not having diabetes), but only nicotinuric acid clustered all indexes.
Table 1.
Baseline clinical and biochemical characteristics of subjects
The level of urine nicotinuric acid in subjects who were overweight (BMI ≥ 24 kg/m2) (n = 40) was higher than in those who were not (BMI < 24 kg/m2) (n = 23) (221 ± 23 vs. 144 ± 18 × 103 milliabsorbance units [mAU], P = 0.0265) and was higher in subjects with high blood pressure (≥140/90 mmHg) (n = 40) than in normotensive subjects (n = 28) (238 ± 28 vs. 154 ± 19 × 103 mAU, P = 0.0269). In subjects with diabetes (glycated hemoglobin [HbA1c] ≥6.5% or receiving diabetes medication) (n = 25), urine nicotinuric acid level was higher than in those without diabetes (n = 37) (221 ± 31 vs. 152 ± 13 × 103 mAU, P = 0.0268), and in subjects with high levels of TG (≥150 mg/dL) (n = 44), it was higher than in those with normal levels of TG (<150 mg/dL) (n = 21) (218 ± 20 vs. 136 ± 22 × 103 mAU, P = 0.0147). In subjects with high levels of LDL cholesterol (LDL-C) (≥100 mg/dL) (n = 37), urine nicotinuric acid values were higher than in those with normal levels of LDL-C (<100 mg/dL) (n = 18) (239 ± 26 vs. 158 ± 20 × 103 mAU, P = 0.0426), and it was higher in subjects with high TC levels (≥200 mg/dL) than in those with normal levels (data not shown). On the other hand, urine nicotinuric acid values in subjects with low levels of HDL cholesterol (HDL-C) (<40 mg/dL) (n = 14) were higher than in those with normal levels of HDL-C (≥40 mg/dL) (n = 36) (234 ± 23 vs. 167 ± 14 × 103 mAU, P = 0.0134).
Moreover, we selected high-sensitivity C-reactive protein (hs-CRP) as the index for assessing cardiovascular disease risk. Urine nicotinuric acid values in subjects with high levels of hs-CRP (≥0.3 mg/dL) (n = 23) were higher than in those with low levels of hs-CRP (<0.3 mg/dL) (n = 32) (252 ± 37 vs. 170 ± 15 × 103 mAU, P = 0.0296).
CONCLUSIONS
To our knowledge, this report is the first to show that urinary nicotinuric acid level is positively correlated with BMI, blood pressure, and plasma HbA1c, TC, LDL-C, TG, and hs-CRP levels but negatively correlated with HDL-C level. Nicotinuric acid is the major catabolic product of nicotinic acid and regarded as a good index for assessing nicotinic acid biotransformation in the liver (2). The structure of nicotinuric acid is a type of acylglycine, which participates in various coenzyme tasks, including glycolysis, gluconeogenesis, the citric acid cycle, and oxidation, for all tissues as well as in forming long-chain fatty acids (3). Previous studies indicated that acylglycine in urine reflects an accumulating condition of acyl-CoA ester in mitochondria (4). Moreover, long-chain acyl-CoA esters have been addressed as an index for muscle lipid metabolism and negatively correlated to the effects of insulin (5).
Nicotinic acid is transformed from tryptophan and mainly used to produce two coenzymes, NAD+ and NADP+ (6). A recent study revealed that 5-hydroxyindole-3-acetic acid (a derivative end product of serotonin converted from tryptophan) concentrations are high in subjects with metabolic syndrome (7). Mechanistically, NADP+ and NADPH are the coenzymes for the oxidation-reduction reactions of fatty acid synthesis (8,9). Nicotinic acid has been proven to effectively reduce TG and LDL-C levels and increase HDL-C levels, but it increases the possibility of insulin resistance (10,11). In this respect, nicotinuric acid in urine reasonably shows the changes of lipid metabolism and insulin resistance, which comprise the core of the pathological mechanism of metabolic syndrome.
Recent studies showed that the concentration of plasma choline is related to cardiovascular disease risk (12,13). Betaine and glycine are part of the metabolic pathways for choline (14). In this regard, the metabolites of nicotinic acid (nicotinuric acid [N-nicotinoyl-glycine] and trigonelline [betaine nicotinate]) could also reflect part of the metabolism of choline (Supplementary Fig. 1).
In conclusion, this study proposes that nicotinuric acid could be used to represent a potential pathogenic mechanism of metabolic syndrome. However, there are two limitations that need to be addressed. First, the subjects did not fully meet the diagnostic criteria for metabolic syndrome, although comparative parameters included in this study are much wider than the current diagnostic criteria for metabolic syndrome. Second, the presence of atherosclerotic cardiovascular disease was not confirmed in the subjects but only speculated by serum hs-CRP level. Regardless, these findings bring a new perspective not only to the lipid metabolism and insulin resistance properties of nicotinuric acid, but also to the balance of NAD+/NADH and NADP+/NADPH, and deserve further exploration.
Acknowledgments
This study was supported by a National Science Council grant (NSC98-2314-B-182-009-MY3), by Chang Gung University (EMRPD1A0851), and by Saint Mary’s Hospital Luodong. The funder played no role in the conduct of the study, collection of data, management of the study, analysis of data, interpretation of data, or preparation of the manuscript.
No potential conflicts of interest relevant to this article were reported.
C.-F.H. acquired, analyzed, and interpreted data and wrote, critically revised, and approved the manuscript. M.-L.C. performed the statistical analysis and critically revised and approved the manuscript. C.-M.F. provided technical support and critically revised and approved the manuscript. C.-Y.H. performed the statistical analysis, provided technical support, and critically revised and approved the manuscript. M.-S.S. obtained funding; conceived of, directed, and supervised the study; acquired, analyzed, and interpreted the data; and critically revised and approved the manuscript. C.-F.H. and M.-S.S. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
The authors thank the staff of the Division of Family Medicine, Saint Mary’s Hospital Luodong and the Department of Biomedical Sciences, Chang Gung University, for their clinical support of this study.
Footnotes
This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc12-1067/-/DC1.
References
- 1.Chen KH, Cheng ML, Jing YH, Chiu DT, Shiao MS, Chen JK. Resveratrol ameliorates metabolic disorders and muscle wasting in streptozotocin-induced diabetic rats. Am J Physiol Endocrinol Metab 2011;301:E853–E863 [DOI] [PubMed] [Google Scholar]
- 2.Inamadugu JK, Damaramadugu R, Mullangi R, Ponneri V. Simultaneous determination of niacin and its metabolites—nicotinamide, nicotinuric acid and N-methyl-2-pyridone-5-carboxamide—in human plasma by LC-MS/MS and its application to a human pharmacokinetic study. Biomed Chromatogr 2010;24:1059–1074 [DOI] [PubMed] [Google Scholar]
- 3.Jones KM. The mechanism of nicotinuric acid synthesis. Biochem J 1959;73:714–719 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rinaldo P, Schmidt-Sommerfeld E, Posca AP, Heales SJ, Woolf DA, Leonard JV. Effect of treatment with glycine and L-carnitine in medium-chain acyl-coenzyme A dehydrogenase deficiency. J Pediatr 1993;122:580–584 [DOI] [PubMed] [Google Scholar]
- 5.Ellis BA, Poynten A, Lowy AJ, et al. Long-chain acyl-CoA esters as indicators of lipid metabolism and insulin sensitivity in rat and human muscle. Am J Physiol Endocrinol Metab 2000;279:E554–E560 [DOI] [PubMed] [Google Scholar]
- 6.Zhu J, Ganton MD, Kerr MA, Workentin MS. Chemical modification of monolayer-protected gold nanoparticles using hyperbaric conditions. J Am Chem Soc 2007;129:4904–4905 [DOI] [PubMed] [Google Scholar]
- 7.Fukui M, Tanaka M, Toda H, et al. High plasma 5-hydroxyindole-3-acetic acid concentrations in subjects with metabolic syndrome. Diabetes Care 2012;35:163–167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Seubert W, Podack ER. Mechanisms and physiological roles of fatty acid chain elongation in microsomes and mitochondria. Mol Cell Biochem 1973;1:29–40 [DOI] [PubMed] [Google Scholar]
- 9.Rawlings BJ. Biosynthesis of fatty acids and related metabolites. Nat Prod Rep 1998;15:275–308 [DOI] [PubMed] [Google Scholar]
- 10.Villines TC, Kim AS, Gore RS, Taylor AJ. Niacin: the evidence, clinical use, and future directions. Curr Atheroscler Rep 2012;14:49–59 [DOI] [PubMed] [Google Scholar]
- 11.Karpe F, Frayn KN. The nicotinic acid receptor—a new mechanism for an old drug. Lancet 2004;363:1892–1894 [DOI] [PubMed] [Google Scholar]
- 12.Wang Z, Klipfell E, Bennett BJ, et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011;472:57–63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Danne O, Lueders C, Storm C, Frei U, Möckel M. Whole blood choline and plasma choline in acute coronary syndromes: prognostic and pathophysiological implications. Clin Chim Acta 2007;383:103–109 [DOI] [PubMed] [Google Scholar]
- 14.Landfald B, Strøm AR. Choline-glycine betaine pathway confers a high level of osmotic tolerance in Escherichia coli. J Bacteriol 1986;165:849–855 [DOI] [PMC free article] [PubMed] [Google Scholar]