

Abstract
Purpose
To develop a criterion for determining the topographic progression of keratoconus and to analyze the prognostic factors of progression.
Methods
Medical records of 211 eyes of 128 patients who had been followed up for more than 2 years on three or more occasions were retrospectively reviewed. Topographic parameters, including simulated K, corneal astigmatism, irregular astigmatism at 3 and 5 mm, thinnest-point pachymetry, anterior and posterior elevation, and inferior minus superior index, were used to determine topographic progression. Topographic progression was determined by the greatest kappa value associated with progression to corneal graft surgery. Eyes were separated into progressed and non-progressed groups on the basis of topographic progression. The association of clinical factors with topographic progression, including demographic factors, contact lens use, corneal erosion, and atopic history at the time of diagnosis, was assessed by logistic regression.
Results
When topographic progression was defined as five or more progressed topographic parameters, the greatest kappa value (0.354) was obtained. Ninety-four of the 211 keratoconic eyes (44.5%) were identified as topographically progressed. Age at diagnosis was significantly different between the progressed and non-progressed groups (22.2 vs. 24.7 years, p = 0.014). Logistic regression revealed that younger age at diagnosis was a risk factor for topographic progression (odds ratio, 0.948; 95% confidence interval, 0.907 to 0.991; p = 0.010).
Conclusions
We developed a criterion for evaluating topographic progression of keratoconus using diverse topographic indices. Younger age at diagnosis was associated with topographic progression of keratoconus.
Keywords: Keratoconus, Prognostic factor, Progression, Topography
Keratoconus is a progressive non-inflammatory disease of the cornea characterized by central stromal thinning that causes apical protrusion, irregular astigmatism, and impaired vision. [1,2] Although the cause of keratoconus remains unknown, many factors, including biomechanical and molecular factors and mechanical trauma, have been considered to contribute to the occurrence or progression of the disease.
One controversial aspect of previous studies is that different criteria for progression have been used, including clinical progression to penetrating keratoplasty [3-12]. Previous studies have defined the progression of keratoconus with diverse parameters, from the clinical progression that necessitates penetrating keratoplasty to several topographic indices. As corneal topography provides the most effective means of evaluating morphologic change in patients with keratoconus, several topographic parameters obtained by Orbscan II (Bausch & Lomb, Claremont, CA, USA) have been used [7,10,11], but there has been no consensus on which parameters should be used for evaluation. Furthermore, the number of parameters used in earlier studies was so limited that diverse topographic changes indicating progression of keratoconus could not be used to determine progression.
We aimed to include many of the Orbscan II parameters used in previous studies to determine keratoconus progression. We investigated changes in eight such parameters among patients followed-up for more than 2 years. Subsequently, prognostic factor analysis was used to explore factors associated with topographic progression of keratoconus.
Materials and Methods
A retrospective chart review of patients with keratoconus who visited Seoul National University Hospital from May 2005 to July 2009 was performed. Of these patients, only those who underwent follow-up examinations where Orbscan II topography was assessed over a 2-year interval on three or more occasions were included. In total, 211 eyes of 128 patients were assessed.
For all of the patients, age at diagnosis, sex, follow-up period, presence of atopic or other systemic diseases, and history of glasses/contact lens use and surgical treatment were reviewed. If a patient had been previously diagnosed with keratoconus at a separate institution, information obtained at the first time of diagnosis was used for the analysis. For the surgical treatment of keratoconus, penetrating keratoplasty was performed in patients with advanced keratoconus who had a best-corrected visual acuity of ≤20 / 200 on the Snellen chart. In addition, lens refitting, intolerance history, and duration of contact lens use (month) were investigated.
All patients underwent complete ophthalmic examination, including visual acuity measurement, slit-lamp examination, and corneal topography assessment. Keratoconus was diagnosed by identification of positive Rabinowitz indices on topographic analysis by Orbscan II as well as characteristic slit-lamp findings such as corneal thinning or protrusion, Vogt's striae, and Fleischer ring. Experienced examiners using the manufacturer-recommended acquisition protocol performed all of the Orbscan II examinations.
To review topographic parameters used in previous studies, a MEDLINE search of the English language literature from 1990 to 2010 was performed using the key words "keratoconus" and "topographic progression." Publications before 1990 were identified by reviewing the references of articles found during this search. All reports with five or more patients with keratoconus were included and the topographic parameters used to determine progression were identified for each article. A table listing the criteria for keratoconus progression in previous studies was generated. Among the topographic indices used, simulated K (SimK), astigmatism, irregularity index of 3 and 5 mm, thinnestpoint pachymetry, anterior and posterior elevation, and inferior minus superior (I-S value) asymmetry were common [3-12]. Therefore, these eight parameters were used for the topographic evaluation in this study.
These parameters were compared between the baseline and last visit for each patient. If the value at the last visit was more than that at the baseline, the topographic parameter was considered to have progressed except for thinnest-point pachymetry for which a decreased value at the last visit was considered indicative of progression. The number of progressed parameters was calculated for each patient and each case was determined to have progressed or not based on the number of progressed parameters. For example, if one case had more than a certain number of progressed parameters, the case was determined to have progressed.
The kappa (κ) statistic was used to determine the critical number of progressed parameters. When calculating the κ value, progression to keratoplasty, a previously used unambiguous criterion of keratoconus progression, was used as a standard [8,9]. The calculation of the κ value was based on the difference between the extent of agreement with the standard observed compared to the extent of agreement expected due to chance alone. In order to determine the critical number of progressed parameters for judging topographic progression (ranging from 1 to 8), the κ value was calculated, and the criterion that produced the greatest κ value was selected.
Logistic regression was performed to evaluate the prognostic factors associated with topographic progression. Age at diagnosis, sex, duration of contact lens use, follow-up period, severity at initial presentation (mild, mean K <45 diopters [D]; moderate, 45≤ mean K ≤52 D; and advanced, mean K >52 D) [11], and atopic disease were used in the analysis. A p-value of <0.05 was considered statistically significant. Statistical analyses were performed using the SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA).
Results
The demographic and clinical features of patients with and without progression are shown in Table 1. This study included 76 men and 52 women with a mean age of 23.4 ± 7.2 years (range, 12 to 48 years) at diagnosis. The mean follow-up period was 41.8 ± 13.3 months (range, 24 to 82 months). Table 2 shows the criteria for topographic progression and κ values for each criterion. As the greatest k value was obtained when topographic progression was defined using ≥5 topographic indices (κ = 0.354), this criterion was used for the evaluation of topographic progression in all patients. Topographic progression of keratoconus was thus detected in 94 (44.5%) eyes.
Table 1.
Comparison of clinical features and treatment methods between patients with and without progression
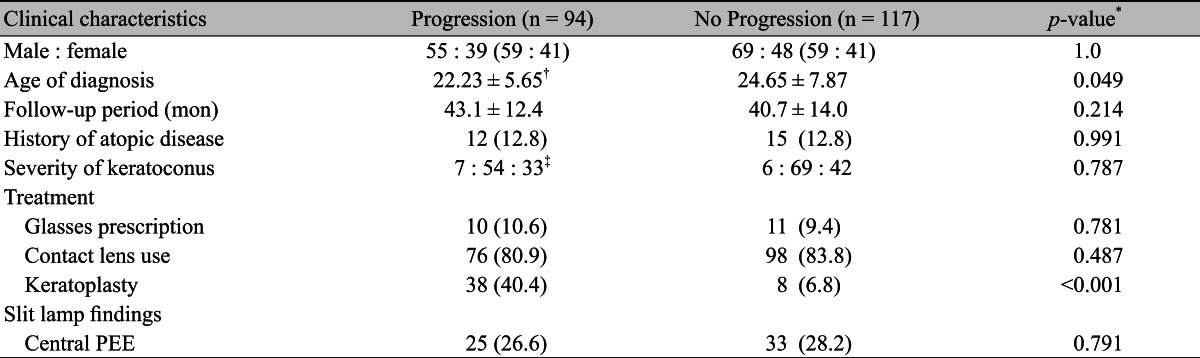
Values are presented as number (%) unless otherwise indicated.
PEE = punctate epithelial erosion; D = diopters.
*p-values were obtained by chi-square test for nominal or interval variables and Student's t-test for continuous variables; †Mean ± standard deviation; ‡Mild (mean K <45 D) : moderate (45≤ mean K ≤52 D ) : severe (mean K >52 D).
Table 2.
Criteria for topographic progression and kappa values

There was no difference in the distribution of sex and history of atopic diseases between patients with and without progression, but the mean age at diagnosis (22.23 ± 5.65 vs. 24.65 ± 7.87 years) was significantly different between the two groups (p = 0.049). The severity of keratoconus at baseline, determined by SimK, was not significantly associated with topographic progression. Furthermore, there was no significant difference in follow-up period between groups (43.1 ± 12.4 months in the progressed group vs. 40.7 ± 14.0 months in the non-progressed group).
To evaluate associations between topographic progression and treatment methods, the percentage of glasses-wearing, contact-lens-wearing, and surgically-treated patients was compared between the progressed and non-progressed groups. This comparison revealed that treatment method was not associated with topographic progression (Table 1). Furthermore, the duration of contact lens use was not significantly different between groups (36.7 ± 26.5 months in the progressed group vs. 42.4 ± 25.7 months in the non-progressed group). Moreover, the proportion of patients with keratoconus progression was not significantly different between patients who used contact lenses for more than 2 years and those who did not (41.1% vs. 55.9%). No findings on slit-lamp examination were associated with keratoconus progression. More specifically, the frequency of central punctate epithelial erosion was not significantly different between progressed and non-progressed cases (Table 1).
Table 3 shows the means and standard deviations of the Orbscan II parameters at baseline and at the last examination based on topographic progression. All topographic indices in the eyes with topographic progression showed progression at follow-up, whereas the indices, except for thinnest-point pachymetry, improved in eyes without topographic progression. The degree of progression, defined as the change of topographic values from baseline to follow-up examination, was significantly greater in the progressed group than in non-progressed group in the eight parameters (all p < 0.05).
Table 3.
Comparison of topographic parameters at baseline and follow-up examinations between patients with and without progression
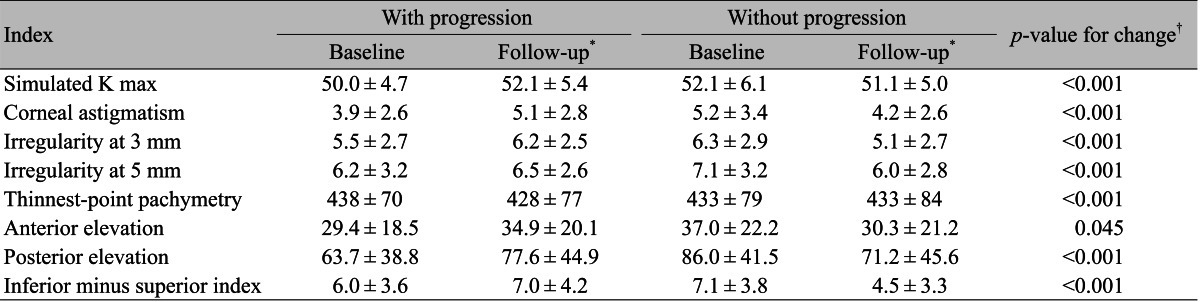
*The topographic data at the last visit were utilized for the analysis; †The change of topographic values from baseline and follow-up were compared between the two groups using Student's t-test.
Clinical characteristics such as age at diagnosis, sex, contact lens use, duration of contact lens use, the presence of central epithelial erosion on the cornea, severity of keratoconus, and a history of atopic disease were evaluated by logistic regression for association with topographic progression. Age at diagnosis was statistically significant according to the forward method of logistic regression (p = 0.010). The odds ratio (OR) was less than 1 (OR, 0.948; 95% confidence interval, 0.907 to 0.991), which indicates that younger age is a prognostic factor for topographic progression.
The results of the literature review are shown in Table 4. We identified nine studies that reported the indices used for progression and their longitudinal changes. These studies used different criteria for keratoconus progression, but some commonly defined progression in regards to corneal graft surgery [9,13].
Table 4.
Summary of criteria for keratoconus progression
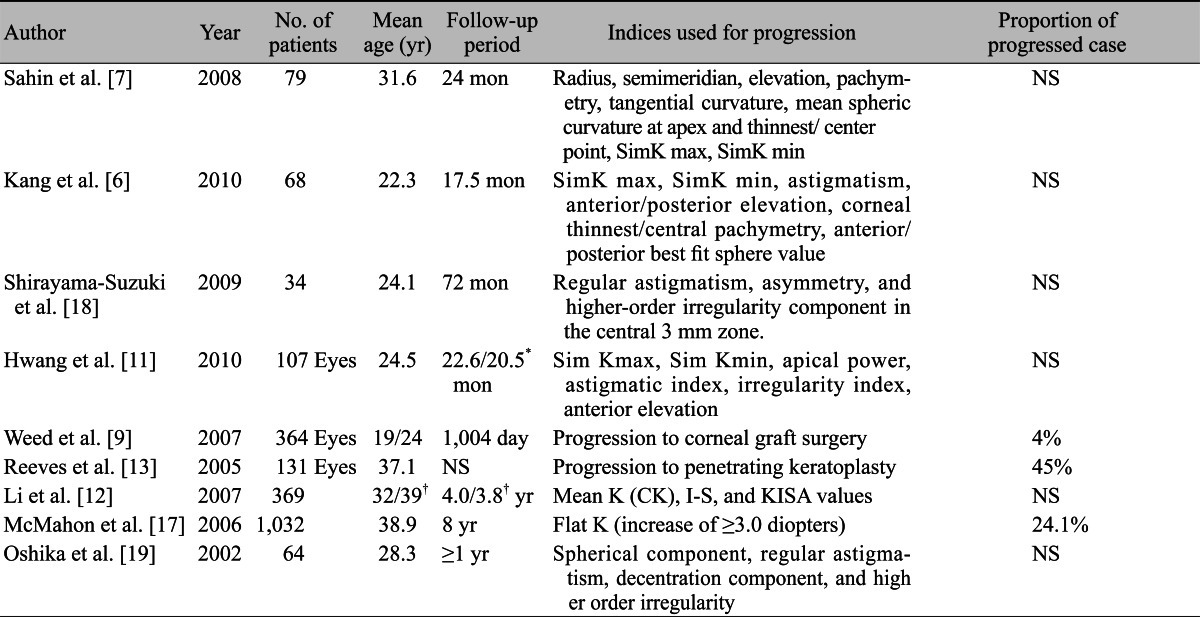
SimK = simulated K; NS = not stated; CK = central K; I-S = inferior minus superior asymmetry; KISA = (CK) × (I-S) × (SimK1 - SimK2) × (skewed radial axis) × 100/300.
*Lens-wearing group/control group; †Keratoconus relatives/normal controls.
Discussion
This study defined topographic progression in eyes with keratoconus using various topographic indices affected by the disease. Criteria that showed the greatest agreement with progression to corneal graft surgery were used to evaluate each eye with keratoconus and the factors associated with topographic progression were investigated. As a result, age at diagnosis was found to be associated with topographic progression in patients with keratoconus. Logistic regression analysis suggested that younger age is a risk factor for topographic progression.
There have been several reports of topographic progression in keratoconus [3,4,6,7,9-12]. However, all of these studies have used different criteria to evaluate progression, but these did not include diverse topographic parameters affected by keratoconus. In addition, there has been no trial to develop a criterion to determine the progression of keratoconus. We believe that such a criterion could be applied in clinical practice. Accordingly, we developed a criterion using various Orbscan II topographic parameters and subsequently validated the criterion by evaluating its agreement with a standard, progression to surgical treatment. We chose progression to surgical treatment as the standard because it has been used as a criterion of progression in previous studies [8,9] and because it is unambiguous and widely applicable in studies of keratoconus. Additionally, if a criterion was developed based on progression to corneal graft surgery, such a criterion may be useful for predicting the possibility of corneal graft surgery in the future.
In this study, the κ value obtained by defining the criterion of progression as greater than five progressed indices was 0.354. A commonly cited scale was used to interpret the κ value [14,15] and the value showed fair agreement between the criterion and progression to corneal graft surgery. As our criterion was based on progression to corneal graft surgery, the frequency of penetrating keratoplasty was significantly different between eyes with and without topographic progression. More extensive discussion of the most appropriate standard for keratoconus progression is required and further studies should develop a criterion with greater agreement.
The benefits of using a number of progressed indices are as follows. First, it is easily applied when evaluating topographic progression in clinical practice because evaluation does not require any calculation. Instead, by counting the number of progressed corneal topography parameters, clinicians can determine topographic progression in an eye with keratoconus. Second, the criterion using the number of progressed indices can minimize potential misinterpretation of progression caused by erroneous indices. Corneal topography can produce errors that can mislead interpretation of topographic progression. Furthermore, if some patients show progressive changes in only a few indices and if only these indices are used as a criterion of keratoconus progression, bias can occur. Since it is less likely that such errors would occur in multiple topographic parameters, our criterion used eight parameters identified from previous studies.
Previous studies have also suggested that age is an important factor in progression of keratoconus [12,13,16,17]. Our study also showed that younger age at diagnosis is associated with increased risk of keratoconus progression. In previous clinical studies, the mean age of patients differed (Table 4), therefore in addition to other criteria for progression, age should be carefully considered in patients with keratoconus when interpreting data. In clinical practice, age at diagnosis should be carefully considered and precautions against progression should be taken for younger patients such as adolescents and young adults. However, there might be temporal difference between the age of onset and that of diagnosis. This study is limited in that age of onset, a more appropriate clinical characteristic, was not analyzed. However, in order to minimize the temporal difference between the two time points, the first time at diagnosis was used to reduce bias.
In conclusion, we developed a criterion for topographic progression of keratoconus and our findings suggest that younger age at diagnosis is a prognostic factor. In clinical practice, clinicians can envisage the course of keratoconus in individual patients based on age. Our criterion can predict the need for surgical treatment in the future and thus facilitate decisions on surgical treatment.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28:293–322. doi: 10.1016/0039-6257(84)90094-8. [DOI] [PubMed] [Google Scholar]
- 2.Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:297–319. doi: 10.1016/s0039-6257(97)00119-7. [DOI] [PubMed] [Google Scholar]
- 3.Caporossi A, Mazzotta C, Baiocchi S, Caporossi T. Long-term results of ribof lavin ultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena Eye Cross Study. Am J Ophthalmol. 2010;149:585–593. doi: 10.1016/j.ajo.2009.10.021. [DOI] [PubMed] [Google Scholar]
- 4.El-Raggal TM. Ribof lavin-ultraviolet a corneal cross-linking for keratoconus. Middle East Afr J Ophthalmol. 2009;16:256–259. doi: 10.4103/0974-9233.58418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ertan A, Ozkilic E. Effect of age on outcomes in patients with keratoconus treated by Intacs using a femtosecond laser. J Refract Surg. 2008;24:690–695. doi: 10.3928/1081597X-20080901-08. [DOI] [PubMed] [Google Scholar]
- 6.Kang YS, Park YK, Lee JS, et al. The effect of the YK lens in keratoconus. Ophthalmic Physiol Opt. 2010;30:267–273. doi: 10.1111/j.1475-1313.2010.00724.x. [DOI] [PubMed] [Google Scholar]
- 7.Sahin A, Yildirim N, Basmak H. Two-year interval changes in Orbscan II topography in eyes with keratoconus. J Cataract Refract Surg. 2008;34:1295–1299. doi: 10.1016/j.jcrs.2008.04.016. [DOI] [PubMed] [Google Scholar]
- 8.Tuft SJ, Moodaley LC, Gregory WM, et al. Prognostic factors for the progression of keratoconus. Ophthalmology. 1994;101:439–447. doi: 10.1016/s0161-6420(94)31313-3. [DOI] [PubMed] [Google Scholar]
- 9.Weed KH, Macewen CJ, McGhee CN. The Dundee University Scottish Keratoconus Study II: a prospective study of optical and surgical correction. Ophthalmic Physiol Opt. 2007;27:561–567. doi: 10.1111/j.1475-1313.2007.00524.x. [DOI] [PubMed] [Google Scholar]
- 10.Kim H, Joo CK. Measure of keratoconus progression using Orbscan II. J Refract Surg. 2008;24:600–605. doi: 10.3928/1081597X-20080601-08. [DOI] [PubMed] [Google Scholar]
- 11.Hwang JS, Lee JH, Wee WR, Kim MK. Effects of multicurve RGP contact lens use on topographic changes in keratoconus. Korean J Ophthalmol. 2010;24:201–206. doi: 10.3341/kjo.2010.24.4.201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Li X, Yang H, Rabinowitz YS. Longitudinal study of keratoconus progression. Exp Eye Res. 2007;85:502–507. doi: 10.1016/j.exer.2007.06.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Reeves SW, Stinnett S, Adelman RA, Afshari NA. Risk factors for progression to penetrating keratoplasty in patients with keratoconus. Am J Ophthalmol. 2005;140:607–611. doi: 10.1016/j.ajo.2005.05.029. [DOI] [PubMed] [Google Scholar]
- 14.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174. [PubMed] [Google Scholar]
- 15.Viera AJ, Garrett JM. Understanding interobserver agreement: the kappa statistic. Fam Med. 2005;37:360–363. [PubMed] [Google Scholar]
- 16.Pouliquen Y, Forman MR, Giraud JP. Evaluation of the rapidity of progression of keratoconus by a study of the relationship between age when first detected and age at operation. J Fr Ophtalmol. 1981;4:219–221. [PubMed] [Google Scholar]
- 17.McMahon TT, Edrington TB, Szczotka-Flynn L, et al. Longitudinal changes in corneal curvature in keratoconus. Cornea. 2006;25:296–305. doi: 10.1097/01.ico.0000178728.57435.df. [DOI] [PubMed] [Google Scholar]
- 18.Shirayama-Suzuki M, Amano S, Honda N, et al. Longitudinal analysis of corneal topography in suspected keratoconus. Br J Ophthalmol. 2009;93:815–819. doi: 10.1136/bjo.2008.140012. [DOI] [PubMed] [Google Scholar]
- 19.Oshika T, Tanabe T, Tomidokoro A, Amano S. Progression of keratoconus assessed by fourier analysis of videokeratography data. Ophthalmology. 2002;109:339–342. doi: 10.1016/s0161-6420(01)00903-4. [DOI] [PubMed] [Google Scholar]