

Abstract
Children's posture has been of growing concern due to observations that it seems to be impaired compared to previous generations. So far there is no reference data for spinal posture and pelvic position in healthy children available. Purpose of this pilot study was to determine rasterstereographic posture values in children during their second growth phase. Three hundred and forty-five pupils were measured with a rasterstereographic device in a neutral standing position with hanging arms. To further analyse for changes in spinal posture during growth, the children were divided into 12-month age clusters. A mean kyphotic angle of 47.1°±7.5 and a mean lordotic angle of 42.1°±9.9 were measured. Trunk imbalance in girls (5.85 mm±0.74) and boys (7.48 mm± 0.83) varied only little between the age groups, with boys showing slightly higher values than girls. The trunk inclination did not show any significant differences between the age groups in boys or girls. Girls' inclination was 2.53°±1.96 with a tendency to decreasing angles by age, therefore slightly smaller compared to boys (2.98°±2.18). Lateral deviation (4.8 mm) and pelvic position (tilt: 2.75 mm; torsion: 1.53°; inclination: 19.8°±19.8) were comparable for all age groups and genders. This study provides the first systematic rasterstereographic analysis of spinal posture in children between 6 and 11 years. With the method of rasterstereography a reliable three-dimensional analysis of spinal posture and pelvic position is possible. Spinal posture and pelvic position does not change significantly with increasing age in this collective of children during the second growth phase.
Key words: rasterstereography, children, posture, spine, back pain, pelvic position.
Introduction
Correct upright posture is considered to be an important indicator of musculoskeletal health. Incorrect posture in turn is regarded as a possible factor for the development of cervical and back pain.1 In recent years, children's posture has been of growing concern to parents, teachers and medical professionals due to observations that it seems to be impaired compared to previous generations.2 Nevertheless the quantification and analysis of spinal posture and pelvic position in children has received only scant attention and the question of what is normal posture in children? still remains to be answered.3
This seems not surprising, as varying analysis techniques were often utilized to measure spinal posture. Early studies used e.g. external measuring devices such as the kyphometer or the inclinometer.4,5 Since 1970 the Moiré-phenomenon was commonly used to analyse the back surface. Until today this method has not been well established because of a lack of well-defined methodological procedures. Recent video based measuring devices produce more reliable and precise results, but most of them are rather time consuming or can only be operated by experts.6 Other automatic systems, e.g. 3D ultrasonic devices, need reflective markers to detect anatomical structures. Because of these problems radiological imaging is still the gold standard in the analysis of spinal posture and pelvic position. Due to the problem of radiation exposure, x-rays are not feasible for epidemiological questions or frequent measurements in routine diagnostics and long-term follow-ups.7 One method that has been used in clinical routine for many years and that has considerably evolved over time is rasterstereography.8,9
Purpose of this present pilot study was to measure and analyse the spinal posture and pelvic position in children between the age of 6 and 11 years. Further, we were interested in acquiring rasterstereographic reference data for future comparison with children that have spinal pathologies like e.g. scoliosis, back pain or Scheuermann's disease.
Materials and Methods
345 elementary school pupils (168 girls and 177 boys) between the age of 6 and 11 years were measured in this study. To further analyse for changes in spinal posture during the second growth phase, the children were divided into the following 12-month age-clusters: 6–7, 7–8, 8–9, 9–10, 10–11 years of age. All pupils were grouped according to their actual age on the day of the measurement as shown in Table 1. Parents of all subjects were informed about this study and gave their written consent as well as were given the option to quit participation of their children at any time. The institutional ethic committee approved the study protocol. Body-height and weight were measured and the body mass index (BMI) was calculated resulting in an individual percentile according to Kronmeyer-Hausschild.10 Since we were interested in reference data of healthy kids, children with back pain in the last year longer than three days, with a BMI >35 kg/m2, scoliosis with a Cobb angle >50° and a history of spine, pelvis or lower extremity fracture, were excluded from the study.
Table 1. Anthropometric data of the measured pupils separated by gender: the mean age, body mass index (BMI), weight, height, standard deviation (SD) and number of subjects in the selected age groups (N) are shown. Weight, height and the respective BMI increased by age as expected with an almost comparable trend in boys and girls. The increase in body height was significant, with a difference between the youngest and the oldest group in both sexes of approximately 20 cm.
| Sex | Age (years) | Mean age | SD | BMI | SD | Weight | SD | Height | SD | N. |
|---|---|---|---|---|---|---|---|---|---|---|
| Girls | 6–7 | 6.54 | 0.28 | 15.74 | 1.74 | 23.39 | 4.36 | 1.21 | 0.07 | 24 |
| 7–8 | 7.50 | 0.32 | 15.75 | 1.71 | 25.01 | 3.87 | 1.26 | 0.05 | 54 | |
| 8–9 | 8.49 | 0.27 | 16.90 | 2.84 | 29.89 | 6.38 | 1.33 | 0.05 | 40 | |
| 9–10 | 9.49 | 0.27 | 17.83 | 2.24 | 34.39 | 4.88 | 1.39 | 0.05 | 27 | |
| 10–11 | 10.43 | 0.31 | 17.89 | 3.26 | 35.77 | 6.90 | 1.41 | 0.06 | 23 | |
| Total girls | - | 8.32 | 1.27 | 16.65 | 2.50 | 28.92 | 6.91 | 1.31 | 0.09 | 168 |
| Boys | 6–7 | 6.70 | 0.26 | 15.81 | 1.79 | 24.52 | 3.94 | 1.24 | 0.05 | 23 |
| 7–8 | 7.47 | 0.22 | 16.68 | 2.27 | 27.04 | 5.24 | 1.27 | 0.05 | 40 | |
| 8–9 | 8.48 | 0.30 | 16.69 | 2.54 | 30.51 | 6.91 | 1.35 | 0.07 | 43 | |
| 9–10 | 9.44 | 0.30 | 17.50 | 2.70 | 34.12 | 7.30 | 1.39 | 0.07 | 45 | |
| 10–11 | 10.47 | 0.33 | 17.70 | 2.60 | 36.17 | 6.38 | 1.43 | 0.05 | 26 | |
| Total boys | - | 8.56 | 1.24 | 16.92 | 2.49 | 30.67 | 7.34 | 1.34 | 0.09 | 177 |
SD, standard devation; BMI, body mass index.
Spinal posture and pelvic position were measured with the rasterstereography system Formetric® (Diers International GmbH, Schlangenbad, Germany). Rasterstereography is a method for surface measuring, which was developed in the 1980s by Hierholzer and Drerup.8,11 Therefore, horizontal parallel light lines are projected onto the unclothed surface of the back by a slide projector. Next, a surface reconstruction of the back is performed by transforming the stripes and their corresponding curvature into a scatter plot. The acquired space coordinates are used to reconstruct the back surface according to convex, concave or saddle shaped areas (Figure 1). Then, a model of the spine can be calculated based on the specific convex shaped form of the spinous process of the vertebra prominence (VP) and the concavity of the lumbar dimples, which all are automatically detected by the system with a standard deviation of ±1 mm.9 Using this model, transverse and sagittal profiles, the spinous process line and several spinal angles and indices can be calculated. All measurements were performed with the children in a neutral upright standing position. The neutral zero standing position was defined as the spinal posture in the erect, with the arms hanging down laterally to the body, barefoot in a comfortable standing position with extended knees. Marking the position of the feet ensured reproducibility of the foot position. For the purpose of this study it is necessary to define certain terms regarding the parameters that were measured. The pelvic tilt is the amount of tilt in degrees or mm from the horizontal of a line between the two lumbar dimples DL (left dimple) to DR (right dimple). A positive value indicates that the right dimple is higher than the left and a negative value indicates that the left dimple is higher than the right. The pelvic torsion measured in degrees is the rotation of the surface normals of the two lumbar dimples (DL & DR). A positive pelvic torsion means that the right hipbone is oriented farther anterior than the left hipbone and a negative value signifies that the left hipbone is farther anterior than the right hipbone. Pelvic inclination is the mean vertical torsion of the two surface normals on the dimples, where a positive pelvic inclination signifies a mean vertical component upwards and a negative inclination a mean vertical component downwards. The lateral deviation is defined as the deviation of the spinal midline from the line between the VP to midpoint between DL & DR (DM) in the frontal plane. The kyphotic angle is the angle between the surface tangents on points VP and the calculated spinous process of the 12th thoracic vertebrae (T12) and the lordotic angle is the angle between the surface tangents on points T12 and DM. Trunk inclination was calculated as the distance in the sagittal plane between VP and the lumbar dimples (DM). A positive value was interpreted as an increase in inclination in an anterior direction, whereas a negative value represents a more upright or even hyper-extended standing position. The lateral distance between the VP and the DM is called the trunk imbalance. A positive value signifies a shift of the VP to the right and a negative value to the left.
Figure 1.
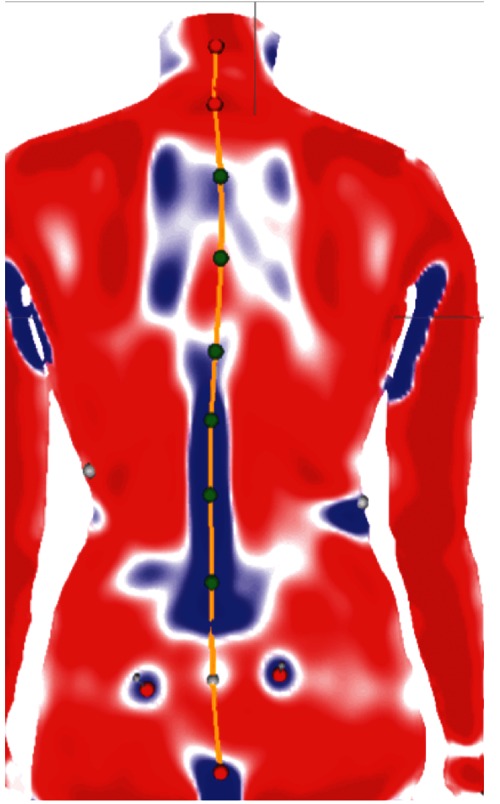
This figure shows a rasterstereographic measurement of a child. After the acquisition of the picture with a digital video camera, the image is then analysed by the computer, the anatomical landmarks are automatically detected, and transformed into a 3-D surface map of the back surface. The red colour on the back surface represents convex surface areas, while the blue colour stands for concave surface areas.
Data analysis
Statistical analysis was carried out using the Statistical Package for the Social Sciences, version 20.0 (SPSS, Inc, Chicago, IL, USA). Descriptive statistics represents mean values and standard deviation (SD) for the total population, as well as for the individual sexes and age groups. Differences between the sexes were tested using a paired t-test. A one factor ANOVA and a post-hoc Bonferroni test were used to calculate for differences.
Results
Children's anthropometric data as shown in Table 1 were within a normal range.10 Weight, height and BMI increased by age with an almost comparable trend in boys and girls (Figure 2). The increase in body height was significant (P<0.05), with a difference between the youngest and the oldest group in both sexes of approximately 20 cm. In contrast to the measured body height the measured trunk length increased non-significantly (P>0.05) from the youngest to the oldest group (girls 0.5 cm, boys 0.4 cm) as seen in Figure 2.
Figure 2.
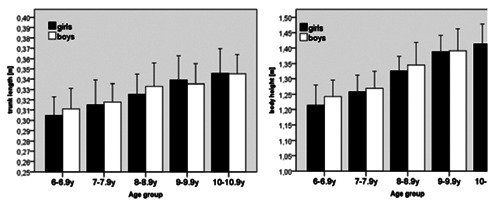
Mean and SD of the variables trunk length (left) and body height (right) across the age groups, separated by sex. In contrast to the measured body height, the calculated trunk length (distance between spinous process of the 7th vertebrae to the midpoint of the lumbar dimples), increased only slightly from the youngest to the oldest group (girls 0.5 cm, boys 0.4 cm).
Spinal posture
For all age groups a mean kyphotic angle of 47.1° (SD±7.5) was measured. The kyphotic angle did not show any significant changes (P>0.05) between the measured age groups. In girls, the respective angle was 47°, whereas in boys a small not significant increase (P>0.05) by age could be noticed from 44° in the youngest group to 48° in the oldest. There was no significant difference (P>0.05) between boys and girls (Figure 3).
Figure 3.
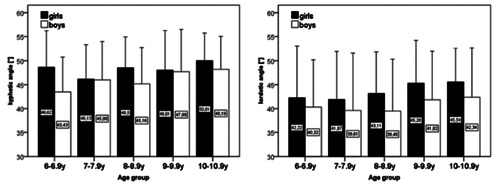
The kyphotic angle did not show any significant changes between the measured age groups. For the lordotic angle, we observed a small increase according to age, that was more pronounced in girls than in boys. However, no significant differences were found between the age groups or genders.
The lordotic angle was determined in our study with a mean value of 42.1° (SD±9.9). For the lordotic angle, we observed a small increase according to age that was more pronounced in girls than in boys. However, no significant differences (P>0.05) were found between the age groups or genders (Figure 3). Trunk imbalance in girls (5.85 mm ±0.74) and boys (7.48 mm ±0.83) varied only little, with boys showing slightly higher values than girls (Table 2). Remarkably, the youngest boys presented the highest deviation in the trunk imbalance (7.35 mm ±0.89). Lateral deviation was comparable for all age groups and genders measuring a mean value of 4.8 mm (SD ±0.58). Trunk inclination did not show any significant differences (P>0.05) between the age groups in boys or girls. Girls' inclination was 2.53°±1.96 with a tendency to decreasing angles by age and slightly smaller compared to boys (2.98°±2.18) (Table 2).
Table 2. Mean and standard deviation (SD) for the spine and pelvic parameters. The mean trunk imbalance varied only slightly between the age groups and the lateral deviation was comparable for all age groups and genders. In addition the trunk inclination showed no significant difference between the age groups. There was no significant difference found for pelvic tilt, torsion and inclination between the age groups and gender.
| Trunk parameters | Pelvic parameters | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Age group (years) | Inclination (mm) | SD | Imbalance (mm) | SD | Lateral deviation (mm) | SD | Tilt (mm) | SD | Inclination | SD | Torsion | SD |
| Girls | 6–6.9 | 3.4 | 2.3 | 6.49 | 4.63 | 4.5 | 2.1 | 2.39 | 1.8 | 20.07° | 6.48 | 1.39° | 1.05 |
| 7–7.9 | 2.9 | 2.3 | 5.09 | 3.8 | 4.7 | 2.3 | 2.59 | 2.34 | 18.31° | 5.63 | 2.15° | 1.53 | |
| 8–8.9 | 2.5 | 1.7 | 5.3 | 4.14 | 4.8 | 2.3 | 3.46 | 2.78 | 18.6° | 6.22 | 1.35° | 1.28 | |
| 9–9.9 | 1.7 | 1.6 | 6.77 | 4.47 | 4.7 | 2.3 | 2.6 | 1.94 | 20.81° | 4.12 | 1.92° | 1.55 | |
| 10–10.9 | 2.2 | 1.9 | 5.59 | 4.17 | 6.3 | 4.1 | 3.05 | 1.74 | 21.41° | 3.36 | 1.07° | 1.06 | |
| Mean | 2.6 | 2.1 | 5.68 | 4.16 | 4.9 | 2.6 | 2.79 | 2.19 | 19.68° | 5.45 | 1.66° | 1.38 | |
| SD | 0.66 | - | 0.74 | - | 0,74 | - | 0.43 | - | 1.35° | - | 0.44° | - | |
| Boys | 6–6.9 | 2.7 | 2 | 8.79 | 4.99 | 4.1 | 2.4 | 2.51 | 2.22 | 19.23° | 4.86 | 1.38° | 1.25 |
| 7–7.9 | 3.1 | 2.4 | 7.29 | 5.27 | 4.4 | 2.1 | 2.78 | 2 | 19.01° | 7.19 | 1.71° | 1.8 | |
| 8–8.9 | 2.9 | 2.2 | 7.63 | 5.52 | 5.2 | 2.8 | 2.48 | 1.69 | 19.22° | 5.57 | 1.33° | 1.25 | |
| 9–9.9 | 2.8 | 2.1 | 6.55 | 4.56 | 4.7 | 2 | 2.7 | 2.39 | 20.82° | 7.54 | 0.72° | 0.64 | |
| 10–10.9 | 3.3 | 2.1 | 7.12 | 4.5 | 4.6 | 2.2 | 3.58 | 1.65 | 24.3° | 5.67 | 1.53° | 1.38 | |
| Mean | 3 | 2.2 | 7.35 | 5.01 | 4.7 | 2.3 | 2.71 | 1.99 | 19.91° | 6.08 | 1.39° | 1.36 | |
| SD | 0.24 | - | 0.83 | - | 0.41 | - | 0.45 | - | 2.24° | - | 0.38° | - | |
SD, standard deviation.
Pelvic position
A mean pelvic tilt of 2.75 mm (SD±0.44) for all age groups and both genders was measured (Table 2). No significant differences (P>0.05) in pelvic tilt were found between the age groups. 19.8° (SD±2.24) for the pelvic inclination and 1.53° (SD±1.37) for the pelvic torsion were measured. Here also no significant differences (P>0.05) for both parameters between gender and age groups were found.
Discussion
To the best of our knowledge this study provides the first systematic analysis of spinal posture and pelvic position in children measured with a rasterstereographic device. Growth in children can be divided into three phases: infancy, childhood and puberty.12 The infancy phase extends from mid-gestation to the age of three, while the childhood phase starts at the age of three and ends with the beginning of the puberty. We have focused our interest on children in the second growth phase during childhood. We did not examine children younger than 6 years, because they were not able to follow the instructions given to stand still during measurements. Further studies will have to follow to analyse the posture of adolescents during puberty.
We used a rasterstereographic device because of its high accuracy and reliability, which was shown in multiple studies.13,14 In comparison of rasterstereography to radiographic measurements, Hackenberg et al.15 showed a good correlation of r=0.89 for the frontal deviation in subjects even with scoliosis. Good reliability was also found by Goh,16 who analysed healthy subjects. Because of a strong correlation (r=0.99) between the two lumbar dimples (DR and DL) to the underlying posterior superior iliac spine,11 rasterstereography can also be used to determine the pelvic position.17 Compared to other methods, rasterstereography has several advantages, especially for back screenings and follow-up studies.6 Due to the projection of visible light, subjects are not exposed to any harmful radiation. Furthermore, the shape of the back can be visualized three-dimensionally and the calculated parameters represent three-dimensional-space-coordinates.6
The overall increase in BMI, body height and weight reflects a normal development during these age periods.10 As shown in Figure 2 the parameter trunk length increases in a lesser amount than the total body height. This can be explained by the fact that most of the increase in height comes from an increase in leg length rather than from the spine itself in these age groups.18 Although the correlation between rasterstereographic measurements and standing radiographs has been shown to be high for both lateral and frontal plane values,14 sagittal parameters e.g. kyphotic and lordotic angle, cannot be compared directly because of the different technical setup of the systems. The rasterstereographic reconstruction of the spine has been shown to be good in comparison to radiographic measurements, as well as in scoliotic patients with Cobb angles up to 50°. Even there the root-mean-square was only 4 mm for lateral translation and 3° for vertebral rotation.19
So far there is no data available describing the spinal posture in children measured with a rasterstereographic device. Since there is a growing need for normative posture data because of increasing incidence of impaired posture and back pain in children,20 we consider this study a first step into further analysing and describing children's posture. The cross-sectional design of this study is a limitation that has to be kept in mind when interpreting this data. In the future a longitudinal study protocol would be beneficial to further determine the intra-individual changes in spinal posture and pelvic position during growth.
Using radiographs for the evaluation of normative data in a large collective is unethical because of the radiation exposure, which can be associated e.g. with an increased breast cancer risk as shown in patients with scoliosis.7 Therefore, we refused to conduct radiographs as a direct comparison to rasterstereographic pictures.
Since this is a pilot study we compared the found values with the present literature of radiologically/clinically measured spinal parameters and with rasterstereographic reference values of adults. In contrast to studies of Willner, Widhe and Poussa the increase of the thoracic angle in our study was only marginally pronounced in girls with the means in our collective being generally higher.2,21,22 The described differences can probably be explained by different measuring methods. Widhe e.g. used a Debrunner's kyphometer and Poussa an inclinometer to determine the sagittal angles. Although the reliability of these external-measuring devices has been reported to be satisfactory, their validity compared to radiographs measuring the Cobb angle is considered to be only acceptable for kyphotic and inferior for lordotic angles.23
Previous studies have shown that growth and age might have an influence on posture;22,24,25 e.g. Poussa et al.21 examined children between the age of eleven and fourteen and at a follow-up at 22 years and Widhe et al.2 measured children between five and six years and again at fifteen years. These studies showed that the peak height velocity occurred in girls about 2 years earlier than in boys.21 This might explain the here measured greater kyphotic angle in girls compared to boys. In studies using radiographs to measure the kyphosis according to Cobb, a major difference between the sexes in children and adolescents was not observed.26–28 Moreover, Propst-Proctor did not find an influence of age on kyphosis.28 So the kyphotic angles found in our population concur with the recent radiographic studies.27,29 Compared to Poussa et al.,21 lumbar lordosis increased slightly by age groups, more pronounced in girls than in boys. This supports the observations by Widhe, who found a progression of lumbar lordosis which was slightly more distinct in girls.2 Mac-Thiong et al. also found a trend to higher lordosis in their older age group more pronounced in girls than boys.27 The mean values and the increase between the two age groups were somewhat higher in their study compared to our population. These differences again might be due to the different study populations and methods used. In 2011 Schroeder et al. compared rasterstereographic values of adult low back pain patients with 177 healthy subjects. They found mean values of 48.2° (SD±9.0) for the kyphosis and 39.3° (SD±7.4) for lordosis in adults with a mean age of 27.1 years. These results are comparable to the values (kyphotic angle 47.1°, lordotic 42.1°) that we have found in children, suggesting that sagittal parameters might not significantly change over time.
So far only little is known about changes of the frontal parameters of the spine. Schroeder et al.30 determined trunk inclination with 12.3° (SD±17.9) in females and 10.3° (SD±16.4) in males. With values of 19.91° (SD±2.24) in females and 19.68° (SD±1.35) in males in our study, there seems to be a difference between adults and children suggesting that children might have a more upright posture. Interestingly, in our study the lateral deviation and trunk imbalance remained almost constant with increasing age.
Looking at the current literature we hardly found suitable studies, which referenced the pelvic position in children. Because of that we had to compare the results of our study with the data from Schroeder et al. in adults.30 For pelvic tilt Schroeder measured 3.45 mm (SD±2.6) comparing to 2.75 mm (SD±0.44) in our study. The pelvic torsion in Schroeder's study was 2.15° (SD±1.7) and in our study 1.53° (SD±0.41).30 By analysing both results it seems that there is no difference between adults and children for the pelvic position.
Conclusions
For the first time rasterstereographically measured values of spinal posture and pelvic position in children between 6 and 11 years have been determined. Rasterstereography seems to be reliable for the analysis of the spinal posture and pelvic position in children. Further studies would be feasible with a larger number of children in a longitudinal study protocol to gain more data concerning an age dependent development.
References
- 1.Hertzberg A. Prediction of cervical and low-back pain based on routine school health examinations. A nine- to twelve-year follow-up study. Scand J Prim Health Care. 1985;3:247–53. doi: 10.3109/02813438509013957. [DOI] [PubMed] [Google Scholar]
- 2.Widhe T. Spine: posture, mobility and pain. A longitudinal study from childhood to adolescence. Eur Spine J. 2001;10:118–23. doi: 10.1007/s005860000230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.McEvoy MP, Grimmer K. Reliability of upright posture measurements in primary school children. BMC Musculoskelet Disord. 2005;6:35. doi: 10.1186/1471-2474-6-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ohlen G, Spangfort E, Tingvall C. Measurement of spinal sagittal configuration and mobility with Debrunner's kyphometer. Spine (Phila Pa 1976) 1989;14:580–3. doi: 10.1097/00007632-198906000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Bunnell WP. An objective criterion for scoliosis screening. J Bone Joint Surg Am. 1984;66:1381–7. [PubMed] [Google Scholar]
- 6.Asamoah V, Mellerowicz H, Venus J, Klockner C. [Measuring the surface of the back. Value in diagnosis of spinal diseases] Orthopade. 2000;29:480–9. doi: 10.1007/s001320050486. [Article in Geman] [DOI] [PubMed] [Google Scholar]
- 7.Ronckers CM, Erdmann CA, Land CE. Radiation and breast cancer: a review of current evidence. Breast Cancer Res. 2005;7:21–32. doi: 10.1186/bcr970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Drerup B, Hierholzer E. Objective determination of anatomical landmarks on the body surface: measurement of the vertebra prominens from surface curvature. J Biomech. 1985;18:467–74. doi: 10.1016/0021-9290(85)90282-9. [DOI] [PubMed] [Google Scholar]
- 9.Drerup B, Hierholzer E. Automatic localization of anatomical landmarks on the back surface and construction of a body-fixed coordinate system. J Biomech. 1987;20:961–70. doi: 10.1016/0021-9290(87)90325-3. [DOI] [PubMed] [Google Scholar]
- 10.Meigen C, Keller A, Gausche R, et al. Secular trends in body mass index in German children and adolescents: a cross-sectional data analysis via CrescNet between 1999 and 2006. Metabolism. 2008;57:934–9. doi: 10.1016/j.metabol.2008.02.008. [DOI] [PubMed] [Google Scholar]
- 11.Drerup B, Hierholzer E. Movement of the human pelvis and displacement of related anatomical landmarks on the body surface. J Biomech. 1987;20:971–7. doi: 10.1016/0021-9290(87)90326-5. [DOI] [PubMed] [Google Scholar]
- 12.Okasha M, Gunnell D, Holly J, Davey Smith G. Childhood growth and adult cancer. Best Pract Res Clin Endocrinol Metab. 2002;16:225–41. doi: 10.1053/beem.2002.0204. [DOI] [PubMed] [Google Scholar]
- 13.Betsch M, Wild M, Jungbluth P, et al. Reliability and validity of 4D rasterstereography under dynamic conditions. Comput Biol Med. 2011;41:308–12. doi: 10.1016/j.compbiomed.2011.03.008. [DOI] [PubMed] [Google Scholar]
- 14.Hackenberg L, Hierholzer E, Liljenqvist U. Accuracy of rasterstereography versus radiography in idiopathic scoliosis after anterior correction and fusion. Stud Health Technol Inform. 2002;91:241–5. [PubMed] [Google Scholar]
- 15.Hackenberg L, Liljenqvist U, Hierholzer E, Halm H. [Scanning stereographic surface measurement in idiopathic scoliosis after VDS (ventral derotation spondylodesis)] Z Orthop Ihre Grenzgeb. 2000;138:353–9. doi: 10.1055/s-2000-10162. [Article in Geman] [DOI] [PubMed] [Google Scholar]
- 16.Goh S PR, Leedman PJ, Singer KP. Rasterstereographic analysis of the thoracic sagittal curvature: a reliability study. J Muscoskel Res. 1999;3:137–42. [Google Scholar]
- 17.Drerup B, Ellger B, Meyer zu Bentrup FM, Hierholzer E. [Functional rasterstereographic images. A new method for biomechanical analysis of skeletal geometry] Orthopade. 2001;30:242–50. doi: 10.1007/s001320050603. [Article in Geman] [DOI] [PubMed] [Google Scholar]
- 18.Hattori K, Hirohara T, Satake T. Body proportion chart for evaluating changes in stature, sitting height and leg length in children and adolescents. Ann Hum Biol. 2011;38:556–60. doi: 10.3109/03014460.2011.577456. [DOI] [PubMed] [Google Scholar]
- 19.Drerup B, Hierholzer E. Assessment of scoliotic deformity from back shape asymmetry using an improved mathematical model. Clin Biomech (Bristol, Avon) 1996;11:376–83. doi: 10.1016/0268-0033(96)00025-3. [DOI] [PubMed] [Google Scholar]
- 20.Erne C, Elfering A. Low back pain at school: unique risk deriving from unsatisfactory grade in maths and school-type recommendation. Eur Spine J. 2011;20:2126–33. doi: 10.1007/s00586-011-1803-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Poussa MS, Heliovaara MM, Seitsamo JT, et al. Development of spinal posture in a cohort of children from the age of 11 to 22 years. Eur Spine J. 2005;14:738–42. doi: 10.1007/s00586-004-0701-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Willner S, Johnson B. Thoracic kyphosis and lumbar lordosis during the growth period in children. Acta Paediatr Scand. 1983;72:873–8. doi: 10.1111/j.1651-2227.1983.tb09833.x. [DOI] [PubMed] [Google Scholar]
- 23.Willner S. Spinal pantograph - a non-invasive technique for describing kyphosis and lordosis in the thoraco-lumbar spine. Acta Orthop Scand. 1981;52:525–9. doi: 10.3109/17453678108992142. [DOI] [PubMed] [Google Scholar]
- 24.Hellsing E, Reigo T, McWilliam J, Spangfort E. Cervical and lumbar lordosis and thoracic kyphosis in 8, 11 and 15-year-old children. Eur J Orthod. 1987;9:129–38. doi: 10.1093/ejo/9.2.129. [DOI] [PubMed] [Google Scholar]
- 25.Nissinen M. Spinal posture during pubertal growth. Acta Paediatr. 1995;84:308–12. doi: 10.1111/j.1651-2227.1995.tb13634.x. [DOI] [PubMed] [Google Scholar]
- 26.Fon GT, Pitt MJ, Thies AC., Jr Thoracic kyphosis: range in normal subjects. AJR Am J Roentgenol. 1980;134:979–83. doi: 10.2214/ajr.134.5.979. [DOI] [PubMed] [Google Scholar]
- 27.Mac-Thiong JM, Berthonnaud E, Dimar JR, 2nd, et al. Sagittal alignment of the spine and pelvis during growth. Spine (Phila Pa 1976) 2004;29:1642–7. doi: 10.1097/01.brs.0000132312.78469.7b. [DOI] [PubMed] [Google Scholar]
- 28.Propst-Proctor SL, Bleck EE. Radiographic determination of lordosis and kyphosis in normal and scoliotic children. J Pediatr Orthop. 1983;3:344–6. doi: 10.1097/01241398-198307000-00013. [DOI] [PubMed] [Google Scholar]
- 29.Cil A, Yazici M, Uzumcugil A, et al. The evolution of sagittal segmental alignment of the spine during childhood. Spine (Phila Pa 1976) 2005;30:93–100. [PubMed] [Google Scholar]
- 30.Schroeder J, Stiller T, Mattes K. Reference data for spine shape analysis. Approaching a majority norm and deviations for unspecific low back pain. Manuelle Medizin. 2011;49:161–6. [Google Scholar]