

Abstract
We report the case of a 37-year-old man with a high myopic keratoconus eye that was treated with a posterior chamber toric implantable collamer lens (ICL) in Korea. The patient had a history of contact lens intolerance and did not want to have a corneal transplantation. His uncorrected visual acuity (UCVA) and best spectacle corrected visual acuity were 0.02 and 0.4 in the left eye, respectively. Preoperatively, the manifest refraction was -12.0 -3.5 × 30A. Postoperatively, the manifest refraction was -1.75 × 180A. UCVA improved markedly after implantation. No intraoperative or postoperative complications were observed during 20 months of follow-up. Toric ICL implantation may be a possible alternative surgical option for the visual rehabilitation of high myopic astigmatism in keratoconus patients with rigid gas permeable contact lens intolerance and in patients who do not want to get a corneal transplant.
Keywords: Astigmatism, High myopia, Keratoconus, Toric implantable collamer lens
Keratoconus is a noninflammatory, progressive corneal degeneration characterized by stromal thinning and conical ectasia leading to high degree of irregular myopic astigmatism and corneal scarring [1,2]. Corneal scarring and irregular astigmatism become worse and can reduce the best-corrected visual acuity (BCVA) as the disease progresses [3]. The treatment for keratoconus depends on the stage of the disease progression and varies from spectacles or soft contact lenses to penetrating keratoplasty. Rigid gas permeable (RGP) contact lenses are the mainstay of treatment. Approximately 10% to 20% of patients with keratoconus undergo penetrating keratoplasty when RGP lenses intolerance occurs or if RGP lenses provide poor vision [4,5]. Various surgical procedures including photorefractive keratectomy, epikeratophakia, sectoral keratotomy, and lamellar keratoplasty can be considered, although they have had disappointing results [6,7]. Both the Keraring (Mediphacos, Belo Horizonte, Brazil) and Intacs (Addition Technology, Fremont, CA, USA) implantations are additional surgical options for managing keratoconus [8-10]. Corneal collagen cross-linking has been used for the management of progressive keratoconus after the first clinical study was performed by Wollensak et al. [11].
The toric implantable collamer lens (ICL; Visian ICL, STAAR Surgical, Nidau, Switzerland) is capable of correcting moderate to high astigmatism [12-14]. Although irregular astigmatism cannot be corrected, the toric ICL may be an alternative for correcting high myopic astigmatism in eyes with stable keratoconus for partial visual rehabilitation [15]. However, to our knowledge, the use of phakic toric ICL has not yet been reported in a keratoconus patient in Korea. Herein, we report the case of a keratoconus patient with high myopic astigmatism who, through a posterior chamber toric ICL, achieved partial visual rehabilitation.
The preoperative and postoperative ophthalmic examinations including uncorrected visual acuity (UCVA), best spectacle corrected visual acuity (BSCVA), manifest refraction, topographic findings, and adverse events complications were noted. The efficacy index, the ratio of postoperative UCVA to preoperative BSCVA (>1 indicates the BCVA improved postoperatively), the safety index, the ratio of postoperative BSCVA to preoperative BSCVA (>1 indicates the postoperative UCVA was better than the preoperative BSCVA) were evaluated [16].
Case Report
A 37-year-old man with keratoconus (Fig. 1A) could not tolerate RGP lens-wearing and did not want to have a corneal transplant or other corneal surgeries. He had been using RGP contact lenses in both eyes for 10 years. He was diagnosed with unilateral keratoconus of the left eye. Stable keratoconus was confirmed with refraction and corneal topography for 7 years (Fig. 1B and 1C). In the right eye, the UCVA was 0.04 and the BSCVA was 0.7 with -3.75 -3.00 × 155A. In the left eye, the UCVA was 0.02, and the BSCVA was 0.4 with -12.00 -3.50 × 30A. The corneal refractive power was 58.40 / 48.70 diopters × 117A in the left eye (Fig. 1C). With manifest refraction, a BSCVA of 0.4 was achieved. He was told that the maximal possible visual correction would be 0.4 or less because irregular astigmatism could not be corrected with toric ICL implantation. With informed consent, toric ICL implantation was performed without any surgical complications. After surgery, the manifest refraction became -0.75 × 180A with a UCVA of 0.5 and BSCVA of 0.7 at 1 month, which then shifted to +2.25 -0.50 × 180A with a UCVA of 0.4 and BSCVA of 0.7 at 9 months, and to -1.75 × 180A with a UCVA of 0.2 and BSCVA of 0.5 at 20 months. The anterior chamber depth, from the endothelium to the ICL, decreased from 2.21 mm at 1 month to 2.13 mm at 9 months follow-up, corresponding with mild corneal flattening and transient hyperopic changes (Fig. 1D), without any vault changes (Fig. 1E and 1F). At the last follow-up, 20 months after surgery, the ICL vault was decreased, resulting in mild deepening of the ACD from 2.13 mm to 2.17 mm, and the manifest refraction results finally stabilized at mild myopic astigmatism (Fig. 1G). The efficacy and safety index were 1.0 and 1.75 at 9 months and 0.5 and 1.25 at 20 months (Table 1). Postoperative contrast sensitivity was also enhanced (Fig. 1H).
Fig. 1.

(A) Anterior segment photography, arrow marking Fleischer's ring, ar rowhead marking corneal scarring. (B) Topography taken 7 years before surgery. (C) Topography before surgery shows stable keratoconus compared with Fig. 1B. The preoperative 3 mm zone irregular astigmatism was ±8.3 diopters and the central corneal thickness was 527 µm. (D) Topography taken 9 months after surgery shows stable keratoconus compared with preoperative topographies. (E) The ultrasound biomicroscopy (UBM) measurement of anterior chamber depth from the endothelium to the anterior surface of implantable collamer lens (ICL) was 2.21 mm one month after surgery. (F) The UBM measurement of anterior chamber depth from the endothelium to the anterior surface of ICL was 2.13 mm 9 months after surgery. (G) The UBM measurement of anterior chamber depth from the endothelium to the anterior surface of ICL was 2.17 mm 20 months after surgery. (H) Contrast sensitivity improved after toric ICL implantation (solid line, postoperative 1 month; dashed line, postoperative 9 months).
Table 1.
Summary of clinical data of 37-year-old male patient with keratoconus before and after toric ICL implantation
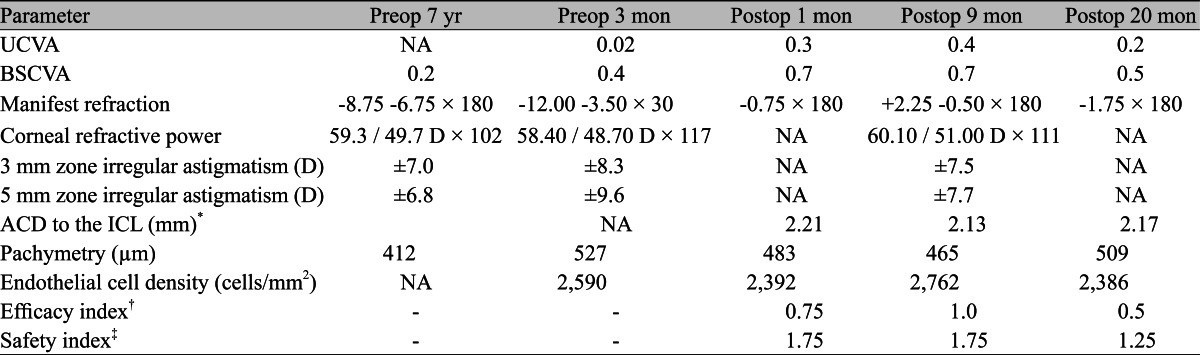
ICL = implantable collamer lens; Preop = preoperative; Postop = postoperative; UCVA = uncorrected visual acuity; BSCVA = best spectacle corrected visual acuity; D = diopters; NA = not available; ACD = anterior chamber depth.
*ACD from endothelium to the anterior surface of ICL at the final follow-up; †Postop UCVA / preop BSCVA; ‡Postop BSCVA / preop BSCVA.
Discussion
Toric ICL has been used as an alternative for the correction of high myopic astigmatism in eyes with stable keratoconus, though irregular astigmatism is a concern due to its ability to interfere with visual rehabilitation [15]. The two-step procedure of combining intrastromal corneal rings and phakic intraocular lens implantation may be another alternative treatment option for keratoconus with high myopic astigmatism. Toric ICL may have advantages in terms of expense, time, and being a one-step procedure. Toric ICL implantation can improve clinically useful vision even if perfect vision cannot be achieved in patients with advanced stable keratoconus. In our case, the patient was satisfied with partial visual rehabilitation because his daily activities could be comfortably performed with his spectacles-corrected vision with his ICL implants.
There are still issues regarding toric ICL target diopter, which may not be precisely calculated exactly in keratoconus and postoperative refractive changes due to keratoconus progression. We used the astigmatism decomposition method recommended by the manufacturer (STAAR Surgical) to perform the toric ICL power calculation [17]. Exact calculation of the target diopter, however, is more difficult in keratoconus than in other high myopic astigmatism conditions due to the difficulty of achieving a precise keratometric reading and manifest refraction. Moshirfar et al. [18] reported that phakic ICL selection for emmetropia in keratoconus eyes with high myopic astigmatism may lead to hyperopia. Our patient had a transient hyperopic shift that appeared to be associated with a suspicious progression of scarring that resulted in flattening of the cornea and subsequent shallowing of the anterior chamber depth. This hyperopic change resolved with decreasing the ICL vault and the refraction stabilized by 20 months follow-up. Despite transient refractive changes during the follow-up, the visual improvement with correction was maintained, and the patient was satisfied with the postoperative vision and the lack of postoperative complications. It is important that the patient is well informed before the surgery of possible visual fluctuations and only a partial restoration of vision.
Because toric ICL aims to correct spherical and cylindrical errors, it cannot correct a large amount of high order aberrations caused by irregular shapes of the cornea. After a toric ICL implantation, our patient still had a similar amount of high order aberrations despite correcting the high myopic astigmatism.
It is important to choose adequate candidates for toric ICL implantation. Examples include patients with RGP intolerance, stable keratoconus, or fear of corneal surgery. To select suitable candidates, correction of high myopia and astigmatism with spectacles before the surgery should be tried in the clinic.
Recently, to reduce both irregular astigmatism and high myopia, cross-linking, or corneal ring implantation combined with toric ICL, has been newly adapted for treating keratoconus. Nevertheless, our case report suggests that toric ICL implantation may be a possible alternative surgical option for the partial visual rehabilitation of high myopic astigmatism in keratoconus patients with RGP contact lens intolerance who do not want to have a corneal transplant or other corneal surgeries.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28:293–322. doi: 10.1016/0039-6257(84)90094-8. [DOI] [PubMed] [Google Scholar]
- 2.Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:297–319. doi: 10.1016/s0039-6257(97)00119-7. [DOI] [PubMed] [Google Scholar]
- 3.Tuft SJ, Moodaley LC, Gregory WM, et al. Prognostic factors for the progression of keratoconus. Ophthalmology. 1994;101:439–447. doi: 10.1016/s0161-6420(94)31313-3. [DOI] [PubMed] [Google Scholar]
- 4.Lass JH, Lembach RG, Park SB, et al. Clinical management of keratoconus: a multicenter analysis. Ophthalmology. 1990;97:433–445. doi: 10.1016/s0161-6420(90)32569-1. [DOI] [PubMed] [Google Scholar]
- 5.Brierly SC, Izquierdo L, Jr, Mannis MJ. Penetrating keratoplasty for keratoconus. Cornea. 2000;19:329–332. doi: 10.1097/00003226-200005000-00014. [DOI] [PubMed] [Google Scholar]
- 6.Sekundo W, Stevens JD. Surgical treatment of keratoconus at the turn of the 20th century. J Refract Surg. 2001;17:69–73. doi: 10.3928/1081-597X-20010101-09. [DOI] [PubMed] [Google Scholar]
- 7.Jhanji V, Sharma N, Vajpayee RB. Management of keratoconus: current scenario. Br J Ophthalmol. 2011;95:1044–1050. doi: 10.1136/bjo.2010.185868. [DOI] [PubMed] [Google Scholar]
- 8.Kubaloglu A, Cinar Y, Sari ES, et al. Comparison of 2 intrastromal corneal ring segment models in the management of keratoconus. J Cataract Refract Surg. 2010;36:978–985. doi: 10.1016/j.jcrs.2009.12.031. [DOI] [PubMed] [Google Scholar]
- 9.Colin J, Malet FJ. Intacs for the correction of keratoconus: two-year follow-up. J Cataract Refract Surg. 2007;33:69–74. doi: 10.1016/j.jcrs.2006.08.057. [DOI] [PubMed] [Google Scholar]
- 10.Rabinowitz YS. INTACS for keratoconus. Int Ophthalmol Clin. 2010;50:63–76. doi: 10.1097/IIO.0b013e3181e21b76. [DOI] [PubMed] [Google Scholar]
- 11.Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135:620–627. doi: 10.1016/s0002-9394(02)02220-1. [DOI] [PubMed] [Google Scholar]
- 12.Sanders DR, Schneider D, Martin R, et al. Toric implantable collamer lens for moderate to high myopic astigmatism. Ophthalmology. 2007;114:54–61. doi: 10.1016/j.ophtha.2006.08.049. [DOI] [PubMed] [Google Scholar]
- 13.Chang J, Lau S. Toric implantable collamer lens for high myopic astigmatic Asian eyes. Ophthalmology. 2009;116:2340–2347. doi: 10.1016/j.ophtha.2009.04.053. [DOI] [PubMed] [Google Scholar]
- 14.Kamiya K, Shimizu K, Aizawa D, et al. One-year follow-up of posterior chamber toric phakic intraocular lens implantation for moderate to high myopic astigmatism. Ophthalmology. 2010;117:2287–2294. doi: 10.1016/j.ophtha.2010.03.054. [DOI] [PubMed] [Google Scholar]
- 15.Kamiya K, Shimizu K, Ando W, et al. Phakic toric implantable collamer lens implantation for the correction of high myopic astigmatism in eyes with keratoconus. J Refract Surg. 2008;24:840–842. doi: 10.3928/1081597X-20081001-12. [DOI] [PubMed] [Google Scholar]
- 16.Gazieva L, Beer MH, Nielsen K, Hjortdal J. A retrospective comparison of efficacy and safety of 680 consecutive lasik treatments for high myopia performed with two generations of flying-spot excimer lasers. Acta Ophthalmol. 2011;89:729–733. doi: 10.1111/j.1755-3768.2009.01830.x. [DOI] [PubMed] [Google Scholar]
- 17.Sarver EJ, Sanders DR. Astigmatic power calculations for intraocular lenses in the phakic and aphakic eye. J Refract Surg. 2004;20:472–477. doi: 10.3928/1081-597X-20040901-10. [DOI] [PubMed] [Google Scholar]
- 18.Moshirfar M, Feilmeier MR, Kang PC. Implantation of verisyse phakic intraocular lens to correct myopic refractive error after penetrating keratoplasty in pseudophakic eyes. Cornea. 2006;25:107–111. doi: 10.1097/01.ico.0000164829.02841.ec. [DOI] [PubMed] [Google Scholar]