

Abstract
Here, we present the case of a patient with bilateral choroidal metastases with extraocular extension in one eye. Metastasis of papillary thyroid carcinoma to the uvea is extremely rare, with only 6 patients reported in the literature. A 62-year-old man with a prior history of papillary thyroid carcinoma suffered the rapid loss of vision in his right eye. He had neovascular glaucoma, total retinal detachment, and a solitary choroidal mass. A month later, his left visual acuity also decreased because of a small macular choroidal mass. The right eye was enucleated and a nodular lesion over the sclera representing extraocular extension was observed. This tumor and the intraocular lesion were composed of papillary excrescences and cystic spaces and stained positively for thyroid transcription factor 1 and thyroglobulin, all confirming the diagnosis of metastatic papillary thyroid carcinoma. The tumor in the left eye was successfully treated with diode laser transpupillary thermotherapy. The patient expired within a month as a result of widespread pulmonary metastases. Papillary thyroid carcinoma may metastasize to the uvea bilaterally, cause rapid visual function loss, erode the sclera, and may extend outside the globe similar to choroidal melanoma. This aggressive ocular involvement was associated with a dismal prognosis in our patient.
Keywords: Choroid, Neoplasm metastasis, Papillary carcinoma, Thyroid gland, Transpupillary thermotherapy
Thyroid cancer has progressively become the eighth most common malignant tumor with an annual increase rate of 4% and is incriminated in 7.7% to 10% of all malignancies found in patients between 15 and 24 years of age [1]. Despite these alarming demographic data pertaining to thyroid cancer, distant hematogenous spread to the uvea continues to be exceptionally rare. In a survey of 420 patients with uveal metastatic tumors, thyroid cancer was only documented in 2 cases [2]. Two recent publications found 15 cases of metastatic thyroid carcinoma to the eye in the literature, the majority of these being follicular thyroid carcinomas [3,4]. We describe a patient with papillary thyroid carcinoma who had bilateral uveal metastases and extraocular extension of the tumor in one eye. The malignancy had an unusually aggressive clinical course following the appearance of choroidal metastases.
Case Report
A 62-year-old man presented with a red and painful right eye. He had begun to experience visual problems 8 months earlier, which rapidly deteriorated in the last 2 months. He had undergone a total thyroidectomy for papillary carcinoma 4 years prior. Fifteen months later, metastatic disease was discovered in his sternum and he received iodine-131 therapy. His condition remained stable thereafter.
Upon examination, his visual acuity was light perception in the right eye and 20 / 25 in the left eye. Microcystic corneal edema, a fixed and dilated pupil, and rubeosis iridis were found in the right eye. There was total serous retinal detachment and the intraocular pressure was 45 mmHg (applanation). Ocular ultrasonography demonstrated a single choroidal lesion with a basal diameter measuring 11 mm and a thickness of 6 mm in the right eye (Fig. 1A).
Fig. 1.

(A) B-scan ultrasonogram of the right eye before enucleation shows the intraocular tumor with orbital shadowing which probably corresponds to the extraocular extension. (B) The enucleated right eye had a pigmented scleral nodule on the superior part.
The left eye was normal. The right eye was enucleated, as there were no prospects of recovering useful vision. A dark, well-encapsulated scleral nodule was noted over the enucleated globe (Fig. 1B). A month later, the patient's visual acuity in the left eye decreased to 20 / 200 with the new development of a solitary, reddish-pink choroidal mass that measured 6 × 4.5 mm in basal dimensions and 1.5 mm in thickness, superior to the fovea and within the temporal vascular arcades (Fig. 2A). There was minimal subretinal fluid over the lesion. This tumor was treated with a single session of transpupillary thermotherapy using a 0.5 mm spot size, 500 mW power, and 29 overlapping spots each lasting 45 seconds. Six weeks later, the tumor in the left eye totally disappeared without any improvement in the patient's visual acuity (Fig. 2B). Evidence for widespread metastatic involvement of the lungs was confirmed a month later and he expired from respiratory complications.
Fig. 2.
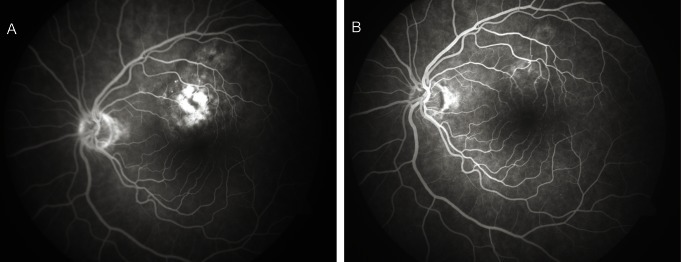
(A) Mid-phase fluorescein angiogram of the left fundus showing the relatively well-delineated lesion above the fovea with patchy areas of hyperfluorescence, before transpupillary thermotherapy. (B) Post-treatment early mid-phase fluorescein angiogram demonstrates the almost complete resolution of the lesion.
Histopathological examination of the eye revealed that the choroidal tumor was composed of papillary excrescences and cystic spaces (Fig. 3A). The papillae were covered by columnar and cuboidal cells with eosinophilic cytoplasms. These cells had elongated nuclei and irregular nuclear contour. In one area, the sclera was eroded in full thickness and tumor cells gained access into the sub-Tenon's space. Immunohistopathological studies showed strong signals of thyroglobulin and thyroid transcription factor 1 (Fig. 3B).
Fig. 3.

Histopathological view of the specimen showing (A) papillary excrescences typical of papillary thyroid carcinoma (H&E, ×40) and (B) strong thyroid transcription factor 1 signals (×40).
Discussion
Papillary carcinoma constitutes 80% of all thyroid cancers in the human [1]. Forty-two percent of metastases develop in the regional lymph nodes. Hematogenous distant metastases occur in only 10% of patients, mainly to the lungs, bones, and brain [1,4]. Ocular metastasis is distinctly unusual and when present, the orbit is more commonly affected than the intraocular tissues [5].
Uveal metastatic thyroid carcinoma was found in patients who had their primary cancer diagnosed and treated for an average of 9.9 years (range, 4 to 30 years) [4-9]. In 2 cases, uveal metastases were the initial presentations of the papillary thyroid cancer [3,8]. Reported ocular signs and symptoms included a sudden loss of visual acuity, loss of color discrimination, visual field defects, and light flashes [3-9]. The majority of these patients had a solitary, amelanotic, orange-yellow choroidal mass sometimes associated with serous or hemorrhagic retinal detachment [3-7,9]. Three patients had bilateral choroidal involvement [3,7,8]. Extraocular extension, very similar to our case, was found only once, in a blind and painful eye [8].
Because a very limited numbers of patients have been reported, no data exist describing the best and most effective treatment of this condition. External beam radiotherapy, I131 ablation therapy and enucleation have been employed based on the extent of the tumor, the potential for visual improvement and the systemic status of the patient [3-9]. In our patient, transpupillary thermotherapy resulted in satisfactory regression of the solitary choroidal metastatic tumor in the left eye.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Rosenbaum MA, McHenry CR. Contemporary management of papillary carcinoma of the thyroid gland. Expert Rev Anticancer Ther. 2009;9:317–329. doi: 10.1586/14737140.9.3.317. [DOI] [PubMed] [Google Scholar]
- 2.Shields CL, Shields JA, Gross NE, et al. Survey of 520 eyes with uveal metastases. Ophthalmology. 1997;104:1265–1276. doi: 10.1016/s0161-6420(97)30148-1. [DOI] [PubMed] [Google Scholar]
- 3.Arat YO, Boniuk M. Red lesions of the iris, choroid, and skin secondary to metastatic carcinoma of the thyroid: a review. Surv Ophthalmol. 2007;52:523–528. doi: 10.1016/j.survophthal.2007.06.006. [DOI] [PubMed] [Google Scholar]
- 4.Bucerius J, Meyka S, Michael B, et al. Papillary thyroid carcinoma with an uncommon spread of hematogenous metastases to the choroid and the skin. J Natl Med Assoc. 2008;100:104–107. doi: 10.1016/s0027-9684(15)31183-4. [DOI] [PubMed] [Google Scholar]
- 5.Slamovits TL, Mondzelewski JP, Kennerdell JS. Thyroid carcinoma metastatic to the globe. Br J Ophthalmol. 1979;63:169–172. doi: 10.1136/bjo.63.3.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ahmadi MA, Nicholes D, Esmaeli B. Late choroidal metastasis secondary to papillary thyroid carcinoma. Am J Ophthalmol. 2001;132:796–798. doi: 10.1016/s0002-9394(01)01129-1. [DOI] [PubMed] [Google Scholar]
- 7.Avram AM, Gielczyk R, Su L, et al. Choroidal and skin metastases from papillary thyroid cancer: case and a review of the literature. J Clin Endocrinol Metab. 2004;89:5303–5307. doi: 10.1210/jc.2004-0757. [DOI] [PubMed] [Google Scholar]
- 8.Singh U, Kaushik S, Pandav SS, et al. Papillary carcinoma thyroid presenting as a choroidal metastasis: report of a case and brief review of literature. Indian J Ophthalmol. 2003;51:81–83. [PubMed] [Google Scholar]
- 9.Yunta Abarca PJ, Ponce JL, Prieto M, et al. Papillary thyroid carcinoma that metastasised to the choroid. Eur J Surg. 1999;165:998–999. doi: 10.1080/110241599750008161. [DOI] [PubMed] [Google Scholar]